You might also like
- MR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHDocument24 pagesMR - INCOVIT - 30521 - Probable Covid-Complicated UTI - SAHIka AyuNo ratings yet
- Case Presentation On Ischemic Stroke: G.Hari Prakash Pharm.D InternDocument22 pagesCase Presentation On Ischemic Stroke: G.Hari Prakash Pharm.D InterngeethaNo ratings yet
- Simple Tools in HD MonitoringDocument66 pagesSimple Tools in HD MonitoringGHALEB A. AlmekhlafiNo ratings yet
- Morning Report: 2 March 2021 Night ShiftDocument16 pagesMorning Report: 2 March 2021 Night ShiftWilujeng AnggrainiNo ratings yet
- Cardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIDocument30 pagesCardiogenic Shock Complicating Acute Myocardial Infarction PPT FIKRIFikriYTNo ratings yet
- MR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDocument23 pagesMR Tengah Incovit - Ketut - 240621 - Covid Severe + DMDr. Surya Abadi KristyoadiNo ratings yet
- MR Aki Joe CorporationDocument58 pagesMR Aki Joe CorporationrizkiNo ratings yet
- TN KoesrinDocument5 pagesTN KoesrinCristian RajagukgukNo ratings yet
- Mortality Meet CASEDocument29 pagesMortality Meet CASEArnavjyoti DasNo ratings yet
- 26 Juni 2020 Materi WebinarDocument116 pages26 Juni 2020 Materi WebinarELLY MAYANGSARINo ratings yet
- Diabetis Mellitus Ischemic Heart Disease Chronic Renal FailureDocument24 pagesDiabetis Mellitus Ischemic Heart Disease Chronic Renal FailureBharath GowdaNo ratings yet
- Amprahan HCU Kamis Pagi, 15 Februari 2024Document6 pagesAmprahan HCU Kamis Pagi, 15 Februari 2024alfaz zamzamiNo ratings yet
- Pomr Belakang Vin CKDDocument25 pagesPomr Belakang Vin CKDPHOENIX LUNANo ratings yet
- Laporan Jaga Bangsal Rabu, 26 Desember 2018Document8 pagesLaporan Jaga Bangsal Rabu, 26 Desember 2018oyomziicNo ratings yet
- POMR Satiti Acute CholangitisDocument30 pagesPOMR Satiti Acute CholangitisIka AyuNo ratings yet
- ABG Final-MAMC PG Assembly 18Document69 pagesABG Final-MAMC PG Assembly 18DrLalit Kumar SamantarayNo ratings yet
- Ward Report 4-5-2017Document9 pagesWard Report 4-5-2017rezaNo ratings yet
- Laporan Icu 16 Okt 2016Document21 pagesLaporan Icu 16 Okt 2016gabbbbbbbbyNo ratings yet
- กรณีศึกษา (case study) อ.เพ็ญนภาDocument8 pagesกรณีศึกษา (case study) อ.เพ็ญนภาKanisthita ChutikittidechapatNo ratings yet
- Acidosis Alkalosis BiochemistryDocument31 pagesAcidosis Alkalosis BiochemistryliyaNo ratings yet
- Ward Report 2-5-2018 MAPDocument10 pagesWard Report 2-5-2018 MAPIvanRaykaNo ratings yet
- DUTY SDH + CKDDocument6 pagesDUTY SDH + CKDadelia putri wirandaniNo ratings yet
- Pomr Belakang Vin CKDDocument25 pagesPomr Belakang Vin CKDPHOENIX LUNANo ratings yet
- Acidosis Alkalosis BiochemistryDocument28 pagesAcidosis Alkalosis BiochemistryDocSam048No ratings yet
- Duty Report: June 2th, 2021Document13 pagesDuty Report: June 2th, 2021SarahNo ratings yet
- MORNING REPORT Monday 2022Document15 pagesMORNING REPORT Monday 2022Thaharatin GizaNo ratings yet
