You might also like
- How To Know If You Need A Rest Day - Based On The Teachings Of Dr. Andrew Huberman: Unlocking Your Body's Secret Signals For The Perfect Rest DayFrom EverandHow To Know If You Need A Rest Day - Based On The Teachings Of Dr. Andrew Huberman: Unlocking Your Body's Secret Signals For The Perfect Rest DayNo ratings yet
- 0 Absent 1 Altered 2 Normal NT Not TestableDocument2 pages0 Absent 1 Altered 2 Normal NT Not Testablepablo lópezNo ratings yet
- Thang điểm ASIADocument2 pagesThang điểm ASIADiệu My VươngNo ratings yet
- ASIADocument2 pagesASIALuis Galván BastidasNo ratings yet
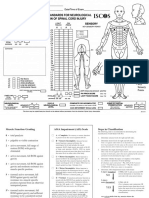
- Spinal Cord Injury Assessment Chart (ASIA)Document2 pagesSpinal Cord Injury Assessment Chart (ASIA)cpradheep100% (5)
- Isncsci Exam Sheet r4Document2 pagesIsncsci Exam Sheet r4akhmadukiNo ratings yet
- Asia Score For Vertebra InjuryDocument2 pagesAsia Score For Vertebra InjuryAzwin Kamar100% (1)
- Muscle Function and ASIA Impairment Scale DefinitionsDocument2 pagesMuscle Function and ASIA Impairment Scale DefinitionsIqbal BaryarNo ratings yet
- Asia Chart IscosDocument2 pagesAsia Chart IscosJeremiah HiiNo ratings yet
- ASIA Impairment ScaleDocument10 pagesASIA Impairment Scaleazimahzainal211No ratings yet
- ASIA Scoring CardDocument2 pagesASIA Scoring CardSomu VictorNo ratings yet
- Isncsci Asia Iscos LowDocument2 pagesIsncsci Asia Iscos LowmanuelmayoralNo ratings yet
- AIS 2011 ResumeDocument7 pagesAIS 2011 Resumesani widya firnandaNo ratings yet
- SEnSORY MOTOR TESTDocument4 pagesSEnSORY MOTOR TESTSergio Navarrete VidalNo ratings yet
- Spine ScoreDocument3 pagesSpine ScoreSteven TandeanNo ratings yet
- ASIA WorksheetDocument2 pagesASIA Worksheetmayones80No ratings yet
- ASIA WorksheetDocument2 pagesASIA WorksheetDinar Yudistira FirdausNo ratings yet
- evaluation of SCI -ASIADocument12 pagesevaluation of SCI -ASIAwr48f26rjmNo ratings yet
- Klasifikasi Dan Pengukuran ASIADocument8 pagesKlasifikasi Dan Pengukuran ASIAannisayaNo ratings yet
- American Spinal Cord Injury Association (ASIA) Impairment Scale - PhysiopediaDocument1 pageAmerican Spinal Cord Injury Association (ASIA) Impairment Scale - PhysiopediaMary OvbieboNo ratings yet
- Asia ScaleDocument30 pagesAsia ScaleKavya MittalNo ratings yet
- Spine Trauma - Dr. Didik Librianto, SpOT (K)Document65 pagesSpine Trauma - Dr. Didik Librianto, SpOT (K)Verty SalleNo ratings yet
- Assessment: The Neurologic Exam: InterviewDocument10 pagesAssessment: The Neurologic Exam: InterviewJun ManNo ratings yet
- SPINEDocument8 pagesSPINEadrian kristopher dela cruzNo ratings yet
- Output 14Document2 pagesOutput 14Ephraim BernaldezNo ratings yet
- NIH Stroke Scale for Diagnosing Stroke SubtypeDocument23 pagesNIH Stroke Scale for Diagnosing Stroke SubtypekNo ratings yet
- Isncsci / Asia Examination & Cases: ObjectivesDocument27 pagesIsncsci / Asia Examination & Cases: Objectivesrj salvosaNo ratings yet
- Physiology Lab 2 - Motor ExaminationsDocument6 pagesPhysiology Lab 2 - Motor Examinationsk tawNo ratings yet
- NIH Stroke Scale BookletDocument11 pagesNIH Stroke Scale Bookletcleber333100% (2)
- NCP Hip FractureDocument5 pagesNCP Hip FractureCherry Ann BalagotNo ratings yet
- 116A PrelimsDocument6 pages116A PrelimsKimjin MallareNo ratings yet
- 9.1. Pract. Erb Palsy WorksheetDocument6 pages9.1. Pract. Erb Palsy WorksheetNoof AlmarriNo ratings yet
- F0826 International Standards For Neurological Classification of SCI Worksheet HGHDGDocument25 pagesF0826 International Standards For Neurological Classification of SCI Worksheet HGHDGreeves_cool100% (1)
- 整理Document5 pages整理SilvieNo ratings yet
- Peripheral Neuropathies (Trans)Document3 pagesPeripheral Neuropathies (Trans)Preeti Joan BuxaniNo ratings yet
- SPINEDocument8 pagesSPINEadrian kristopher dela cruzNo ratings yet
- Mất vững CSTLDocument36 pagesMất vững CSTL46 Lê Văn BìnhNo ratings yet
- NIHSSDocument1 pageNIHSSBobet Reña100% (1)
- chapter-167Document14 pageschapter-167Cluster 1 2023No ratings yet
- Manual Muscle TestingDocument38 pagesManual Muscle TestingNada RonaldNo ratings yet
- Autonomic Nervous SystemDocument12 pagesAutonomic Nervous SystemKaye NeeNo ratings yet
- SCI EvaluationDocument11 pagesSCI EvaluationNereen EssamNo ratings yet
