You might also like
- Assignmen 2 AnswersDocument3 pagesAssignmen 2 AnswersAlasl Boby100% (3)
- DocxDocument6 pagesDocxScott Russell McGillivray89% (9)
- Asthma - Case PresentationDocument56 pagesAsthma - Case Presentationsarooah199467% (6)
- Bronchial Asthma in AEDocument14 pagesBronchial Asthma in AECharmie Lou Dadivas CelestialNo ratings yet
- Respiratory Care ModalitiesDocument5 pagesRespiratory Care ModalitiesWendy EscalanteNo ratings yet
- NCP - Ineffective Airway Clearance PediaDocument2 pagesNCP - Ineffective Airway Clearance PediaAdrian Mallar100% (6)
- Asthma!!!Document18 pagesAsthma!!!Jabbamackeez50% (2)
- Tosse Cronica em CriançasDocument17 pagesTosse Cronica em CriançasEdvaldo Pereira da Silva JúniorNo ratings yet
- A&e Case SummaryDocument1 pageA&e Case SummaryYOS HANANo ratings yet
- Asma BronkialDocument39 pagesAsma BronkialLidia WatiNo ratings yet
- OB Last Case Pres FINALDocument14 pagesOB Last Case Pres FINALLhea LaraNo ratings yet
- NURSING CARE PLAN PneumoniaDocument38 pagesNURSING CARE PLAN PneumoniaLuna JadeNo ratings yet
- Asthma Case Report FinalDocument6 pagesAsthma Case Report FinalJiaYee GoNo ratings yet
- Paediatric Respiratory History and Examination: DR Montaha AL-Iede MD, FRACP, DCHDocument35 pagesPaediatric Respiratory History and Examination: DR Montaha AL-Iede MD, FRACP, DCHRasha Al MousaNo ratings yet
- Bronchiolitis ScriptDocument6 pagesBronchiolitis ScriptAhmed RmelahNo ratings yet
- BronchiolitisDocument7 pagesBronchiolitisNader SmadiNo ratings yet
- Clinical Case Logs ReportDocument14 pagesClinical Case Logs ReportSeth Therizwhiz RockerfellaNo ratings yet
- Pneumonia Lung CoughDocument7 pagesPneumonia Lung Coughserai maramaNo ratings yet
- Childhood Asthma Research PaperDocument4 pagesChildhood Asthma Research Paperaflbtjglu100% (1)
- Broncho Pneumonia CaseDocument52 pagesBroncho Pneumonia CaseprsentNo ratings yet
- Asthma - Child - Discharge: When You're in The HospitalDocument15 pagesAsthma - Child - Discharge: When You're in The HospitalJu Lie AnnNo ratings yet
- Approach Child With Recurrent WheezeDocument41 pagesApproach Child With Recurrent Wheezecristina_zaharia865440No ratings yet
- Case PresentationDocument18 pagesCase PresentationNoli Galope IINo ratings yet
- Bronchial Asthma in Acute Exacerbation - FinalDocument17 pagesBronchial Asthma in Acute Exacerbation - Finalmary_sulit_150% (2)
- Chronic Cough In Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandChronic Cough In Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- I Can'T Breathe If Breathing Is Without: Bronchial AsthmaDocument33 pagesI Can'T Breathe If Breathing Is Without: Bronchial AsthmaklamorenaNo ratings yet
- Acute Bronchitis... The OneDocument35 pagesAcute Bronchitis... The One'mYk FavilaNo ratings yet
- Pediatric Asthma ManagementDocument81 pagesPediatric Asthma Managementmartinbsas100% (9)
- Ecologic ModelDocument3 pagesEcologic ModelHazel Regencia RodriguezNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) Is An Umbrella Term Used ToDocument21 pagesChronic Obstructive Pulmonary Disease (COPD) Is An Umbrella Term Used ToFatima Mae GarciaNo ratings yet
- Case Study Asthma Group 2Document17 pagesCase Study Asthma Group 2Kennedy PelicoNo ratings yet
