You might also like
- Modified Checklist For Autism in Toddlers Revised (MCHAT R/F) in An Urban Metropolitan Sample of Young Children in TurkeyDocument8 pagesModified Checklist For Autism in Toddlers Revised (MCHAT R/F) in An Urban Metropolitan Sample of Young Children in TurkeyProfe CatalinaNo ratings yet
- Nguyen 2019Document13 pagesNguyen 2019Jose Alonso Aguilar ValeraNo ratings yet
- 39-Article Text-77-1-10-202007Document7 pages39-Article Text-77-1-10-202007MageeNo ratings yet
- CitarDocument3 pagesCitarVictor NamurNo ratings yet
- Dental Caries Status in Autistic Children: A Meta Analysis: Yujian Zhang Ling Lin Jianbo Liu Ling Shi Jianping LuDocument9 pagesDental Caries Status in Autistic Children: A Meta Analysis: Yujian Zhang Ling Lin Jianbo Liu Ling Shi Jianping Luzsazsa nissaNo ratings yet
- Alshaban Et Al-2019-Journal of Child Psychology and PsychiatryDocument15 pagesAlshaban Et Al-2019-Journal of Child Psychology and PsychiatryZachNo ratings yet
- Validation of Indonesian M-CHAT for early autism detectionDocument7 pagesValidation of Indonesian M-CHAT for early autism detectionNurul MillatiNo ratings yet
- Priyanka K P Synopsis-1Document18 pagesPriyanka K P Synopsis-1RAJESHWARI PNo ratings yet
- M Chat Tamil 2020Document8 pagesM Chat Tamil 2020Profe CatalinaNo ratings yet
- JurnalDocument18 pagesJurnalEry ShaffaNo ratings yet
- Factors Associated With HIV Status Disclosure and Its Effect On Treatment Adherence and Quality of Life Among Children 6-17 YearDocument1 pageFactors Associated With HIV Status Disclosure and Its Effect On Treatment Adherence and Quality of Life Among Children 6-17 YearKarima Iffani UlifahNo ratings yet
- Evaluating Oral Health-Related Quality of Life Measure For Children and Preadolescents With Temporomandibular DisorderDocument12 pagesEvaluating Oral Health-Related Quality of Life Measure For Children and Preadolescents With Temporomandibular DisorderChika MarsenaNo ratings yet
- Indonesian Modified Checklist For Autism in ToddleDocument5 pagesIndonesian Modified Checklist For Autism in ToddleAfifah AtsmaraNo ratings yet
- Determinants of Stunting and Severe Stunting Among Under-Fives: Evidence From The 2011 Nepal Demographic and Health SurveyDocument15 pagesDeterminants of Stunting and Severe Stunting Among Under-Fives: Evidence From The 2011 Nepal Demographic and Health SurveyNIRMALANo ratings yet
- CHAPTER 02, Literature ReviewDocument27 pagesCHAPTER 02, Literature ReviewAyesha ArshedNo ratings yet
- Validation of The Modified Checklist For Autism in ToddlersDocument11 pagesValidation of The Modified Checklist For Autism in ToddlersFrancisca Aliaga ArellanoNo ratings yet
- Age of Diagnosis of Autism Spectrum Disorder in NepalDocument10 pagesAge of Diagnosis of Autism Spectrum Disorder in NepalKarel GuevaraNo ratings yet
- VR vs video distraction efficacy managing pain anxiety pediatric dental patientsDocument2 pagesVR vs video distraction efficacy managing pain anxiety pediatric dental patientsHashir SalamNo ratings yet
- Povećana Prevalencija AutizmaDocument4 pagesPovećana Prevalencija AutizmaJohn SmithNo ratings yet
- Validation of The Modified Checklist For Autism M CHAT RFDocument12 pagesValidation of The Modified Checklist For Autism M CHAT RFAmal AhamedNo ratings yet
- Article WMC004539Document13 pagesArticle WMC004539daniel_siitompulNo ratings yet
- Jenny Abanto, Georgios Tsakos, Saul Martins Paiva, Thiago S. Carvalho, Daniela P. Raggio and Marcelo BöneckerDocument10 pagesJenny Abanto, Georgios Tsakos, Saul Martins Paiva, Thiago S. Carvalho, Daniela P. Raggio and Marcelo BöneckerTasya AwaliyahNo ratings yet
