You might also like
- Pharmacology MidtermDocument27 pagesPharmacology Midtermnaomie manaliliNo ratings yet
- Cardio Q&aDocument147 pagesCardio Q&aHoney Lyn AlebioNo ratings yet
- Nursing Care of Clients With Upper Airway or Respiratory DisordersDocument6 pagesNursing Care of Clients With Upper Airway or Respiratory DisordersLuna MarieNo ratings yet
- Lecture Notes on Fluids and Electrolytes by Mark Fredderick R AbejoDocument18 pagesLecture Notes on Fluids and Electrolytes by Mark Fredderick R Abejogreen_archerNo ratings yet
- DAILY ICU ROUNDSDocument59 pagesDAILY ICU ROUNDStuulipNo ratings yet
- Nursing Flash CardsDocument5 pagesNursing Flash CardsJan Clarisse RamosNo ratings yet
- Catheterization: A Guide to Proper TechniqueDocument33 pagesCatheterization: A Guide to Proper TechniqueJoseph DusichNo ratings yet
- NRS 2109 Revised Pharma Syllabus AY 2020 2021Document48 pagesNRS 2109 Revised Pharma Syllabus AY 2020 2021Julianne Kyla MercadoNo ratings yet
- MI MEDIC CARDS - Reference MaterialDocument26 pagesMI MEDIC CARDS - Reference MaterialAylinNo ratings yet
- Cardiotrophin 1Document2 pagesCardiotrophin 1Wikipedia ArchivesNo ratings yet
- Outpatient1 minuteQueuingMachineDocument169 pagesOutpatient1 minuteQueuingMachineParisGeronimoNo ratings yet
- Drug Measurement AbbreviationsDocument3 pagesDrug Measurement AbbreviationsAshitakaNo ratings yet
- Common Medical AbbreviationsDocument78 pagesCommon Medical AbbreviationsRAISA N. RASIDNo ratings yet
- Anatomy & Physiology Bootcamp NotesDocument51 pagesAnatomy & Physiology Bootcamp Notesgeorgia robinsonNo ratings yet
- Drugs Affecting The Autonomic Nervous System: 1 AlazarDocument55 pagesDrugs Affecting The Autonomic Nervous System: 1 Alazarsiltanu awokeNo ratings yet
- Newsletter-Fall21-Links 1Document15 pagesNewsletter-Fall21-Links 1api-398712370No ratings yet
- Social Determinants of Health PDF - 3 Per Page NotesDocument8 pagesSocial Determinants of Health PDF - 3 Per Page Notesapi-657470217No ratings yet
- 03 Sympathomimetics-And-Blockers NCM206Document9 pages03 Sympathomimetics-And-Blockers NCM206julinka beyla yansonNo ratings yet
- Fluids and Renal DisorderDocument139 pagesFluids and Renal DisorderLhara MañoNo ratings yet
- 12 Drugs Acting On The Cardiovascular SystemDocument7 pages12 Drugs Acting On The Cardiovascular SystemJAN CAMILLE LENONNo ratings yet
- Antimicrobial Treatment Guidelines For Common Infections enDocument111 pagesAntimicrobial Treatment Guidelines For Common Infections enRoofia VahedianNo ratings yet
- Acute Critical Care Nursing HandoutDocument17 pagesAcute Critical Care Nursing HandoutRuby Ann DimayugaNo ratings yet
- Mohammed H. Eid - The Intensivist-Middle East & ElMarwa For Publishing & Distribution, GN (2019)Document372 pagesMohammed H. Eid - The Intensivist-Middle East & ElMarwa For Publishing & Distribution, GN (2019)Mohamed Moussa100% (1)
- Pharmaceutics 1 (Chapter 7 To 11) BOOKDocument58 pagesPharmaceutics 1 (Chapter 7 To 11) BOOKshahida hassanNo ratings yet
- ENDOCRINE DISORDERS Ms HandoutsDocument14 pagesENDOCRINE DISORDERS Ms HandoutsCatherine FaithNo ratings yet
