You might also like
- Dismissal Job AbandonmentDocument3 pagesDismissal Job AbandonmentMigz & Bet Catering & Paluto ServicesNo ratings yet
- Dismissal - Gross MisconductDocument2 pagesDismissal - Gross MisconductSamatar DaherNo ratings yet
- Human Resource Service Request SlipDocument1 pageHuman Resource Service Request SlipAvery Jan Magabanua SilosNo ratings yet
- Transfer Claim Form: 9th Floor Nirmal Building Nariman Point Mumbai 400 021Document2 pagesTransfer Claim Form: 9th Floor Nirmal Building Nariman Point Mumbai 400 021Karan RathoreNo ratings yet
- Time Keeping FormDocument13 pagesTime Keeping FormyamaNo ratings yet
- SMPL LTR DismissalDocument2 pagesSMPL LTR DismissalEdward AlmazanNo ratings yet
- Clearance Form: Lot 138 Panipuan, City of San Fernando, Pampanga 2000 Phone: +63 45 455 1939 Mobile: +63 9213276388Document3 pagesClearance Form: Lot 138 Panipuan, City of San Fernando, Pampanga 2000 Phone: +63 45 455 1939 Mobile: +63 9213276388Precious Mercado QuiambaoNo ratings yet
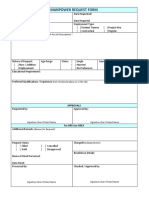
- Manpower Request Form: (Or Attach The Job Description)Document2 pagesManpower Request Form: (Or Attach The Job Description)pt koanbaNo ratings yet
- BNC employee leave guidelinesDocument2 pagesBNC employee leave guidelinessethu devadasNo ratings yet
- Salary Advance Request FormDocument1 pageSalary Advance Request FormTahir JahangirNo ratings yet
- Job Offer LetterDocument1 pageJob Offer LetterAmity TechnologiesNo ratings yet
- Leave Application Form: M/S.Ese Powercon PVT LTDDocument1 pageLeave Application Form: M/S.Ese Powercon PVT LTDuttam mishraNo ratings yet
- Extended Probationary StatusDocument1 pageExtended Probationary StatusAshna MeiNo ratings yet
- Mid-Year Manager EvaluationDocument3 pagesMid-Year Manager Evaluationprojectrik roomNo ratings yet
- Employee Information Form 01Document1 pageEmployee Information Form 01Dave Pagara0% (1)
- Admin PolicyDocument36 pagesAdmin PolicyMamun MozidNo ratings yet
- Completete SET OF HR FORMSDocument9 pagesCompletete SET OF HR FORMSALEXANDER DIMAFELIX JR.No ratings yet
- No Dues Checklist: AdministrationDocument2 pagesNo Dues Checklist: AdministrationpraneethNo ratings yet
- Termination, Regular EmployeeDocument2 pagesTermination, Regular EmployeeAzmyNo ratings yet
- Employee Movement Form.v01 - Recg - Mohamed Adam Izhar Bin Mohamed RidzwanDocument1 pageEmployee Movement Form.v01 - Recg - Mohamed Adam Izhar Bin Mohamed RidzwanXiao Minn NeohNo ratings yet
- College hospitality tourism waiver OJTDocument1 pageCollege hospitality tourism waiver OJTKenneth MarianoNo ratings yet
- Employee Information SheetDocument2 pagesEmployee Information SheetMeggy Okada Jung100% (2)
- Vacation, Sick and Bereavement LeaveDocument4 pagesVacation, Sick and Bereavement LeaveCherry AldayNo ratings yet
- Human Resources PresentationDocument8 pagesHuman Resources Presentationapi-299534152No ratings yet
- Form of AppealDocument1 pageForm of Appealadnan1888No ratings yet
- Revised Hours of Work Policy 071021Document19 pagesRevised Hours of Work Policy 071021Faridatul MelurNo ratings yet
- Sample Employee Absence FormDocument2 pagesSample Employee Absence FormTamara Glasgow-CoxNo ratings yet
- Sample COEDocument4 pagesSample COEMina MagallonesNo ratings yet
- HR Template - End of Contract NoticeDocument1 pageHR Template - End of Contract NoticeRobF100% (1)
- Personnel Movement FormDocument1 pagePersonnel Movement FormCathleya Marie CoNo ratings yet
- Promotion Letter TemplateDocument2 pagesPromotion Letter TemplateisabelaNo ratings yet
- Acts Against Attendance Policies: Notice To ExplainDocument2 pagesActs Against Attendance Policies: Notice To ExplainRecruitmentNo ratings yet
- Time Reporting Memo: Enforcement: The Department of Labor May Recover Back Wages Either Administratively orDocument3 pagesTime Reporting Memo: Enforcement: The Department of Labor May Recover Back Wages Either Administratively orsamNo ratings yet