- Chinese Dental Students' Knowledge and Attitudes Toward HIV/AIDSDocument7 pagesChinese Dental Students' Knowledge and Attitudes Toward HIV/AIDStamara tugasNo ratings yet
- A Critical Review of Autism Spectrum MeasuresDocument20 pagesA Critical Review of Autism Spectrum MeasuresJayne PenningtonNo ratings yet
- Csa ExaminationDocument21 pagesCsa ExaminationCorina IoanaNo ratings yet
- Magno 2018Document25 pagesMagno 2018baridinoNo ratings yet
- Archive of SIDDocument6 pagesArchive of SIDBeuty SavitriNo ratings yet
- Al Maqati2020Document6 pagesAl Maqati2020Paula FaberoNo ratings yet
- Effects of Risk Factors On Periodontal Disease Defined by Calibrated Community Periodontal Index and Loss of Attachment ScoresDocument23 pagesEffects of Risk Factors On Periodontal Disease Defined by Calibrated Community Periodontal Index and Loss of Attachment ScoresinkaNo ratings yet
- 10 1016@j Spen 2020 100831Document17 pages10 1016@j Spen 2020 100831tania luarteNo ratings yet
- Knowledge, Awareness and Perception On Contraception Among Women of Reproductive Age Attending Senawang Health ClinicDocument7 pagesKnowledge, Awareness and Perception On Contraception Among Women of Reproductive Age Attending Senawang Health Clinic2A - Nicole Marrie Honrado100% (1)
- Knowledge, Decision-Making and Acceptance of Human Papilloma Virus Vaccination Among Parents of Primary School Students in Kota Bharu, Kelantan, MalaysiaDocument6 pagesKnowledge, Decision-Making and Acceptance of Human Papilloma Virus Vaccination Among Parents of Primary School Students in Kota Bharu, Kelantan, MalaysiaMeidina DewatiNo ratings yet
- The Reported Edmonton Frail Scale-Thai Version DevDocument9 pagesThe Reported Edmonton Frail Scale-Thai Version DevIsmail ZeroualNo ratings yet
- Autism Research - 2021 - Tan - Prevalence and Age of Onset of Regression in Children With Autism Spectrum Disorder ADocument17 pagesAutism Research - 2021 - Tan - Prevalence and Age of Onset of Regression in Children With Autism Spectrum Disorder AAlhabbadNo ratings yet
- Hodge 2018Document7 pagesHodge 2018Ines Arias PazNo ratings yet
- Cognitive Behaviour Therapy For Anxious Paediatric Dental Patients: A Systematic ReviewDocument10 pagesCognitive Behaviour Therapy For Anxious Paediatric Dental Patients: A Systematic ReviewSung Soon ChangNo ratings yet
- Ages Questionary Development ScreeningDocument7 pagesAges Questionary Development ScreeningPamela Chuquicondor CuevaNo ratings yet
- AsdDocument7 pagesAsdElian Y. Sanchez-RiveraNo ratings yet
- Sociodemographic Barriers To Early Detection of Autism M CHAT RFDocument12 pagesSociodemographic Barriers To Early Detection of Autism M CHAT RFAmal AhamedNo ratings yet
- Stunting 2 PDFDocument7 pagesStunting 2 PDFPermata HatiNo ratings yet
- Clinician Perspectives On Telehealth Assessment of Autism Spectrum Disorder During The COVID-19 PandemicDocument16 pagesClinician Perspectives On Telehealth Assessment of Autism Spectrum Disorder During The COVID-19 PandemicrenatoNo ratings yet
- Parents' Emotions Toward Children's Dental TreatmentDocument5 pagesParents' Emotions Toward Children's Dental TreatmentpanduutamidrgNo ratings yet
- CDH 4550barasuol05Document5 pagesCDH 4550barasuol05Deepakrajkc DeepuNo ratings yet
- Assessment Tools 2Document43 pagesAssessment Tools 2Letícia Maraqui PrezziNo ratings yet
- Ijcpd 16 199Document6 pagesIjcpd 16 199Shahid ShaikhNo ratings yet
- Journal of Communication Disorders: Rachel Preston, Marie Halpin, Gemma Clarke, Sharon MillardDocument14 pagesJournal of Communication Disorders: Rachel Preston, Marie Halpin, Gemma Clarke, Sharon MillardNUR SYIFAA HAZWANI MOHAMAD SUHAIMINo ratings yet