- Pharma Final ModuleDocument139 pagesPharma Final ModuleQuantum XavierNo ratings yet
- Introduction To PharmacologyDocument119 pagesIntroduction To PharmacologyYzel Vasquez AdavanNo ratings yet
- Fluid and electrolyte balance: Maintaining homeostasisDocument120 pagesFluid and electrolyte balance: Maintaining homeostasisAlessandra MercadoNo ratings yet
- IV Therapy Complications: Local IssuesDocument79 pagesIV Therapy Complications: Local IssuesChannelGNo ratings yet
- Perioperative Nursing ManualDocument101 pagesPerioperative Nursing ManualGabrielle MagdaraogNo ratings yet
- Nursing Student Handbook 2020-2021Document41 pagesNursing Student Handbook 2020-2021serbo81No ratings yet
- Nursing Board Exam Pointers for SingaporeDocument18 pagesNursing Board Exam Pointers for SingaporeHegi Ann AlcalaNo ratings yet
- Dispensing 1 LECDocument10 pagesDispensing 1 LECate aiNo ratings yet
- Pediatric NursingDocument146 pagesPediatric NursingJannele BernadasNo ratings yet
- Tipsy Avant ResumeDocument3 pagesTipsy Avant ResumeTIPSY ANTONYNo ratings yet
- Dokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedDocument54 pagesDokumen - Pub - Current Hospital Medicine Quick Guide For Management of Common Medical Conditions in Acute Care Setting 1stnbspedMahmoud FathyNo ratings yet
- KLE Pharmacy - NPC Brochure 2022Document13 pagesKLE Pharmacy - NPC Brochure 2022Bhaskar PandeyNo ratings yet
- Applying For Security Guard PositionDocument1 pageApplying For Security Guard PositionaNo ratings yet
- Pharma NotesDocument18 pagesPharma Notesseanne kskwkwkaNo ratings yet
- PHA6118 Course Orientation Portfolio 2TAY2022-23 Salonga ForRevision v3Document25 pagesPHA6118 Course Orientation Portfolio 2TAY2022-23 Salonga ForRevision v3christian redotaNo ratings yet
- Nursing Assessment ToolDocument6 pagesNursing Assessment ToolRaniNo ratings yet
- ArrythmiaDocument31 pagesArrythmialubnaNo ratings yet
- UTI GuidelineDocument10 pagesUTI Guidelinecatalin petreNo ratings yet
- Assess client readiness for health changesDocument13 pagesAssess client readiness for health changesDarren VargasNo ratings yet
- PharmacyDocument16 pagesPharmacyJow RamosNo ratings yet
- Medication and Administration C.NDocument286 pagesMedication and Administration C.NJaleto sunkemoNo ratings yet
- April Released ExamDocument31 pagesApril Released ExamSophia BowlesNo ratings yet
- Hospital Pharm NotesmergedDocument152 pagesHospital Pharm NotesmergedShawn Vaughn Allen Silorio100% (1)
- Renal Disorders GuideDocument62 pagesRenal Disorders GuideDardarConstantinoNo ratings yet
- Forms, Documents, and Sample Letters For Organic ProducersDocument20 pagesForms, Documents, and Sample Letters For Organic ProducersAlif AdnanNo ratings yet
- (PHA6129 LAB) Terms, Abbreviations, and DefinitionsDocument7 pages(PHA6129 LAB) Terms, Abbreviations, and DefinitionsNotfor TaoNo ratings yet
- Pharmacy Cbahi Questions 2022Document12 pagesPharmacy Cbahi Questions 2022osama hosni100% (1)
- Brochure The MS Disease Modifying MedicationsDocument16 pagesBrochure The MS Disease Modifying MedicationsBarath R BaskaranNo ratings yet