- The Everything Parent's Guide to Children with Asthma: Professional advice to help your child manage symptoms, be more active, and breathe betterFrom EverandThe Everything Parent's Guide to Children with Asthma: Professional advice to help your child manage symptoms, be more active, and breathe betterNo ratings yet
- Asthma: A troubleshooting guide to common childhood ailmentsFrom EverandAsthma: A troubleshooting guide to common childhood ailmentsRating: 3 out of 5 stars3/5 (1)
- AEBADocument6 pagesAEBAAtirah AaNo ratings yet
- Pediatrics Case StudiesDocument32 pagesPediatrics Case StudiesprinceejNo ratings yet
- Bronchial AsthmaDocument22 pagesBronchial AsthmaJheric SbNo ratings yet
- Asthma and Cystic Fibrosis: Chinchu MDocument38 pagesAsthma and Cystic Fibrosis: Chinchu MChinchu MohanNo ratings yet
- Pulmonology - Cases With AnswersDocument4 pagesPulmonology - Cases With AnswersSimran PiñheiroNo ratings yet
- Name: Muhib Abdullah Karim S T U D e N T I D: 2 1 1 1 6 2 9 6 3 0 Course: Introduction To Public Health Faculty: AFC Section: 6Document11 pagesName: Muhib Abdullah Karim S T U D e N T I D: 2 1 1 1 6 2 9 6 3 0 Course: Introduction To Public Health Faculty: AFC Section: 6Nazifa IbnatNo ratings yet
- Signs and Symptoms: MicroorganismsDocument4 pagesSigns and Symptoms: MicroorganismsNikki P. NarteNo ratings yet
- Patient Education: Asthma Symptoms and Diagnosis in Children (Beyond The Basics)Document8 pagesPatient Education: Asthma Symptoms and Diagnosis in Children (Beyond The Basics)Fitria Ummu HabibahNo ratings yet
- Diagnosis of Asthma: Following Initial Assessment: Without Airflow ObstructionDocument5 pagesDiagnosis of Asthma: Following Initial Assessment: Without Airflow ObstructionebookdrNo ratings yet
- TCP PneumoniaDocument6 pagesTCP PneumoniaAnonymous FgT04krgymNo ratings yet
- Assessing and Managing Wheezing in Preschool ChildrenDocument8 pagesAssessing and Managing Wheezing in Preschool ChildrenEndy Widya PutrantoNo ratings yet
- Gina Pocket 2009 Pediatrico Unlocked)Document21 pagesGina Pocket 2009 Pediatrico Unlocked)Anonymous L9qkHGXNo ratings yet
- BronchiolitisDocument7 pagesBronchiolitislisa.aschauerNo ratings yet
- Asthma & PneumoniaDocument5 pagesAsthma & PneumoniaRenjie ElizardeNo ratings yet
- 4 Bronchial AsthmaDocument9 pages4 Bronchial Asthmashanfiza_92No ratings yet
- What Is AsthmaDocument5 pagesWhat Is AsthmajayrizNo ratings yet
- What Is AsthmaDocument5 pagesWhat Is AsthmajayrizNo ratings yet
- 2 History Is Not His StoryDocument424 pages2 History Is Not His StorydrsourabhsinghNo ratings yet
- Recurrent Wheeze in Pre-School Children: Respiratory MedicineDocument5 pagesRecurrent Wheeze in Pre-School Children: Respiratory MedicinejprakashjjNo ratings yet
- 01 Pediatric Clinics - February2009Document291 pages01 Pediatric Clinics - February2009Tessa CruzNo ratings yet
- Homeopathic Treatment For AsthmaDocument4 pagesHomeopathic Treatment For AsthmaDr Rangadhar SatapathyNo ratings yet
- PEDIATRIC HEALTH NURSING BOOK الجزء الثاني اطفالDocument47 pagesPEDIATRIC HEALTH NURSING BOOK الجزء الثاني اطفالSimaNo ratings yet
- Casestudy 5Document14 pagesCasestudy 5krystelle jade labineNo ratings yet
- Bronchopneumonia - MedscapeDocument7 pagesBronchopneumonia - MedscapecleoaerNo ratings yet
