You might also like
- Stability and Uniformity of Extemporaneous Preparations of Voriconazole in Two Liquid Suspension Vehicles at Two Storage TemperaturesDocument7 pagesStability and Uniformity of Extemporaneous Preparations of Voriconazole in Two Liquid Suspension Vehicles at Two Storage TemperaturesLUIS MIGUEL CASTILLA MORANNo ratings yet
- NMRDocument135 pagesNMRKhan Sameer100% (1)
- Using Remifentanil in Mechanically VentilatedDocument5 pagesUsing Remifentanil in Mechanically VentilatedChurrunchaNo ratings yet
- Intravenous Infusion of Lidocaine Reduces PropofolDocument6 pagesIntravenous Infusion of Lidocaine Reduces PropofolAnonymous lSWQIQNo ratings yet
- Proceeding of The LAVC Latin American Veterinary Conference Apr. 22-25, 2014 - Lima, PeruDocument3 pagesProceeding of The LAVC Latin American Veterinary Conference Apr. 22-25, 2014 - Lima, PeruLove GeckoNo ratings yet
- Clinical Assessment of Repeated Propofol-Associated Anesthesia in CatsDocument7 pagesClinical Assessment of Repeated Propofol-Associated Anesthesia in CatsSatria Adi MarhendraNo ratings yet
- Pi Is 0007091217382302Document5 pagesPi Is 0007091217382302agnes hutabaratNo ratings yet
- Drug-Induced Sleep Endoscopy in Adults With Sleep-Disordered Breathing: Technique and The VOTE Classification SystemDocument8 pagesDrug-Induced Sleep Endoscopy in Adults With Sleep-Disordered Breathing: Technique and The VOTE Classification SystemSheila Rahmi Ismi FaizahNo ratings yet
- Comparison of Propofol CRI and Isoflurane Speke Gazelle 2017Document11 pagesComparison of Propofol CRI and Isoflurane Speke Gazelle 2017Tareas GalileoNo ratings yet
- Layryngeal Mask Airway Placement: A Comparison Between Propofol and Thiopentone Sodium in The Day Case SurgeryDocument5 pagesLayryngeal Mask Airway Placement: A Comparison Between Propofol and Thiopentone Sodium in The Day Case SurgeryAzzam Saqr100% (1)
- Propofol: Present by The StudentDocument7 pagesPropofol: Present by The StudentAli dhyaaNo ratings yet
- Southern African Journal of Anaesthesia and AnalgesiaDocument6 pagesSouthern African Journal of Anaesthesia and AnalgesiaAF KoasNo ratings yet
- Use of A Combination of Propofol and Fentanyl, Alfentanil, or Sufentanil For Total Intravenous Anesthesia in CatsDocument6 pagesUse of A Combination of Propofol and Fentanyl, Alfentanil, or Sufentanil For Total Intravenous Anesthesia in CatsRajesh KumarNo ratings yet
- 2021 VCNA Lizard Sedation AnesthesiaDocument23 pages2021 VCNA Lizard Sedation AnesthesiaFiorella YavarNo ratings yet
- Safety of Propofol When Used For Rapid Sequence Intubation in Septic Patients: A Multicenter Cohort StudyDocument7 pagesSafety of Propofol When Used For Rapid Sequence Intubation in Septic Patients: A Multicenter Cohort StudyPaloma LizardiNo ratings yet
- Journal English AsliDocument19 pagesJournal English AslidenokkosasiNo ratings yet
- Melo Toxicity and Penetration Retina 2010Document7 pagesMelo Toxicity and Penetration Retina 2010Igor VainerNo ratings yet
- Nebulised Furosemide in The PaDocument8 pagesNebulised Furosemide in The PaManisha UppalNo ratings yet
- Comparissons NeuroanesthesiaDocument8 pagesComparissons Neuroanesthesialina yohanesNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleRajesh KumarNo ratings yet
- Propofol AnesthesiaDocument3 pagesPropofol AnesthesiaJulio Cesar Marin ConchaNo ratings yet
- Paper Anestesicos MedvetDocument6 pagesPaper Anestesicos Medvetmelimeli106No ratings yet
- Articulo SaidDocument11 pagesArticulo SaidAna Karen Rodriguez AldamaNo ratings yet
- UEG Journal - 2018 - Nishizawa - Propofol For Gastrointestinal EndosDocument5 pagesUEG Journal - 2018 - Nishizawa - Propofol For Gastrointestinal Endosmax medinaNo ratings yet
- Comparison of Drooeridol&,metoclopramideDocument4 pagesComparison of Drooeridol&,metoclopramidemanishmandal1976No ratings yet