- Nursing Research - InitialDocument25 pagesNursing Research - InitialNur SanaaniNo ratings yet
- Personal Data SheetDocument8 pagesPersonal Data SheetAlberta Monica Defiesta YubalNo ratings yet
- Guidelines For NursesDocument21 pagesGuidelines For NursesSumayya AhmedNo ratings yet
- Health Assessment - MIDTERM-TRANSDocument36 pagesHealth Assessment - MIDTERM-TRANSShene Claire VigillaNo ratings yet
- Workbook On IV TherapyDocument24 pagesWorkbook On IV TherapyFATIMA MARYAMA USMANNo ratings yet
- Artificial Intelligence in Tracking Solutions For The Logistics in A Hospital in Real TimeDocument84 pagesArtificial Intelligence in Tracking Solutions For The Logistics in A Hospital in Real TimeAmit JagtapNo ratings yet
- Questions From Exam 08.09.22Document12 pagesQuestions From Exam 08.09.22Ismo SNo ratings yet
- NCM 119 Ethicomoral Magna Carta Pages 6 9 1Document4 pagesNCM 119 Ethicomoral Magna Carta Pages 6 9 1Loren SarigumbaNo ratings yet
- Drug Classification, Actions, Indications and Nursing ConsiderationsDocument14 pagesDrug Classification, Actions, Indications and Nursing ConsiderationsLoren SarigumbaNo ratings yet
- Tracheostomy CareDocument5 pagesTracheostomy CareLoren SarigumbaNo ratings yet
- Controlling Components in the Management ProcessDocument3 pagesControlling Components in the Management ProcessLoren SarigumbaNo ratings yet
- MEPERIDINE (Demerol) C A I CDocument3 pagesMEPERIDINE (Demerol) C A I CLoren SarigumbaNo ratings yet
- 119 Anti Sexual Harassment Act of 1995Document5 pages119 Anti Sexual Harassment Act of 1995Loren SarigumbaNo ratings yet
- TheContemporaryWorld BookDocument101 pagesTheContemporaryWorld BookLoren Sarigumba100% (2)
- Globalization of Religion GROUP 2 SECTION A TCWDocument13 pagesGlobalization of Religion GROUP 2 SECTION A TCWLoren SarigumbaNo ratings yet
- NCM118 Week11Document6 pagesNCM118 Week11Loren SarigumbaNo ratings yet
- 15 - TortsDocument6 pages15 - TortsLoren SarigumbaNo ratings yet
- Nurse Close The DoorDocument1 pageNurse Close The DoorLoren SarigumbaNo ratings yet
- Women's Ways of KnowingDocument12 pagesWomen's Ways of KnowingLoren SarigumbaNo ratings yet
- NCM 117: Long Exam 2: Anxiety & Anxiety Disorders Topic OutlineDocument56 pagesNCM 117: Long Exam 2: Anxiety & Anxiety Disorders Topic OutlineLoren SarigumbaNo ratings yet
- The Effect of JobDocument68 pagesThe Effect of JobLoren SarigumbaNo ratings yet
- Drug Calculations Sarigumba BSN 2EDocument1 pageDrug Calculations Sarigumba BSN 2ELoren SarigumbaNo ratings yet
- 123 Quiz PintsDocument3 pages123 Quiz PintsLoren SarigumbaNo ratings yet
- Bubble Pop PintsDocument1 pageBubble Pop PintsLoren SarigumbaNo ratings yet
- Nursing Care of Hearing DisordersDocument6 pagesNursing Care of Hearing DisordersLoren SarigumbaNo ratings yet
- NCM 117: Long Exam 2: Anxiety & Anxiety Disorders Topic OutlineDocument27 pagesNCM 117: Long Exam 2: Anxiety & Anxiety Disorders Topic OutlineLoren Sarigumba0% (1)
- SampleDocument8 pagesSampleAntônioNo ratings yet
- 88 Dean StreetDocument36 pages88 Dean StreetPatrick BatyNo ratings yet
- SilverDocument16 pagesSilversharma_shruti0% (1)
- ConvergeDocument22 pagesConvergekharynconvergeboholNo ratings yet
