You might also like
- Summary of Suzanne Humphries & Roman Bystrianyk's Dissolving IllusionsFrom EverandSummary of Suzanne Humphries & Roman Bystrianyk's Dissolving IllusionsNo ratings yet
- REFERAT - Meassles - FirdaDocument19 pagesREFERAT - Meassles - FirdaEriza LuthfansyahNo ratings yet
- Zoonoses - 06.11.2023Document53 pagesZoonoses - 06.11.2023johnnycash5404No ratings yet
- Yellow FeverDocument11 pagesYellow FeverPriyanka TalukdarNo ratings yet
- Dengue FeverDocument7 pagesDengue FeverTabarak BhuiyanNo ratings yet
- 1-Measles (Rubeola) PDFDocument37 pages1-Measles (Rubeola) PDFمصطفى رسول هاديNo ratings yet
- Yellow FeverDocument31 pagesYellow FeverVibha AvasthiNo ratings yet
- Yellow FeverDocument26 pagesYellow Feverprofarmah615081% (16)
- Common Childhood Infections For CIDocument89 pagesCommon Childhood Infections For CIBeamlak Getachew WoldeselassieNo ratings yet
- Communicable DiseaseDocument193 pagesCommunicable DiseaseLuvastranger Auger100% (2)
- Chikungunya FeverDocument15 pagesChikungunya FeverAyomide AlayandeNo ratings yet
- Respiratory Infections: - Small Pox - Chicken Pox - TuberculosisDocument45 pagesRespiratory Infections: - Small Pox - Chicken Pox - TuberculosisNamrata SharmaNo ratings yet
- Dengue FeverDocument7 pagesDengue Feverأجيد الحازميNo ratings yet
- Meningococcal Meningitis & JE .PPTX CK Apr 2020 EditedDocument20 pagesMeningococcal Meningitis & JE .PPTX CK Apr 2020 EditedvaishnaviNo ratings yet
- Assign. Communicable DiseaseDocument25 pagesAssign. Communicable Diseasepooja banyalNo ratings yet
- Communicable Disease: Mr. Pankaj Kusum Ramdas KhuspeDocument113 pagesCommunicable Disease: Mr. Pankaj Kusum Ramdas KhuspeManisa ParidaNo ratings yet
- MEASLESDocument34 pagesMEASLESmanibharathiNo ratings yet
- Chikungunya by DR NaziaDocument37 pagesChikungunya by DR NaziaNazia ShamimNo ratings yet
- Dengue 121008123903 Phpapp02Document34 pagesDengue 121008123903 Phpapp02maharshi mNo ratings yet
- Swine Influenza: Nature of The DiseaseDocument8 pagesSwine Influenza: Nature of The Diseasejawairia_mmgNo ratings yet
- ViralDocument49 pagesViralأحمد خيريNo ratings yet
- PlagueDocument33 pagesPlaguesurajaarya11No ratings yet
- Herpesvirida E& Adenoviridae: By: MJ Briones Bsn-IiDocument93 pagesHerpesvirida E& Adenoviridae: By: MJ Briones Bsn-IiMj BrionesNo ratings yet
- Chikungunya FeverDocument16 pagesChikungunya Feversiwap34656No ratings yet
- Bovine Viral Diseases: 1: Foot and Mouth Disease (FMD)Document17 pagesBovine Viral Diseases: 1: Foot and Mouth Disease (FMD)chachaNo ratings yet
- Communicable DiseaseDocument32 pagesCommunicable DiseaseRaquel M. MendozaNo ratings yet
- 0 - 1 April Journal ChikungunyaDocument7 pages0 - 1 April Journal ChikungunyaMayuri SonawaneNo ratings yet
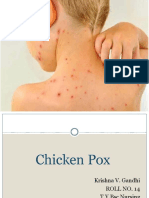
- Chicken PoxDocument26 pagesChicken PoxKrishna GandhiNo ratings yet
- FB4 - 11 - NishanKharel - Dengue and MalariaDocument18 pagesFB4 - 11 - NishanKharel - Dengue and Malariavaskar_karkiNo ratings yet
- Chickenpox and SmallpoxDocument28 pagesChickenpox and SmallpoxFourth YearNo ratings yet