- Awareness, Knowledge Level, and Misconceptions AboutDocument11 pagesAwareness, Knowledge Level, and Misconceptions AboutlhykaNo ratings yet
- China 2019 Guo Article ReliabilityAndValidityOfTheChina MCHAT RFDocument12 pagesChina 2019 Guo Article ReliabilityAndValidityOfTheChina MCHAT RFKarel GuevaraNo ratings yet
- Impact of Traumatic Dental Injuries and Malocclusions On Quality of Life of Preschool Children: A Population-Based StudyDocument11 pagesImpact of Traumatic Dental Injuries and Malocclusions On Quality of Life of Preschool Children: A Population-Based StudyfghdhmdkhNo ratings yet
- Dental Fear and Concomitant Factors in 3-6 Year-Old ChildrenDocument5 pagesDental Fear and Concomitant Factors in 3-6 Year-Old ChildrenDrSugandh MittalNo ratings yet
- Xu Tian Et Al, Meta AnalisisDocument10 pagesXu Tian Et Al, Meta Analisisnadya gratiaNo ratings yet
- Kelly 2019Document17 pagesKelly 2019Sergio A. Dávila SantanaNo ratings yet
- Adult PsychiatricDocument21 pagesAdult PsychiatricAndré SilvaNo ratings yet
- Dental Utilization and Expenditures by Children With AutismDocument5 pagesDental Utilization and Expenditures by Children With AutismPoli BMNo ratings yet
- Artigo 2011 Prevalencia Autismo de MercadanteDocument5 pagesArtigo 2011 Prevalencia Autismo de MercadanteDan Cardoso da SilvaNo ratings yet
- Artikel Jurnal Reading IKGMDocument10 pagesArtikel Jurnal Reading IKGMYuvitri AyuNo ratings yet
- ZimbabweDocument10 pagesZimbabweRosa ParksNo ratings yet
- Universal Newborn Hearing Screening 2001Document11 pagesUniversal Newborn Hearing Screening 2001Alexander AdrielNo ratings yet
- Rakotomanana Et Al-2017-Maternal & Child NutritionDocument10 pagesRakotomanana Et Al-2017-Maternal & Child Nutritionsunino ninoNo ratings yet
- Pregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsFrom EverandPregnancy Tests Explained (2Nd Edition): Current Trends of Antenatal TestsNo ratings yet
- Differences in The Intellectual Profile of Children With Intellectual vs. Learning DisabilityDocument7 pagesDifferences in The Intellectual Profile of Children With Intellectual vs. Learning DisabilityKarel GuevaraNo ratings yet
- Pathology of Neurodegenerative DiseasesDocument22 pagesPathology of Neurodegenerative DiseasesKarel GuevaraNo ratings yet
- 415 2017 Article 8641Document8 pages415 2017 Article 8641Karel GuevaraNo ratings yet
- Evidence and Perspectives of Cell Senescence in Neurodegenerative DiseasesDocument11 pagesEvidence and Perspectives of Cell Senescence in Neurodegenerative DiseasesKarel GuevaraNo ratings yet
- Neurodegenerative diseases may have genetic roots in autoinflammationDocument11 pagesNeurodegenerative diseases may have genetic roots in autoinflammationKarel GuevaraNo ratings yet
- Cognitive Clusters in SpecificDocument11 pagesCognitive Clusters in SpecificKarel GuevaraNo ratings yet
- Epigenetic Eti Old IDocument10 pagesEpigenetic Eti Old IStella IguiniNo ratings yet
- Zebrafish and Medaka - Important Animal Models For Human Neurodegenerative DiseasesDocument17 pagesZebrafish and Medaka - Important Animal Models For Human Neurodegenerative DiseasesKarel GuevaraNo ratings yet
- Manual Raven Escala ColoreadaDocument71 pagesManual Raven Escala ColoreadaKarel Guevara100% (7)
- Comparative Analysis of The WISC-IV in A Clinical Setting - ADHD vs. non-ADHDDocument7 pagesComparative Analysis of The WISC-IV in A Clinical Setting - ADHD vs. non-ADHDKarel GuevaraNo ratings yet
- 702 2020 Article 2145Document36 pages702 2020 Article 2145Karel GuevaraNo ratings yet
