You might also like
- Full Test Bank For Environment and Society A Critical Introduction 2Nd Edition by Robbins Hintz Moore PDF Docx Full Chapter ChapterDocument33 pagesFull Test Bank For Environment and Society A Critical Introduction 2Nd Edition by Robbins Hintz Moore PDF Docx Full Chapter Chapterpearlhortonmaich100% (10)
- PMRF 012020 PDFDocument2 pagesPMRF 012020 PDFJenilyn Gonzales Narrido100% (2)
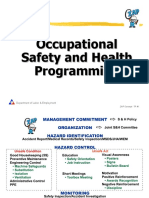
- OSH Programming (Bosh) (Repaired)Document22 pagesOSH Programming (Bosh) (Repaired)Lauro CanceranNo ratings yet
- Phase 1Document7 pagesPhase 1Rizza PardinasNo ratings yet
- Narrative ReportDocument3 pagesNarrative Reportann yucomNo ratings yet
- Arnis Reaction PaperDocument2 pagesArnis Reaction Paperjp gutierrezNo ratings yet
- Fire Safety Inspection Certificate FinalDocument2 pagesFire Safety Inspection Certificate FinalFerdinand M. Turbanos100% (1)
- Rhetorical Analysis of Lyndon B. Johnson's "We Shall Overcome"Document5 pagesRhetorical Analysis of Lyndon B. Johnson's "We Shall Overcome"bethrothenberger75% (8)
- Thirst First Bottling CompanyDocument17 pagesThirst First Bottling CompanyLei Mendoza75% (4)
- Reflection About The Film The CastawayDocument2 pagesReflection About The Film The CastawayFrednixen Bustamante GapoyNo ratings yet
- Module 6 Social SelfDocument36 pagesModule 6 Social SelfElaine PolicarpioNo ratings yet
- MMW Final Exam PDFDocument8 pagesMMW Final Exam PDFRenzo Arvin MatiasNo ratings yet
- Entrep ActivityDocument2 pagesEntrep ActivitySeph Torres100% (1)
- ResumeDocument4 pagesResumeroyarvin0% (1)
- Resume Edit ModeDocument7 pagesResume Edit Modemark jovanNo ratings yet
- Review of Related LiteratureDocument5 pagesReview of Related LiteratureHantini Hana75% (4)
- Lesson 2 Rizal Law The Catholic HeirarchyDocument12 pagesLesson 2 Rizal Law The Catholic HeirarchybryanNo ratings yet
- Form OJT PDSDocument1 pageForm OJT PDSJiehainie Irag33% (3)
- Letters of Support From Future Customers SamplesDocument4 pagesLetters of Support From Future Customers SamplesKai de LeonNo ratings yet
- RRL LayoutDocument4 pagesRRL LayoutKenya Kate GungobNo ratings yet
- Scope and Delimitation of The StudyDocument2 pagesScope and Delimitation of The StudyTrixy ParaneNo ratings yet
- PMMA Psychological Evaluation Announcemen1Document2 pagesPMMA Psychological Evaluation Announcemen1John Vincent D. Reyes100% (1)
- Theoretical and Conceptual DUWTRWHDocument6 pagesTheoretical and Conceptual DUWTRWHReynil LabriagaNo ratings yet
- Filipino PhysicistDocument1 pageFilipino PhysicistJeredPanalagaoAdal100% (1)
- CHAPTER II BIOMETRIC TRACKING SYSTEM FinalDocument13 pagesCHAPTER II BIOMETRIC TRACKING SYSTEM FinalJayr FloresNo ratings yet
- Research Instrument and Data GatheringDocument3 pagesResearch Instrument and Data GatheringGlaiza Mei NatividadNo ratings yet
- Lyrics of Ako Na Lang - Zia QuizonDocument3 pagesLyrics of Ako Na Lang - Zia QuizondaisyNo ratings yet
- Reaction PaperDocument5 pagesReaction PaperNorman A. Bernabe100% (1)
- ResumeDocument3 pagesResumeNeil Alexis M. MartinezNo ratings yet
- PLMAT CoverageDocument1 pagePLMAT CoverageReign SinocruzNo ratings yet