- Actual Freedom - Made Easy (Print Friendly Edition)Document186 pagesActual Freedom - Made Easy (Print Friendly Edition)Justine100% (5)
- Newton's Laws of Motion Summative TestDocument1 pageNewton's Laws of Motion Summative TestXHiri Pabuaya MendozaNo ratings yet
- KND 3200 eDocument0 pagesKND 3200 eGianna FrolaNo ratings yet
- BARACARBDocument2 pagesBARACARBYudha Satria50% (2)
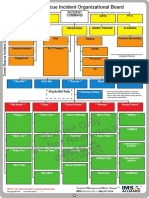
- Sample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardDocument1 pageSample Only Do Not Reproduce: Trench Rescue Incident Organizational BoardLuis Diaz CerdanNo ratings yet
- Orac Charts - BuenisimoDocument92 pagesOrac Charts - BuenisimosanthigiNo ratings yet
- Training ManualDocument41 pagesTraining Manualemiliow_1100% (3)
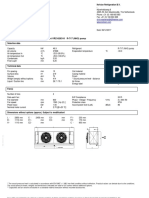
- GSL DIP Phase - 1 Cooler 45kWDocument1 pageGSL DIP Phase - 1 Cooler 45kWMuhasin PallikkalNo ratings yet
- LEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019Document18 pagesLEEA-036 (B) - Academy ITS Practical Training Courses Jan - June 2020 Version 1 October 2019kaito kurabaNo ratings yet
- Design of Temporary Floating Road for Construction SiteDocument6 pagesDesign of Temporary Floating Road for Construction SiteAnonymous hRWwL7pZnCNo ratings yet
- RTWP OptimisationHanFeedbackDocument31 pagesRTWP OptimisationHanFeedbackSeth Mawuli Dedzoe100% (1)
- Mec 323Document68 pagesMec 323VINAY B.SNo ratings yet
- Fundamentals of Wind EnergyDocument24 pagesFundamentals of Wind EnergyMas3odNo ratings yet
- Heliflex Hose CatalogueDocument119 pagesHeliflex Hose CatalogueAugustine DharmarajNo ratings yet
- Edema Paru Kardiogenik Akut Kak TiaraDocument8 pagesEdema Paru Kardiogenik Akut Kak TiaraTyara LarisaNo ratings yet
- Logicroof V-RP enDocument1 pageLogicroof V-RP enCristina DogariNo ratings yet
- Wemco Depurator 2003Document2 pagesWemco Depurator 20031mmahoneyNo ratings yet
- Practical 7 - Angiosperms Marking Guide Exercise 1: Class DicotyledonsDocument3 pagesPractical 7 - Angiosperms Marking Guide Exercise 1: Class DicotyledonsDitiro Maletsanake50% (2)
- Flange Insulation Sets: Technical SpecificationDocument6 pagesFlange Insulation Sets: Technical SpecificationNor Azlan AwangNo ratings yet
- CFD Answer KeyDocument12 pagesCFD Answer KeyRaahini IzanaNo ratings yet
- Miniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDocument4 pagesMiniaturized 90 Degree Hybrid Coupler Using High Dielectric Substrate For QPSK Modulator PDFDenis CarlosNo ratings yet
- Guía de Instalación y Programación: Sistema de Seguridad de 32 ZonasDocument68 pagesGuía de Instalación y Programación: Sistema de Seguridad de 32 ZonasfernanfivNo ratings yet
- Definisi, Karakteristik dan Contoh Aplikasi SIGDocument28 pagesDefinisi, Karakteristik dan Contoh Aplikasi SIGtoyota taaNo ratings yet
- MIND - BODY RelationshipDocument18 pagesMIND - BODY RelationshipvishwabhashaNo ratings yet
- PDM TempDocument2 pagesPDM Tempamit rajputNo ratings yet
- Instapdf - in Bangalore Tourist Places List 674Document31 pagesInstapdf - in Bangalore Tourist Places List 674R K PathamNo ratings yet