- Stemi Anterior ExtensiveDocument29 pagesStemi Anterior ExtensiveNur Abidatul FitriaNo ratings yet
- Duty Report: June 2th, 2021Document12 pagesDuty Report: June 2th, 2021SarahNo ratings yet
- กรณีศึกษา (case study) อ.เพ็ญนภาDocument8 pagesกรณีศึกษา (case study) อ.เพ็ญนภาKanisthita ChutikittidechapatNo ratings yet
- Template Duty ReportDocument6 pagesTemplate Duty ReportJefri SusantoNo ratings yet
- Cerebral Infarction in Risk Factor of Adenoma and Symptomatic Aortic Stenosis Case Report and Literature Reviewp PDFDocument8 pagesCerebral Infarction in Risk Factor of Adenoma and Symptomatic Aortic Stenosis Case Report and Literature Reviewp PDFFortune JournalsNo ratings yet
- Its Just HoaxDocument10 pagesIts Just HoaxArkhan HanafiNo ratings yet
- Computer-Based Scenario Biochemistry: How To Read Bloods?Document66 pagesComputer-Based Scenario Biochemistry: How To Read Bloods?Haytham KhalifaNo ratings yet
- Friday 2-2-2018 Multiple MyelomaDocument20 pagesFriday 2-2-2018 Multiple MyelomaJefri SusantoNo ratings yet
- 1 SPECIFICATION - EPOC NXS Host and Epoc Reader - 230308 - 231313Document2 pages1 SPECIFICATION - EPOC NXS Host and Epoc Reader - 230308 - 231313Muhammad Daniala SyuhadaNo ratings yet
- Ward Report Thursday, July 13 2016Document6 pagesWard Report Thursday, July 13 2016bobyNo ratings yet
- Electrical InjuryDocument6 pagesElectrical Injuryadelia putri wirandaniNo ratings yet
- OPD/CHL/ACH Page 1 of 4Document4 pagesOPD/CHL/ACH Page 1 of 4udithaireshaNo ratings yet
- Cardiogenic Shock Part 1Document36 pagesCardiogenic Shock Part 1Martin Miguel AmorNo ratings yet
- CKD CapdDocument20 pagesCKD CapdgemaNo ratings yet
- ICH Q3C (R8) - Residual Solvent: Step 2Document9 pagesICH Q3C (R8) - Residual Solvent: Step 2IsmailNo ratings yet
- Morning Report: Date: Monday, 2 November 2020Document24 pagesMorning Report: Date: Monday, 2 November 2020Ika AyuNo ratings yet
- 88'Th Ulcus FemoralisDocument21 pages88'Th Ulcus FemoralischiquitaputriNo ratings yet
- Laporan Jaga Bangsal 3-5-2017Document9 pagesLaporan Jaga Bangsal 3-5-2017rezaNo ratings yet
- Morning Report: Physician in ChargeDocument11 pagesMorning Report: Physician in ChargeImam Mi'raj SuprayogaNo ratings yet
- Correos Electrónicos 1. Optimizacion Cardiovascular, FluidosDocument29 pagesCorreos Electrónicos 1. Optimizacion Cardiovascular, FluidosKaren PMNo ratings yet
- Abg PDFDocument40 pagesAbg PDFjohn ginnNo ratings yet
- Cushings Syndrome With Bilateral Adrenal Masses: What Management?Document4 pagesCushings Syndrome With Bilateral Adrenal Masses: What Management?IJAR JOURNALNo ratings yet
- Duty Report: Sunday, 27 May 2018Document17 pagesDuty Report: Sunday, 27 May 2018HarisNo ratings yet
- Managing Covid-19 in IcuDocument77 pagesManaging Covid-19 in IcuninishahirahNo ratings yet
- PERFUSION monitoring-SYSTEMIC-ghalebDocument49 pagesPERFUSION monitoring-SYSTEMIC-ghalebGHALEB A. AlmekhlafiNo ratings yet