- JurnalDocument9 pagesJurnalYanuar Ahsan OfficialNo ratings yet
- Novel Therapy For Hearing Loss: Delivery of Insulin-Like Growth Factor 1 To The Cochlea Using Gelatin HydrogelDocument6 pagesNovel Therapy For Hearing Loss: Delivery of Insulin-Like Growth Factor 1 To The Cochlea Using Gelatin HydrogelHinami TenukiNo ratings yet
- A Randomized Controlled Trial To Determine The.26Document6 pagesA Randomized Controlled Trial To Determine The.26blok etikakedokteranNo ratings yet
- Anesthesia and Procedural MonitoringDocument5 pagesAnesthesia and Procedural MonitoringVanesa Michelle Estrella ObregonNo ratings yet
- Case Study PropofolDocument7 pagesCase Study PropofolaliasLiew100% (1)
- Técnicas de Anestesia Regional Retrobulbar Versus Peribulbar Con Bupivacaína en PerrosDocument10 pagesTécnicas de Anestesia Regional Retrobulbar Versus Peribulbar Con Bupivacaína en PerrosCarolina Duque RodriguezNo ratings yet
- NVBNDocument7 pagesNVBNAnonymous 5K38SwLNo ratings yet
- Lidocaine and Bupivacaine As Part of Multimodal Pain Management in A C57BL/6J Laparotomy Mouse ModelDocument17 pagesLidocaine and Bupivacaine As Part of Multimodal Pain Management in A C57BL/6J Laparotomy Mouse ModelJaka HerbiyantoNo ratings yet
- Downloaded File-195Document6 pagesDownloaded File-195Abdul RachmanNo ratings yet
- Neuroscience Letters: Laura Monni, Filippo Ghezzi, Silvia Corsini, Andrea NistriDocument6 pagesNeuroscience Letters: Laura Monni, Filippo Ghezzi, Silvia Corsini, Andrea NistriardhiNo ratings yet
- Shoemaker Et Al 2020 Disparity in The Effect of Morphine On Eupnea and Gasping in Anesthetized Spontaneously BreathingDocument15 pagesShoemaker Et Al 2020 Disparity in The Effect of Morphine On Eupnea and Gasping in Anesthetized Spontaneously Breathingoliwia.be92No ratings yet
- Response and Physiologic Outcomes After Butorphanol, Midazolam, and Medetomidine Immobilization and Reversal in Captive Reindeer (Rangifer Tarandus)Document6 pagesResponse and Physiologic Outcomes After Butorphanol, Midazolam, and Medetomidine Immobilization and Reversal in Captive Reindeer (Rangifer Tarandus)Javiera Meza LunaNo ratings yet
- Journal Homepage: - : IntroductionDocument9 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Low-Dose HaloperidolDocument6 pagesLow-Dose Haloperidolapi-741687858No ratings yet
- Brief/Technical Note Pulmonary Toxicity of Polysorbate-80-Coated Inhalable Nanoparticles in Vitro and in Vivo EvaluationDocument6 pagesBrief/Technical Note Pulmonary Toxicity of Polysorbate-80-Coated Inhalable Nanoparticles in Vitro and in Vivo Evaluationrey_hadesNo ratings yet
- Literature Survey On The Dependence of Demography On Depth of AnaesthesiaDocument7 pagesLiterature Survey On The Dependence of Demography On Depth of AnaesthesiaLoktongbam Disney MeiteiNo ratings yet
- Assessment of The Cough Reflex After Propofol Anaesthesia For ColonosDocument4 pagesAssessment of The Cough Reflex After Propofol Anaesthesia For ColonosIta RositaNo ratings yet
- Metabolic Precursors of SurfactantDocument8 pagesMetabolic Precursors of Surfactantatika sgrtNo ratings yet
- Deep Sedation During Gastrointestinal Endoscopy: Propofol-Fentanyl and Midazolam-Fentanyl RegimensDocument8 pagesDeep Sedation During Gastrointestinal Endoscopy: Propofol-Fentanyl and Midazolam-Fentanyl RegimensiweNo ratings yet
- Transition To Propofol After Sevoflurane Anesthesia To Prevent Emergence Agitation: A Randomized Controlled TrialDocument7 pagesTransition To Propofol After Sevoflurane Anesthesia To Prevent Emergence Agitation: A Randomized Controlled TrialAndhi Riawan Eko WiikramatunggadewaNo ratings yet
- International Journal of Antimicrobial AgentsDocument8 pagesInternational Journal of Antimicrobial AgentsSarah AlmiraNo ratings yet