- American J of Med Genetics PT C - 2021 - Bulbena Cabr - Updates On The Psychological and Psychiatric Aspects of The EhlersDocument9 pagesAmerican J of Med Genetics PT C - 2021 - Bulbena Cabr - Updates On The Psychological and Psychiatric Aspects of The EhlersKarel GuevaraNo ratings yet
- Cognitive Correlates of Dyslexia, Dyscalculia and Comorbid Dyslexia - DyscalculiaDocument10 pagesCognitive Correlates of Dyslexia, Dyscalculia and Comorbid Dyslexia - DyscalculiaKarel GuevaraNo ratings yet
- WISC-IV and WISC-V Verbal Comprehension Index Scores in ASDDocument12 pagesWISC-IV and WISC-V Verbal Comprehension Index Scores in ASDKarel GuevaraNo ratings yet
- A Review of Executive Function Deficits in AutismDocument12 pagesA Review of Executive Function Deficits in AutismKarel GuevaraNo ratings yet
- WISC-IV Intellectual Profiles in Korean Children and AdolescentsDocument8 pagesWISC-IV Intellectual Profiles in Korean Children and AdolescentsKarel GuevaraNo ratings yet
- Pediatric Allied Healthcare Professionals'knowledge and Self-Efficacy Regarding ASDDocument13 pagesPediatric Allied Healthcare Professionals'knowledge and Self-Efficacy Regarding ASDKarel GuevaraNo ratings yet
- Autism Spectrum Disorder in Sub-Saharan AfricaDocument43 pagesAutism Spectrum Disorder in Sub-Saharan AfricaKarel GuevaraNo ratings yet
- Parent Perceptions About Communicating With Providers Regarding Early Autism ConcernsDocument11 pagesParent Perceptions About Communicating With Providers Regarding Early Autism ConcernsSdNNo ratings yet
- Screening for AutismDocument14 pagesScreening for AutismKarel GuevaraNo ratings yet
- Prevalence of ADHD and Autism Spectrum Disorder in Children With Hypermobility Spectrum Disorders or Hypermobile Ehlers-Danlos Syndrome - A Retrospective StudyDocument10 pagesPrevalence of ADHD and Autism Spectrum Disorder in Children With Hypermobility Spectrum Disorders or Hypermobile Ehlers-Danlos Syndrome - A Retrospective StudyKarel GuevaraNo ratings yet
- Estimating The Prevalence ofDocument8 pagesEstimating The Prevalence ofKarel GuevaraNo ratings yet
- Using The Modified ChecklistDocument8 pagesUsing The Modified ChecklistKarel GuevaraNo ratings yet
- Parents' Experiences of Screening, Diagnosis, and Intervention For Children With Autism Spectrum Disorder.Document15 pagesParents' Experiences of Screening, Diagnosis, and Intervention For Children With Autism Spectrum Disorder.Karel GuevaraNo ratings yet
- Prevalence and Socioeconomic Correlates of Autism Among Children AttendingDocument10 pagesPrevalence and Socioeconomic Correlates of Autism Among Children AttendingKarel GuevaraNo ratings yet
- Parental Care-Seeking Pathway and Challenges For Autistic SpectrumDocument8 pagesParental Care-Seeking Pathway and Challenges For Autistic SpectrumKarel GuevaraNo ratings yet
- The Diagnostic Odyssey of Autism Spectrum Disorder: ObjectivesDocument10 pagesThe Diagnostic Odyssey of Autism Spectrum Disorder: ObjectivesJose Alonso Aguilar ValeraNo ratings yet
- Practice Patterns and Potential Barriers To Early Diagnosis of AutismDocument9 pagesPractice Patterns and Potential Barriers To Early Diagnosis of AutismKarel GuevaraNo ratings yet
- Family Experiences With The Diagnosis of Autism Spectrum DisorderDocument11 pagesFamily Experiences With The Diagnosis of Autism Spectrum DisorderKarel GuevaraNo ratings yet
- Lesson 04 Nutrition Tools, Standards and Guidelines Nutrient RecommendationsDocument4 pagesLesson 04 Nutrition Tools, Standards and Guidelines Nutrient RecommendationsMickey MouseNo ratings yet