- 70FB7C Sample Employee Reprimand Letter For TardinessDocument1 page70FB7C Sample Employee Reprimand Letter For TardinessJohn FaublNo ratings yet
- Administrative Hearing Memo for TherapistDocument1 pageAdministrative Hearing Memo for Therapistmigz_ortalizaNo ratings yet
- HMO Enrollment FormDocument1 pageHMO Enrollment FormJoshuaBatisla-onSorianoNo ratings yet
- Pangasinan Ville Homeowners' Association, Inc.: Incident ReportDocument2 pagesPangasinan Ville Homeowners' Association, Inc.: Incident ReportMark Anthony CarigNo ratings yet
- Promotion and Salary Increment Letter Format 2Document1 pagePromotion and Salary Increment Letter Format 2Vijay Sahu100% (1)
- Locker AgreementDocument1 pageLocker Agreementapi-355617045No ratings yet
- Clearance Form - Employee Turn-Over ChecklistDocument2 pagesClearance Form - Employee Turn-Over Checklistjurex salomonNo ratings yet
- Jeff Lavarez Final - Employment Contract 9622Document4 pagesJeff Lavarez Final - Employment Contract 9622jeff lavarezNo ratings yet
- Holiday Notice (Special Non Working Holiday) - 83rd Araw NG Dabaw March 16, 2020Document1 pageHoliday Notice (Special Non Working Holiday) - 83rd Araw NG Dabaw March 16, 2020allanNo ratings yet
- 14J Sample Letter of Final Written Warning Due To Poor PerformanceDocument1 page14J Sample Letter of Final Written Warning Due To Poor PerformanceTerry OrzalesNo ratings yet
- Clearance Form UpdatedDocument1 pageClearance Form UpdatedmarkanthonymailigNo ratings yet
- Termination Letter TemplateDocument1 pageTermination Letter TemplateKeshvan Sugumaran100% (1)
- C0009 Contractual Employment ContractDocument1 pageC0009 Contractual Employment ContractAndrea R. LageraNo ratings yet
- Employment Contract For Various SkillsDocument3 pagesEmployment Contract For Various SkillsanjbeybiNo ratings yet
- Termination of employment due to unexplained absenceDocument1 pageTermination of employment due to unexplained absenceAllenNo ratings yet
- Attendence PolicyDocument2 pagesAttendence PolicyCalvin PCrunk McCoyNo ratings yet
- Notice To Explain: Ms. JoanDocument1 pageNotice To Explain: Ms. JoanSanchez Roman VictorNo ratings yet
- Purpose:: SC Technologies Global Pvt. LTD 205, Korang Road, I-10/3 Industrial Area. Islamabad, PakistanDocument2 pagesPurpose:: SC Technologies Global Pvt. LTD 205, Korang Road, I-10/3 Industrial Area. Islamabad, PakistanFarhan MehdiNo ratings yet
- Clearance FormDocument2 pagesClearance FormselvamuthukumarNo ratings yet
- VL Form PDFDocument1 pageVL Form PDFMarichu BuenafeNo ratings yet
- Non-Disclosure & Non Compete Agreement: Page 1 of 3Document3 pagesNon-Disclosure & Non Compete Agreement: Page 1 of 3humanresources.qualimarkNo ratings yet
- Memo OverbreakDocument1 pageMemo OverbreakHR GCapitalNo ratings yet
- HR Department Memo on Posting SchedulesDocument1 pageHR Department Memo on Posting SchedulesMichael Rey Zabala BalongcasNo ratings yet
- ATD-Form For Final PayDocument1 pageATD-Form For Final PayEve Mon BustosNo ratings yet
- Leave PolicyDocument6 pagesLeave PolicyMohammed AnwarNo ratings yet
- Overtime Pay Policy in 40 CharactersTITLE OTP-40 ensures fair OT payDocument3 pagesOvertime Pay Policy in 40 CharactersTITLE OTP-40 ensures fair OT payRen SyNo ratings yet
- Unauthorized Leave WarningDocument3 pagesUnauthorized Leave Warningpriya chaudharyNo ratings yet
- Retail Customer Service TrainingDocument36 pagesRetail Customer Service TrainingVice Cosmetics CareersNo ratings yet
- Retail Staff TrainingDocument18 pagesRetail Staff TrainingVice Cosmetics CareersNo ratings yet
- Authorization Matrix Provides Spending LimitsDocument1 pageAuthorization Matrix Provides Spending LimitsVice Cosmetics CareersNo ratings yet
- One On One Meeting Agenda Peak Sales RecruitingDocument1 pageOne On One Meeting Agenda Peak Sales RecruitingVice Cosmetics CareersNo ratings yet