- Artikel 6Document11 pagesArtikel 6Iin Novita SariNo ratings yet
- Atropin Organophosphorus 2Document9 pagesAtropin Organophosphorus 2Elizabeth Toapanta VrnNo ratings yet
- En V62n6a03Document8 pagesEn V62n6a03dian primaNo ratings yet
- Ausculta Cervical y PulmonarDocument9 pagesAusculta Cervical y PulmonarDaniela VRNo ratings yet
- Drug-Induced Sleep Endoscopy (DISE)Document4 pagesDrug-Induced Sleep Endoscopy (DISE)Luis De jesus SolanoNo ratings yet
- Profopol Vs KTMDocument7 pagesProfopol Vs KTMAuliaRusdiAllmuttaqienNo ratings yet
- BjorlDocument6 pagesBjorlaaNo ratings yet
- Nss 10 271Document16 pagesNss 10 271杨钦杰No ratings yet
- Propofol: CH (CH) OH CH (CH)Document3 pagesPropofol: CH (CH) OH CH (CH)Arfadin YusufNo ratings yet
- Uso de Premedicacion Intubacion 2018 CartaDocument2 pagesUso de Premedicacion Intubacion 2018 CartaJorge CastroNo ratings yet
- Rationale For Naphazoline Effects In-Depth StudyDocument5 pagesRationale For Naphazoline Effects In-Depth StudyJasmin AfifNo ratings yet
- Rocuronio Nao Influencia No PSIDocument7 pagesRocuronio Nao Influencia No PSIbrasilvilermandoNo ratings yet
- Dise 4Document5 pagesDise 4Prawira WijayaNo ratings yet
- Remifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized StudyDocument7 pagesRemifentanil Compared With Midazolam and Pethidine Sedation During Colonoscopy: A Prospective, Randomized Studyade_liaNo ratings yet
- Granulomatous Colitis in A Cat: Escherichia Coli-InducedDocument5 pagesGranulomatous Colitis in A Cat: Escherichia Coli-Inducedsigario hutamaNo ratings yet
- Urinalysis in Companion Animals: Part 2: Evaluation of Urine Chemistry & SedimentDocument6 pagesUrinalysis in Companion Animals: Part 2: Evaluation of Urine Chemistry & Sedimentsigario hutamaNo ratings yet
- A Case of Glomerulonephritis in A 4-Year-Old Kano Brown DoeDocument7 pagesA Case of Glomerulonephritis in A 4-Year-Old Kano Brown DoeDewa Aix61No ratings yet
- Skripsi Tanpa Bab Pembahasan PDFDocument71 pagesSkripsi Tanpa Bab Pembahasan PDFmilaNo ratings yet
- Buprenorphine Veterinary Medication Guide For Patient Animal PetDocument2 pagesBuprenorphine Veterinary Medication Guide For Patient Animal Petdoppler_No ratings yet
- Corticosteroids 2008Document34 pagesCorticosteroids 2008Satish PandavNo ratings yet
- Feline Inflammatory Bowel Disease: How I Treat Feline IBDDocument4 pagesFeline Inflammatory Bowel Disease: How I Treat Feline IBDsigario hutamaNo ratings yet
- Mainland Clouded Leopard Reference ListDocument4 pagesMainland Clouded Leopard Reference Listsigario hutamaNo ratings yet
- Meat and Poultry ProductsDocument9 pagesMeat and Poultry Productssigario hutamaNo ratings yet
- Husbandry Manual PDFDocument56 pagesHusbandry Manual PDFToha PutraNo ratings yet
- Ekspresi Gen Homosigot Resesif (C/C) Pada Performans Telur Pertama Itik MojosariDocument6 pagesEkspresi Gen Homosigot Resesif (C/C) Pada Performans Telur Pertama Itik Mojosarisigario hutamaNo ratings yet
- Mainland Clouded Leopard Reference ListDocument4 pagesMainland Clouded Leopard Reference Listsigario hutamaNo ratings yet
- SK Klasifikasi Tindakan Operatif THT KLDocument6 pagesSK Klasifikasi Tindakan Operatif THT KLsigario hutamaNo ratings yet
- Identifikasi Bakteri OK Penelitian PDFDocument90 pagesIdentifikasi Bakteri OK Penelitian PDFsittaNo ratings yet
- Case Report AbdomenDocument5 pagesCase Report Abdomensigario hutamaNo ratings yet
- Serum RBT Hal 1, 4Document10 pagesSerum RBT Hal 1, 4sigario hutamaNo ratings yet
- Case Report ThoraxDocument7 pagesCase Report Thoraxsigario hutamaNo ratings yet
- Media Hal 1, 2Document8 pagesMedia Hal 1, 2sigario hutamaNo ratings yet
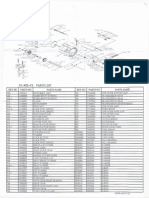
- Okuma CL302L Parts List & ManualDocument3 pagesOkuma CL302L Parts List & Manualcoolestkiwi100% (1)