- WCPT Guideline For Physical Therapy Records Management: Record Keeping, Storage, Retrieval and DisposalDocument17 pagesWCPT Guideline For Physical Therapy Records Management: Record Keeping, Storage, Retrieval and DisposalJaspreet kaurNo ratings yet
- HIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFDocument14 pagesHIV and AIDS in Malawi Groups Most Affected by HIV in Malawi HIV Disproportionately Affects Women in Malawi PDFJames ChinamasaNo ratings yet
- ENDO Q&A Mosby PDFDocument7 pagesENDO Q&A Mosby PDFShikhaNo ratings yet
- IGC 2 - Element 7 - Chemical HazardsDocument67 pagesIGC 2 - Element 7 - Chemical HazardsHim SiwakotiNo ratings yet
- Medical Marijuana BrochureDocument2 pagesMedical Marijuana BrochureMPP100% (1)
- PostsDocument6 pagesPostsQusaiBadrNo ratings yet
- Types of shock surgery updatesDocument1 pageTypes of shock surgery updatesskNo ratings yet
- Pediatrics 8 1202Document5 pagesPediatrics 8 1202ahmed yahyaNo ratings yet
- SMEDA Private HospitalDocument23 pagesSMEDA Private Hospitalomerzafar100% (1)
- Resbakuna - Comirnaty PoU Deck For Site Training and Education-FINAL-013122Document53 pagesResbakuna - Comirnaty PoU Deck For Site Training and Education-FINAL-013122toledanagerald516No ratings yet
- Micro para OSCE For YL6 BacteriaDocument2 pagesMicro para OSCE For YL6 Bacteriagzldiwa100% (1)
- Clinical Guidelines in Primary Care 3rdDocument12 pagesClinical Guidelines in Primary Care 3rdmimi100% (1)
- Caries Risk AssessmentDocument33 pagesCaries Risk AssessmentSomya Jain100% (1)
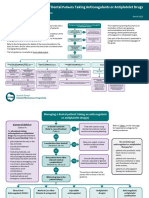
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocument5 pagesSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNo ratings yet
- Hydroxychloroquine Information Booklet 2022Document5 pagesHydroxychloroquine Information Booklet 2022Siddharth KorgaonkarNo ratings yet
- Of Office of The Secretary: Republic PhilippinesDocument112 pagesOf Office of The Secretary: Republic PhilippinesAlex SanchezNo ratings yet
- S4.M22.HO-Assessing Apical PulseDocument2 pagesS4.M22.HO-Assessing Apical PulseNugraNo ratings yet
- A Systematic Review: The Influence of Social Media On Depression, Anxiety and Psychological Distress in AdolescentsDocument6 pagesA Systematic Review: The Influence of Social Media On Depression, Anxiety and Psychological Distress in AdolescentsShivani NeroyNo ratings yet
- Sorbion SachetsDocument3 pagesSorbion SachetsReil_InsulaNo ratings yet
- Hospital Management System UML and Specification DocumentDocument16 pagesHospital Management System UML and Specification DocumentManish PareekNo ratings yet
- Q3 Health 8 Module 1 PDFDocument15 pagesQ3 Health 8 Module 1 PDFkateNo ratings yet
- Aisha Gillan ResumeDocument2 pagesAisha Gillan ResumeAisha GillanNo ratings yet
- Selective Grinding Goals and SequenceDocument22 pagesSelective Grinding Goals and Sequencepaulina yañezNo ratings yet
- Colostrum - How Does It Keep Health?Document9 pagesColostrum - How Does It Keep Health?JakirNo ratings yet
- WHO GHI Target Global Health ProblemsDocument17 pagesWHO GHI Target Global Health ProblemsKrisha Tañare-MalateNo ratings yet
- Urinary Catheter Core Care Plan September 2015 PDFDocument2 pagesUrinary Catheter Core Care Plan September 2015 PDFAsh Staley Delvin SparkNo ratings yet
- Mesothelioma TreatmentDocument3 pagesMesothelioma Treatmentsoupermen905No ratings yet
- Healing Healthcare Through PhilosophyDocument23 pagesHealing Healthcare Through PhilosophyZlom ProfNo ratings yet
- DPU AICET-2015 Information Brochure and Application FormDocument68 pagesDPU AICET-2015 Information Brochure and Application FormAvijat DashNo ratings yet