- 23 09 2019 Public Works General Office Clerk Posting Sept 23Document1 page23 09 2019 Public Works General Office Clerk Posting Sept 23Vice Cosmetics CareersNo ratings yet
- Paradise Screwed - More Selected ColumnsDocument424 pagesParadise Screwed - More Selected ColumnsJuanan Nuevo100% (1)
- Trinidad Gamboa-Roces vs. Judge Ranhel PerezDocument2 pagesTrinidad Gamboa-Roces vs. Judge Ranhel PerezDiane Dee YaneeNo ratings yet
- Rental AgreementDocument3 pagesRental AgreementUdaya Rekha100% (1)
- Employer-Employee Relationship CasesDocument190 pagesEmployer-Employee Relationship CasesEloisa Katrina MadambaNo ratings yet
- JoshuaDocument88 pagesJoshuaaghorbanzadeh67% (3)
- Deed of Donation of A Portion of LandDocument1 pageDeed of Donation of A Portion of LandMarj ApolinarNo ratings yet
- Women EmpowerDocument105 pagesWomen EmpowerAmita Ahirwar100% (1)
- Lost TIN ID affidavitDocument1 pageLost TIN ID affidavitmessageforjasonNo ratings yet
- Death Penalty Review of Related LiteratureDocument5 pagesDeath Penalty Review of Related Literatureea89aa3z100% (1)
- Largest English Daily in South India to Probe Indians Named in Pandora Papers LeakDocument8 pagesLargest English Daily in South India to Probe Indians Named in Pandora Papers LeakDeepthi ChendhuluruNo ratings yet
- Tax Invoice: Original For RecipientDocument3 pagesTax Invoice: Original For RecipientS V ENTERPRISESNo ratings yet
- Doe V TrumpDocument49 pagesDoe V TrumpAnonymous 2lblWUW6rSNo ratings yet
- 9 Wisner V First National Bank of GallitzinDocument2 pages9 Wisner V First National Bank of GallitzinrNo ratings yet
- Constitution Tci Sections 7 and 8Document2 pagesConstitution Tci Sections 7 and 8api-294571442No ratings yet
- Proforma InvoiceDocument1 pageProforma InvoiceNgân DươngNo ratings yet
- Thomas Bernhard - Ereignisse (Occurrences)Document34 pagesThomas Bernhard - Ereignisse (Occurrences)fxxfyNo ratings yet
- Fin MS2Document4 pagesFin MS2chinnnababuNo ratings yet
- Torts and Damages Review Course Syllabus - Atty. TumandaDocument10 pagesTorts and Damages Review Course Syllabus - Atty. TumandaPaulo VillarinNo ratings yet
- The Camera Fades in To A Ground Shot of 59 Station RoadDocument2 pagesThe Camera Fades in To A Ground Shot of 59 Station Roadapi-691465288No ratings yet
- Gunslinger Sheet v2Document3 pagesGunslinger Sheet v2Dmread99No ratings yet
- MAPEH 9 Physical Education Rules and SignalsDocument3 pagesMAPEH 9 Physical Education Rules and SignalsAguinaldo Maria BelenNo ratings yet
- SSC CGL 2019 All 18 Shifts Compilation by Shubham Jain RBE PDFDocument528 pagesSSC CGL 2019 All 18 Shifts Compilation by Shubham Jain RBE PDFMayank Jha100% (2)
- George Learns to Communicate with His New TalkerDocument22 pagesGeorge Learns to Communicate with His New Talker羅世芬No ratings yet
- MAHABHARATADocument33 pagesMAHABHARATACathleen Rose GadianeNo ratings yet
- An Influential Human-Rights Group Weighs The Legalization of Sex WorkDocument2 pagesAn Influential Human-Rights Group Weighs The Legalization of Sex WorkKAMOGELONo ratings yet
- Avid Xelrod: Huntington Center 614.463.9441 41 South High Street 614.463.1108 Fax Suite 2400 Columbus, Ohio 43215Document3 pagesAvid Xelrod: Huntington Center 614.463.9441 41 South High Street 614.463.1108 Fax Suite 2400 Columbus, Ohio 43215David AxelrodNo ratings yet
- Community Policing Partnerships For Problem Solving 7th Edition Miller Solutions ManualDocument5 pagesCommunity Policing Partnerships For Problem Solving 7th Edition Miller Solutions ManualCassandraGilbertodjrg100% (20)
- Application For Lien Sale Authorization and Lienholder'S CertificationDocument2 pagesApplication For Lien Sale Authorization and Lienholder'S CertificationBob WiserNo ratings yet
- Rights and PrivilegesDocument2 pagesRights and PrivilegesKeerthi Shetty100% (1)
- The Indian Express (12 November 2022Document20 pagesThe Indian Express (12 November 2022Pragya GoyalNo ratings yet