- The Complete Asthma Guide: An Asthma book for adults and children, that teaches how to be asthma free naturally with the right therapeutic diets, medications & alternative herbal therapiesFrom EverandThe Complete Asthma Guide: An Asthma book for adults and children, that teaches how to be asthma free naturally with the right therapeutic diets, medications & alternative herbal therapiesNo ratings yet
- Case Study PnuemoniaDocument10 pagesCase Study PnuemoniaKyle B. Nacionales Ü100% (1)
- Pneumonia Is A Condition That Causes The Lungs To Become Inflamed As A Result of A BacterialDocument3 pagesPneumonia Is A Condition That Causes The Lungs To Become Inflamed As A Result of A BacterialDhonnalyn Amene CaballeroNo ratings yet
- Asthma InformationDocument10 pagesAsthma InformationSheen aballeNo ratings yet
- Trinity University of Asia St. Luke'S College of Nursing Case Study (Opd) NAME: Marie Deborah Kay B. Chakas CASE: Pneumonia (Pedia)Document19 pagesTrinity University of Asia St. Luke'S College of Nursing Case Study (Opd) NAME: Marie Deborah Kay B. Chakas CASE: Pneumonia (Pedia)MARIE DEBORAH KAY CHAKASNo ratings yet
- Anatomy-Ms Respi NeuroDocument10 pagesAnatomy-Ms Respi NeuroImmah PinedaNo ratings yet
- Letter of Invitation For The ReactorDocument2 pagesLetter of Invitation For The ReactorImmah PinedaNo ratings yet
- BackSpine NotesDocument9 pagesBackSpine NotesImmah PinedaNo ratings yet
- BackSpine NotesDocument9 pagesBackSpine NotesImmah PinedaNo ratings yet
- Compre Test Blueprint April 2024Document1 pageCompre Test Blueprint April 2024Immah PinedaNo ratings yet
- Hemostasis and Hemotherapy - Pineda (April Rotator)Document31 pagesHemostasis and Hemotherapy - Pineda (April Rotator)Immah PinedaNo ratings yet
- Pineda I Meta AnaDocument5 pagesPineda I Meta AnaImmah PinedaNo ratings yet
- October ActivitiesDocument2 pagesOctober ActivitiesImmah PinedaNo ratings yet
- HeadNeck NotesDocument10 pagesHeadNeck NotesImmah PinedaNo ratings yet
- Suspected Side EffectsDocument2 pagesSuspected Side EffectsImmah PinedaNo ratings yet
- Sample Peer Assessment Form For Collaborative ReportDocument1 pageSample Peer Assessment Form For Collaborative ReportImmah PinedaNo ratings yet
- Project ProposalDocument3 pagesProject ProposalImmah Pineda100% (1)
- How To Survive Sir Teod: Immah Marie R. Pineda, PTRPDocument11 pagesHow To Survive Sir Teod: Immah Marie R. Pineda, PTRPImmah PinedaNo ratings yet
- Special Tests: Upper Extremity: Jrooz Review CenterDocument56 pagesSpecial Tests: Upper Extremity: Jrooz Review CenterImmah PinedaNo ratings yet
- O-P Coaching NotesDocument7 pagesO-P Coaching NotesImmah PinedaNo ratings yet
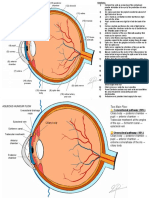
- ANATOMY OF THE EYE (Pineda, Immah)Document2 pagesANATOMY OF THE EYE (Pineda, Immah)Immah PinedaNo ratings yet
- WORKOUT ProgramDocument3 pagesWORKOUT ProgramImmah PinedaNo ratings yet
- Appraising An Article On Prognosis Clinical Scenario I. Appraising DirectnessDocument5 pagesAppraising An Article On Prognosis Clinical Scenario I. Appraising DirectnessImmah PinedaNo ratings yet
- Letter of Request - Daropa Drainage RepairDocument1 pageLetter of Request - Daropa Drainage RepairImmah Pineda100% (1)
- Nursing Care Plan: Cystic FibrosisDocument4 pagesNursing Care Plan: Cystic FibrosisYael EzraNo ratings yet