- Dr.S.M. Joshi Medical Officer Faculty Member H.F.W.T.C.ThaneDocument9 pagesDr.S.M. Joshi Medical Officer Faculty Member H.F.W.T.C.ThaneEzekiel ArtetaNo ratings yet
- Diseases PIDSRDocument25 pagesDiseases PIDSRaringkinking100% (1)
- Penyebab Virus - Flaviridae (Dengue)Document32 pagesPenyebab Virus - Flaviridae (Dengue)Bendy Dwi IrawanNo ratings yet
- CHN - Communicable DiseaseDocument117 pagesCHN - Communicable DiseaseGetom NgukirNo ratings yet
- Chickenpo X: Presented By:-Priya Yadav Roll No 02 2 Yeat BSC Nursing (H) College of Nursing Dr. RML HospitalDocument41 pagesChickenpo X: Presented By:-Priya Yadav Roll No 02 2 Yeat BSC Nursing (H) College of Nursing Dr. RML HospitalNikita JangraNo ratings yet
- Community Notes by DR - Khan Final-1Document44 pagesCommunity Notes by DR - Khan Final-1Aqib IshaqNo ratings yet
- Viral Exanthema: Dharmendra MandalDocument57 pagesViral Exanthema: Dharmendra MandalMaunank TandelNo ratings yet
- Zoonotic VirusesDocument12 pagesZoonotic VirusesSamuel Ojonugwa AuduNo ratings yet
- TyphoidDocument67 pagesTyphoidArnel L. SanicoNo ratings yet
- Dengue: Epidemiological FactorsDocument11 pagesDengue: Epidemiological FactorsGetom NgukirNo ratings yet
- By-Dr. Samarjeet Kaur JR-II BRD Med. College GKPDocument17 pagesBy-Dr. Samarjeet Kaur JR-II BRD Med. College GKPSamarjeet Kaur100% (1)
- Dengue AwarenessDocument4 pagesDengue AwarenesssatpalNo ratings yet
- RabiesDocument28 pagesRabiesrouhanbinrashidNo ratings yet
- Viral Diseases - 06Document51 pagesViral Diseases - 06HIMANSHU SINGHNo ratings yet
- Zoonotic DiseaseDocument34 pagesZoonotic Diseasebajarangi_chaudhary100% (2)
- Dengue Malaria Group2Document100 pagesDengue Malaria Group2Arvinth Guna SegaranNo ratings yet
- Microbialdiseases 160303140348Document42 pagesMicrobialdiseases 160303140348proud.student2023No ratings yet
- Communicable DiseasesDocument43 pagesCommunicable Diseasesipshitadas.21No ratings yet
- Typhus Fever SetDocument3 pagesTyphus Fever SetIra TadikaNo ratings yet
- Mumps, Measles, Rubella (MMR) 06-07Document31 pagesMumps, Measles, Rubella (MMR) 06-07api-3699361100% (3)
- Zoonoses and Arthropod-Borne Diseases - AyaDocument22 pagesZoonoses and Arthropod-Borne Diseases - Aya180045No ratings yet
- Dr. Rehab Aljerbi Assistant Lecturer-Department of Family and Community Medicine Tripoli UniversityDocument31 pagesDr. Rehab Aljerbi Assistant Lecturer-Department of Family and Community Medicine Tripoli UniversityHannan AliNo ratings yet
- Infection Case 45 - HIV & AIDSDocument2 pagesInfection Case 45 - HIV & AIDSkabal321No ratings yet
- Yellow Fever: DR .. Magdi El Baloola Ahmed Physcian & GastrohepatologistDocument24 pagesYellow Fever: DR .. Magdi El Baloola Ahmed Physcian & GastrohepatologistÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- Fiebre AmarillaDocument4 pagesFiebre Amarillafreddy choqueNo ratings yet
- Rift Valley FeverDocument9 pagesRift Valley Feverapi-390015550No ratings yet
- Monkey Pox FinalDocument35 pagesMonkey Pox FinalHiren patelNo ratings yet
- Yellow Fever Original.Document12 pagesYellow Fever Original.Akinsoun MotunrayoNo ratings yet