- Case Study On Head InjuryDocument6 pagesCase Study On Head Injurybaisakhi ghoshNo ratings yet
- Lab ReDocument5 pagesLab RePKMMH LabNo ratings yet
- POMR SATITI - Nephrotic SyndromeDocument27 pagesPOMR SATITI - Nephrotic SyndromeIka AyuNo ratings yet
- Amprahan HCU Minggu Pagi, 18 Februari 2024Document8 pagesAmprahan HCU Minggu Pagi, 18 Februari 2024alfaz zamzamiNo ratings yet
- Capillary Blood Gas (CBG)Document3 pagesCapillary Blood Gas (CBG)848magnoliaNo ratings yet
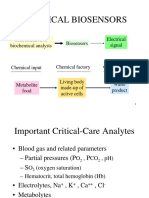
- Lect-13-Chemical BiosensorsDocument37 pagesLect-13-Chemical BiosensorsmeharNo ratings yet
- Infective endocarditis (感染性心內膜炎) : dyspnea and chest pain four days agoDocument11 pagesInfective endocarditis (感染性心內膜炎) : dyspnea and chest pain four days agoapi-19644056No ratings yet
- MR ICU COVID Senin, 27 September 2021Document8 pagesMR ICU COVID Senin, 27 September 2021wim adhitamaNo ratings yet
- Diagnosis of AsthmaDocument16 pagesDiagnosis of Asthmabrajendra singhNo ratings yet
- JPediatrCritCare2167-4903094 133710Document18 pagesJPediatrCritCare2167-4903094 133710brajendra singhNo ratings yet
- Recommendations: Ndian Ediatrics Ecember UB Head F RintDocument34 pagesRecommendations: Ndian Ediatrics Ecember UB Head F Rintbrajendra singhNo ratings yet
- App To CHR CoughDocument6 pagesApp To CHR Coughbrajendra singhNo ratings yet
- All About Fever 6Document42 pagesAll About Fever 6brajendra singhNo ratings yet
- CNS OsceDocument36 pagesCNS Oscebrajendra singhNo ratings yet
- Kuthiroly2021 Article LipoproteinLipaseDeficiencyDocument7 pagesKuthiroly2021 Article LipoproteinLipaseDeficiencybrajendra singhNo ratings yet
- Myotonia in A Child With Muscle Hypertrophy: Clinical Video Clinical Video Clinical Video Clinical Video Clinical VideoDocument1 pageMyotonia in A Child With Muscle Hypertrophy: Clinical Video Clinical Video Clinical Video Clinical Video Clinical Videobrajendra singhNo ratings yet
- 7 Ways To Minimize Jet LagDocument5 pages7 Ways To Minimize Jet LagDivyajyoti DevaNo ratings yet
- Antiarrhythmic Agent - WikipediaDocument23 pagesAntiarrhythmic Agent - WikipediaSai Jeevan SampathiraoNo ratings yet
- Axillary MethodDocument5 pagesAxillary MethodJerica Jaz F. VergaraNo ratings yet
- BPM-1200 (PATRON) /1010 (MATRON) : Operation ManualDocument76 pagesBPM-1200 (PATRON) /1010 (MATRON) : Operation ManualMd ShitolNo ratings yet
- Carganilla - Pathophysiology - Week 1Document4 pagesCarganilla - Pathophysiology - Week 1Marjorie CarganillaNo ratings yet
- Lab Exercise 8Document5 pagesLab Exercise 8Yeong-Ja KwonNo ratings yet
- Physio Preproff Questions 2022Document14 pagesPhysio Preproff Questions 2022aroobaNo ratings yet
- Lesson 28: Bionergetics Utilization of EnergyDocument25 pagesLesson 28: Bionergetics Utilization of EnergyFlorence GuzonNo ratings yet
- Nervous System NotesDocument6 pagesNervous System Notesapi-303021163No ratings yet