- Intensive Care Ventilator MV200: Safety - Reliability - ComfortDocument7 pagesIntensive Care Ventilator MV200: Safety - Reliability - ComfortFathur ArRahmanNo ratings yet
- Breathing ProcessDocument7 pagesBreathing ProcessJasmineNo ratings yet
- Trisha Faye P. Ortega BSN - 3A September 18, 2021: Anatomy and Physiology: Pre Assessment (M1: Activity1)Document7 pagesTrisha Faye P. Ortega BSN - 3A September 18, 2021: Anatomy and Physiology: Pre Assessment (M1: Activity1)Trisha Faye OrtegaNo ratings yet
- ATI MI Emmanuel ChenDocument2 pagesATI MI Emmanuel ChenemanNo ratings yet
- PHINMA University of Pangasinan College of Health Sciences Nursing Care PlanDocument2 pagesPHINMA University of Pangasinan College of Health Sciences Nursing Care PlanJoeriel MontemayorNo ratings yet
- AARC Asthma COPD GuidelineDocument5 pagesAARC Asthma COPD GuidelineMarcelo JunWeiNo ratings yet
- Anesthesia in A Patient With Reactive Airways Case FileDocument2 pagesAnesthesia in A Patient With Reactive Airways Case Filehttps://medical-phd.blogspot.comNo ratings yet
- Case Study Pneumonia)Document20 pagesCase Study Pneumonia)Jai - Ho83% (6)
- Asthma & PneumoniaDocument5 pagesAsthma & PneumoniaRenjie ElizardeNo ratings yet
- Thesis Topics For MD Respiratory MedicineDocument7 pagesThesis Topics For MD Respiratory Medicinelindseyriverakansascity100% (2)
- Pranavaha Strotas Vikar July 2008Document8 pagesPranavaha Strotas Vikar July 2008Sattu Singh100% (1)
- EX-07 - Act 1Document6 pagesEX-07 - Act 1Anisa AzkyaNo ratings yet
- Date and Time Focus: D - Received Patient On BedDocument2 pagesDate and Time Focus: D - Received Patient On BedGraphaiene Neika WacasNo ratings yet
- Assessment On Respiratory ProblemsDocument7 pagesAssessment On Respiratory ProblemsSetiaty PandiaNo ratings yet
- Research Paper Final DraftDocument9 pagesResearch Paper Final Draftapi-605105565No ratings yet
- Mechanical VentDocument24 pagesMechanical VentRochim CoolNo ratings yet
- Salt LampDocument9 pagesSalt LampShahmeer KhanNo ratings yet
- Nebulization TherapyDocument3 pagesNebulization TherapyGemalie KadilNo ratings yet
- Chapter 8 MiscellaneousDocument2 pagesChapter 8 Miscellaneousapi-3705891No ratings yet
- Student Nurses' Community: Nursing Care Plan PneumoniaDocument2 pagesStudent Nurses' Community: Nursing Care Plan PneumoniaJhasmine MocnanganNo ratings yet
- 16 Martie - Curs BPOC - SlideDocument95 pages16 Martie - Curs BPOC - Slidejonah1024No ratings yet
- ACTIVITY SHEET in SCIENCE (Respiratory System)Document2 pagesACTIVITY SHEET in SCIENCE (Respiratory System)VIRGILIO GUZONNo ratings yet
- Increased Intracranial PressureDocument3 pagesIncreased Intracranial PressureElle RosalesNo ratings yet
- The Respiratory System: " " and Complete The Following ActivitiesDocument3 pagesThe Respiratory System: " " and Complete The Following ActivitieswenukaNo ratings yet
- Coronavirus and Aerogen: To 6-Fold Compared To The Jet NebuliserDocument2 pagesCoronavirus and Aerogen: To 6-Fold Compared To The Jet NebuliserSantanu RNo ratings yet
- San Francisco St. Butuan City 8600, Region XIII Caraga, PhilippinesDocument3 pagesSan Francisco St. Butuan City 8600, Region XIII Caraga, Philippineskuro hanabusaNo ratings yet
- Course Out Line EH MSCPH LESSON 1Document42 pagesCourse Out Line EH MSCPH LESSON 1Muhubo MusseNo ratings yet