- Monkey PoxDocument29 pagesMonkey PoxMalavika A GNo ratings yet
- Measles: Rubeola or Morbilli Department of Infectious Disease Wang JingyanDocument16 pagesMeasles: Rubeola or Morbilli Department of Infectious Disease Wang JingyankatsukagemaruNo ratings yet
- Chloroquine Phosphate.: Artemisinin-Based Combination Therapies (Acts)Document3 pagesChloroquine Phosphate.: Artemisinin-Based Combination Therapies (Acts)Getom NgukirNo ratings yet
- Factors Modifying Action of DrugsDocument28 pagesFactors Modifying Action of DrugsGetom NgukirNo ratings yet
- 5 - Introduction To Communicable DiseaseDocument32 pages5 - Introduction To Communicable DiseaseGetom Ngukir100% (1)
- CHN - Communicable DiseaseDocument117 pagesCHN - Communicable DiseaseGetom NgukirNo ratings yet
- PneumoniaDocument3 pagesPneumoniaGetom NgukirNo ratings yet
- Small Pox (CHN)Document13 pagesSmall Pox (CHN)Getom NgukirNo ratings yet
- Pratiksha College of Nursing Nursing Care Plan Format SUB: Nursing FoundationDocument4 pagesPratiksha College of Nursing Nursing Care Plan Format SUB: Nursing FoundationGetom NgukirNo ratings yet
- Classification SL - No Disease Rickettsial Agent Insect Vector Mammalian ReservoirsDocument4 pagesClassification SL - No Disease Rickettsial Agent Insect Vector Mammalian ReservoirsGetom NgukirNo ratings yet
- Dengue: Epidemiological FactorsDocument11 pagesDengue: Epidemiological FactorsGetom NgukirNo ratings yet
- Vomiting: Follows Nausea Comprises Labored Spasmodic Respiratory MovementsDocument5 pagesVomiting: Follows Nausea Comprises Labored Spasmodic Respiratory MovementsGetom NgukirNo ratings yet
- ZVD & LF (CHN)Document6 pagesZVD & LF (CHN)Getom NgukirNo ratings yet
- It Is A Zoonoses - A Group of Cestode Infections Which Are Important Zoonotic Diseases of ManDocument2 pagesIt Is A Zoonoses - A Group of Cestode Infections Which Are Important Zoonotic Diseases of ManGetom NgukirNo ratings yet
- Definition:: Pleural EffusionDocument4 pagesDefinition:: Pleural EffusionGetom NgukirNo ratings yet
- Respiratory Arrest and InsufficiencyDocument6 pagesRespiratory Arrest and InsufficiencyGetom Ngukir100% (1)
- Generics - The Swift Programming Language (Swift 5.7)Document28 pagesGenerics - The Swift Programming Language (Swift 5.7)jomi86No ratings yet
- TEST 3 (8 giỏi 1)Document4 pagesTEST 3 (8 giỏi 1)Alice WilliamsNo ratings yet
- UTS MODULE 1 (Done)Document11 pagesUTS MODULE 1 (Done)Alexis OngNo ratings yet
- CRPC Bail PresentationDocument8 pagesCRPC Bail PresentationDishant ThakkarNo ratings yet
- مذكرات كافر مغربي PDF - PDFDocument1 pageمذكرات كافر مغربي PDF - PDFYassin MejNo ratings yet
- Resonant Column TestDocument9 pagesResonant Column TestRana SenNo ratings yet
- Impression Management For LawyersDocument27 pagesImpression Management For Lawyersrulenso passmoreNo ratings yet
- QuestionnaireDocument4 pagesQuestionnaireSiva KumarNo ratings yet
- Transaction ManagerDocument62 pagesTransaction ManagerAnonymous 5cMeyYyxhNo ratings yet