- Acute ConfusionDocument7 pagesAcute ConfusionYasin JazNo ratings yet
- Work Physiology: Lecture Note: IE 665 Applied Industrial ErgonomicsDocument6 pagesWork Physiology: Lecture Note: IE 665 Applied Industrial ErgonomicsAjay Kumar AgarwalNo ratings yet
- Terapi Cairan Dalam Praktek Sehari-Hari Oleh DR - Sumara Niman, SP - AnDocument49 pagesTerapi Cairan Dalam Praktek Sehari-Hari Oleh DR - Sumara Niman, SP - AnRiony GusbaniansyahNo ratings yet
- Von Gierke DiseaseDocument14 pagesVon Gierke Diseaseapi-590506208No ratings yet
- Skeletal Muscle: Organization ofDocument19 pagesSkeletal Muscle: Organization ofayesha solNo ratings yet
- Haematology NotesDocument184 pagesHaematology NotesJason royNo ratings yet
- WINSEM2017-18 - BIT1012 - ETH - CBMR301 - VL2017185004514 - Assignment I - DA - TEI - DE1 - BIT1012 - RDocument3 pagesWINSEM2017-18 - BIT1012 - ETH - CBMR301 - VL2017185004514 - Assignment I - DA - TEI - DE1 - BIT1012 - RBabbooNo ratings yet
- Sleep Medicine Reviews: Michel Billiard, Karel SonkaDocument11 pagesSleep Medicine Reviews: Michel Billiard, Karel SonkaCharlotteGraceNusiferaNo ratings yet
- Bloodstain Pattern Analysis: DR Rizwan Zafar - MBBS, DMJ Lecturer, Forensic Medicine Deptt CMH Lahore Medical CollegeDocument27 pagesBloodstain Pattern Analysis: DR Rizwan Zafar - MBBS, DMJ Lecturer, Forensic Medicine Deptt CMH Lahore Medical Collegedr rizwanNo ratings yet
- Biochem Midterms SummaryDocument5 pagesBiochem Midterms SummaryAngela CastrilloNo ratings yet
- Clinical Chemistry 2 Lec - W10 - Introduction To Endocrine GlandsDocument3 pagesClinical Chemistry 2 Lec - W10 - Introduction To Endocrine GlandsEmalchris AcadsNo ratings yet
- Rowing PDFDocument8 pagesRowing PDFkullNo ratings yet
- Tugas Bahasa Inggris Lady GagaDocument4 pagesTugas Bahasa Inggris Lady GagaGerishelaWimandaNo ratings yet
- Ineffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesDocument7 pagesIneffective Breathing Pattern Related To Shortness of Breath Possible Evidence by CuesLouie ParillaNo ratings yet
- Product BookletDocument16 pagesProduct Bookletrevanthcrazy7No ratings yet
- YgggbDocument2 pagesYgggbPopi AnggrianiNo ratings yet
- Punam Jaiswal UG-III Mechanism of Photosynthesis (Dark Reaction) C3 CycleDocument4 pagesPunam Jaiswal UG-III Mechanism of Photosynthesis (Dark Reaction) C3 CycleSanjhi JainNo ratings yet
- Physical Education and Health 2 PEDH 112 Week 11 20Document5 pagesPhysical Education and Health 2 PEDH 112 Week 11 20Maica Canete100% (1)
- Cal Dietz CVASPS 2015 PDFDocument46 pagesCal Dietz CVASPS 2015 PDFDavina Belle100% (2)
- Transfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaDocument41 pagesTransfusion in Emergency Room by DR Prannoy George, Department of Emergency Medicine, Amrita Institute of Medical Sciences, Kochi, KeralaAETCM Emergency medicineNo ratings yet
- Circulation 2 QPDocument10 pagesCirculation 2 QPAthenaNo ratings yet