- Rehabilitation Methods for Hemianopic DyslexiaDocument29 pagesRehabilitation Methods for Hemianopic DyslexiaGenoveva IoanaNo ratings yet
- Clinical Examination of The Patient With Brachial Plexus PalsyDocument12 pagesClinical Examination of The Patient With Brachial Plexus PalsyAndre SugiyonoNo ratings yet
- Assessing ReflexesDocument9 pagesAssessing ReflexesRoger ViloNo ratings yet
- Introduction To SpineDocument29 pagesIntroduction To Spinebmahmood1No ratings yet
- NEURO-CONCEPT-NOTESDocument35 pagesNEURO-CONCEPT-NOTEShoney requermeNo ratings yet
- 1 Degrees of Freedom: Rigid Body FixityDocument2 pages1 Degrees of Freedom: Rigid Body FixityCarl SorensenNo ratings yet
- Lab Act 1 - Motor AssessmentDocument6 pagesLab Act 1 - Motor AssessmentZgama AbdulrahmanNo ratings yet
- !exercise Prescription Guidelines - Feb 2020 - FINALDocument2 pages!exercise Prescription Guidelines - Feb 2020 - FINALJordnNo ratings yet
- B. INGGRIS Kls XIDocument5 pagesB. INGGRIS Kls XIwindiNo ratings yet
- Protocolo Stars CrashDocument24 pagesProtocolo Stars CrashteranrobleswaltergabrielNo ratings yet
- Hubungan Antara Intensitas Aktivitas Fisik Dengan Konstipasi Pada Wanita MenopauseDocument11 pagesHubungan Antara Intensitas Aktivitas Fisik Dengan Konstipasi Pada Wanita MenopauseMulti Sari DewiNo ratings yet
- Project Proposal MathDocument5 pagesProject Proposal MathLorenz Philip AriasNo ratings yet
- Roughan and Flecknell, 2006Document16 pagesRoughan and Flecknell, 2006Paul FlecknellNo ratings yet
- Natural History of Disease FINALDocument13 pagesNatural History of Disease FINALnadia nisarNo ratings yet
- Iso 45001Document4 pagesIso 45001Muhammad Danial KhanNo ratings yet
- MSDS NutristarDocument12 pagesMSDS NutristarThảo ThuNo ratings yet
- The Relaxation and Stress Reduction Workbook For Teens CBT SkillsDocument186 pagesThe Relaxation and Stress Reduction Workbook For Teens CBT Skillsfirankisan1313No ratings yet
- Stool AnalysisDocument39 pagesStool AnalysisKhmissiBénnadjiNo ratings yet
- Breastfeeding and Tongue-TieDocument2 pagesBreastfeeding and Tongue-TieClara CarneiroNo ratings yet
- Urinary & Excretory System RegentsDocument3 pagesUrinary & Excretory System Regentsabisantiago6131No ratings yet
- Chemistry Project FileDocument11 pagesChemistry Project FileYash ManralNo ratings yet
- Sbar Communication Model: Situation, Background, Assessment, and RecommendationDocument27 pagesSbar Communication Model: Situation, Background, Assessment, and RecommendationRaquel MonsalveNo ratings yet
- Makalah Singkat FarmasiDocument6 pagesMakalah Singkat FarmasiArul DarmansyahNo ratings yet
- Types of StressDocument2 pagesTypes of StressLuz Marina Mejía MorenoNo ratings yet
- TM 5. Struktur ICD 10Document14 pagesTM 5. Struktur ICD 10HardLine GAMINGNo ratings yet
- Villi and AbsorptionDocument24 pagesVilli and AbsorptionAghaanaa JaiganeshNo ratings yet
- GANGRENEDocument37 pagesGANGRENERick Ghosh (Shreyam)No ratings yet
- Well Behaved WomenDocument141 pagesWell Behaved WomenBrad GlasmanNo ratings yet
- 20-21 WCSD Reopening Plan FinalDocument36 pages20-21 WCSD Reopening Plan FinalWETMNo ratings yet
- Instructions For Use: Stainless Steel Mix TanksDocument16 pagesInstructions For Use: Stainless Steel Mix TanksHendra WiratamaNo ratings yet
- Quarter 4 Assessment Test 4 Mapeh 7: Guipos National High School Poblacion, Guipos Zamboanga Del SurDocument2 pagesQuarter 4 Assessment Test 4 Mapeh 7: Guipos National High School Poblacion, Guipos Zamboanga Del SurCristia Marie Combalicer ColastreNo ratings yet
- Septum Uterino Transverso Por HisterosDocument14 pagesSeptum Uterino Transverso Por HisterosmilifeerNo ratings yet
- Writing Workshop Problem-Solution Essay 2022-2Document3 pagesWriting Workshop Problem-Solution Essay 2022-2Mari joseNo ratings yet
- Hazard Identification and Risk Assessment TemplateDocument3 pagesHazard Identification and Risk Assessment TemplateSejal SatputeNo ratings yet
- Shvatanje Rata - PrilogDocument37 pagesShvatanje Rata - PrilogNikola StarčevićNo ratings yet
- Camp Inspection ChecklistDocument5 pagesCamp Inspection Checklistsubhanmusadiq63% (8)
- Compassion Fatigue Are You at RiskDocument1 pageCompassion Fatigue Are You at RisknitistudyaccNo ratings yet
- Listening Skills for Loving Yourself and OthersDocument75 pagesListening Skills for Loving Yourself and Othersfati_cenNo ratings yet