- Cause and Effect Sutra English and ChineseDocument84 pagesCause and Effect Sutra English and ChineseVendyChenNo ratings yet
- Prediction of Return EductorDocument11 pagesPrediction of Return EductorToti TotiNo ratings yet
- The Miracle Morning - The Not-So-Obvious Secret Guaranteed To Transform Your Life Before 8amDocument1 pageThe Miracle Morning - The Not-So-Obvious Secret Guaranteed To Transform Your Life Before 8amPrashanth Bangalore100% (5)
- Havells - ProfessionalLuminaires Price ListDocument80 pagesHavells - ProfessionalLuminaires Price ListSuper UserNo ratings yet
- Big 1988Document145 pagesBig 1988Tony EmmerNo ratings yet
- Hostile Social ManipulationDocument303 pagesHostile Social ManipulationCV Jesus100% (1)
- Easystart, Marcel and The Mona Lisa AWDocument2 pagesEasystart, Marcel and The Mona Lisa AWVlad-NicolaeAchimNo ratings yet
- Silent MuslimDocument3 pagesSilent MuslimMohamed Dameer FahdNo ratings yet
- Bus Comm AssignDocument9 pagesBus Comm AssignKarenNo ratings yet
- Jordan ResumeDocument3 pagesJordan Resumeapi-462816920No ratings yet
- The Process of Empirical Research A Learning ExperienceDocument13 pagesThe Process of Empirical Research A Learning ExperienceSatyam MishraNo ratings yet
- Text TypesDocument6 pagesText TypesYifan ZhouNo ratings yet
- The Imamis Between Rationalism and TraditionalismDocument12 pagesThe Imamis Between Rationalism and Traditionalismmontazerm100% (1)
- Accountable Talk RubricDocument1 pageAccountable Talk RubricLauren K100% (1)
- Index Xenos Altansar CraftworldDocument14 pagesIndex Xenos Altansar CraftworldPaul Christian de Quant MinguetNo ratings yet
- Indefinite and Definite ArticlesDocument11 pagesIndefinite and Definite ArticlesRahela FoltNo ratings yet
- Factors Influencing Brand Loyalty For Samsung Mobile User in Nepal - With QuestionnaireDocument70 pagesFactors Influencing Brand Loyalty For Samsung Mobile User in Nepal - With QuestionnairevictorNo ratings yet
- Islcollective Worksheets Preintermediate A2 High School Reading Speaking Adjectives To Describe Personality and Characte 881191338542ea693560488 36713719Document2 pagesIslcollective Worksheets Preintermediate A2 High School Reading Speaking Adjectives To Describe Personality and Characte 881191338542ea693560488 36713719Citra Priski Abadi33% (9)
- Coolen ComplaintDocument4 pagesCoolen ComplaintKSTPTVNo ratings yet
- Fundamental of Software Engineering: Faculty of Technology Department of Computer Science Debre Tabor UniversityDocument17 pagesFundamental of Software Engineering: Faculty of Technology Department of Computer Science Debre Tabor UniversityBethelhem YetwaleNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (23)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- How to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingFrom EverandHow to ADHD: The Ultimate Guide and Strategies for Productivity and Well-BeingNo ratings yet
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Troubled: A Memoir of Foster Care, Family, and Social ClassFrom EverandTroubled: A Memoir of Foster Care, Family, and Social ClassRating: 4.5 out of 5 stars4.5/5 (26)