- Huawei Sne Mobile Phone User Guide - (Emui9.0.1 - 01, En-Uk, Normal)Document68 pagesHuawei Sne Mobile Phone User Guide - (Emui9.0.1 - 01, En-Uk, Normal)FarzadNo ratings yet
- Theory of Multiple Intelligences and WhyDocument7 pagesTheory of Multiple Intelligences and WhyEveNo ratings yet
- Phy Interface Pci Express Sata Usb31 Architectures Ver43 PDFDocument99 pagesPhy Interface Pci Express Sata Usb31 Architectures Ver43 PDFRaj Shekhar ReddyNo ratings yet
- AWS Abbreviations Oxyfuel Cutting - OFC Oxyacetylene Cutting - OFC-A Oxyfuel Cutting - Process and Fuel GasesDocument8 pagesAWS Abbreviations Oxyfuel Cutting - OFC Oxyacetylene Cutting - OFC-A Oxyfuel Cutting - Process and Fuel GasesahmedNo ratings yet
- Motherboard Manual 6vem eDocument67 pagesMotherboard Manual 6vem eAri Ercilio Farias FereirraNo ratings yet
- CostcoDocument12 pagesCostcoThảo Nguyên PhạmNo ratings yet
- Most Popular Bootstrap Interview Questions and AnswersDocument6 pagesMost Popular Bootstrap Interview Questions and Answershassan TariqNo ratings yet
- PLC Anupam Samanta 2010JE0976Document64 pagesPLC Anupam Samanta 2010JE0976Anupam SamantaNo ratings yet
- Survey Questionnaire 3 - Student EngagementDocument2 pagesSurvey Questionnaire 3 - Student EngagementDAN MARK CAMINGAWANNo ratings yet
- CMNS Week 3.2 Memo AssignmentDocument2 pagesCMNS Week 3.2 Memo AssignmentPulkit KalhanNo ratings yet
- TT21 28112019BNN (E)Document40 pagesTT21 28112019BNN (E)Thanh Tâm TrầnNo ratings yet
- Ms. Louise Lim Mr. Ivan Cyrus DaldeDocument27 pagesMs. Louise Lim Mr. Ivan Cyrus DaldeJazlyn Andria JarafaNo ratings yet
- Jeff Nippard's Workout Routine & Diet (2022) - Jacked GorillaDocument11 pagesJeff Nippard's Workout Routine & Diet (2022) - Jacked Gorillaticoninx100% (1)
- Directorate of Pension, Provident Fund & Group Insurance: WWW - Wbepension.gov - inDocument37 pagesDirectorate of Pension, Provident Fund & Group Insurance: WWW - Wbepension.gov - inSandipan RoyNo ratings yet
- CRC Ace Far 1ST PBDocument9 pagesCRC Ace Far 1ST PBJohn Philip Castro100% (1)
- II If en April2015 EquitycompoundersDocument8 pagesII If en April2015 EquitycompoundersbgyggghjkkNo ratings yet
- The Blender InterfaceDocument22 pagesThe Blender InterfaceacocancerNo ratings yet
- 08 LCD Slide Handout 1Document5 pages08 LCD Slide Handout 1Jana Gabrielle Canonigo0% (1)
- The Impact On Digital Marketing During Pandemic Outbreak COVID-19 On Business DevelopmentDocument5 pagesThe Impact On Digital Marketing During Pandemic Outbreak COVID-19 On Business DevelopmentInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2006 Estes Model Rocketry CatalogDocument44 pages2006 Estes Model Rocketry CatalogMisesWasRightNo ratings yet
- A New Approach To Air Quality in Hospitals: Www.p3italy - ItDocument19 pagesA New Approach To Air Quality in Hospitals: Www.p3italy - ItMuneer Ahmed ShaikNo ratings yet
- Lesson 12 FastenersDocument9 pagesLesson 12 FastenersEmerson John RoseteNo ratings yet
- XDocument2 pagesXSophiaFrancescaEspinosaNo ratings yet
- "Assessing The Effect of Work Overload On Employees Job Satisfaction" Case of Commercial Bank of Ethiopia Nekemte Town BranchesDocument1 page"Assessing The Effect of Work Overload On Employees Job Satisfaction" Case of Commercial Bank of Ethiopia Nekemte Town Branchesmikiyas zerihunNo ratings yet
- 4 Komponen SDSSDocument9 pages4 Komponen SDSSRebecha Parsellya100% (1)
- Executive MBA Project - Self Help Allowance - FinalDocument55 pagesExecutive MBA Project - Self Help Allowance - FinalKumar SourabhNo ratings yet
- FSED 1F Application Form FSEC For Building Permit Rev02Document2 pagesFSED 1F Application Form FSEC For Building Permit Rev02Angelito RegulacionNo ratings yet
- Gibbs VerBeek CorrespondenceDocument3 pagesGibbs VerBeek CorrespondenceWXMINo ratings yet