- Task 3 - Evaluate - Art CritiqueDocument2 pagesTask 3 - Evaluate - Art CritiqueValerie Ann Opina50% (2)
- AcknowledgementDocument5 pagesAcknowledgementiyaNo ratings yet
- Chegg - Chapter Three PDFDocument131 pagesChegg - Chapter Three PDFTeam DriveNo ratings yet
- Kapit Sa Patalim: Household Service WorkersDocument2 pagesKapit Sa Patalim: Household Service WorkersRodel Novesteras Claus0% (1)
- My Reaction Paper in RWC About Love Story by Taylor Swift by JM LIMDocument1 pageMy Reaction Paper in RWC About Love Story by Taylor Swift by JM LIMTRISTANE ERIC SUMANDENo ratings yet
- Filipinos Are Not Fond of Eating VegetablesDocument2 pagesFilipinos Are Not Fond of Eating VegetablesDaniela Claire FranciscoNo ratings yet
- Nature Spring HistoryDocument21 pagesNature Spring HistoryAnonymous jG86rkNo ratings yet
- 1-4 CompoundInterest 12302011Document28 pages1-4 CompoundInterest 12302011Nemo MaelNo ratings yet
- Application Form For Shifter/Transferee: Personal InformationDocument3 pagesApplication Form For Shifter/Transferee: Personal InformationPatricia Guerra100% (1)
- How Do People Find Information That Matches Their Needs?Document1 pageHow Do People Find Information That Matches Their Needs?Gen Ira Tampus100% (2)
- Layson - R GE 15 ULOb Let's Analyze PDFDocument2 pagesLayson - R GE 15 ULOb Let's Analyze PDFAyah LaysonNo ratings yet
- VACANT TIME PrintDocument9 pagesVACANT TIME PrintNeil Virgel Inding0% (1)
- Biography of Prominent FilipinoDocument2 pagesBiography of Prominent FilipinoLouennaNo ratings yet
- Lto Guidelines On LED LightsDocument4 pagesLto Guidelines On LED LightsL Dominguez Torres-Damian100% (1)
- SCHOLARNIGOVDocument6 pagesSCHOLARNIGOVendayaavrylleNo ratings yet
- Tanging YamanDocument3 pagesTanging YamanMai Cuenco100% (1)
- Alfredo Lazarte JuinioDocument5 pagesAlfredo Lazarte JuinioStevenzel Eala EstellaNo ratings yet
- Ta LaguertaDocument3 pagesTa LaguertaPatson OpidoNo ratings yet
- Key PartnersDocument4 pagesKey PartnersMostafa AboheifNo ratings yet
- Vicinity MapDocument1 pageVicinity MapJonathan Marvin DueNo ratings yet
- Ro4a Peso DirectoryDocument4 pagesRo4a Peso DirectoryRaymund Madayag100% (1)
- Having My On The Job Training in DENR PENRODocument2 pagesHaving My On The Job Training in DENR PENROReymond Lovendino100% (2)
- JOHN LEVY PORCA - Experiment No. 1 Common Chemistry Laboratory EquipmentDocument3 pagesJOHN LEVY PORCA - Experiment No. 1 Common Chemistry Laboratory EquipmentLevy PorcaNo ratings yet
- MomentumDocument23 pagesMomentumAlbieJane CatotoNo ratings yet
- The Problem and Its ScopeDocument24 pagesThe Problem and Its Scopemaryil100% (1)
- Full Info (Educ & Career) : Anacleto Del RosarioDocument4 pagesFull Info (Educ & Career) : Anacleto Del RosarioMark Lonne Peliño100% (1)
- Chapter 3Document6 pagesChapter 3Sheldon BazingaNo ratings yet
- Reaction Paper RRLDocument1 pageReaction Paper RRLKatrina Ponce0% (1)
- Philhealth FormDocument2 pagesPhilhealth FormJaymart Ingreso100% (1)
- Reminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)Document3 pagesReminders:: UHC v.1 January 2020 Philhealth Identification Number (Pin)Jhepoy Lumanglas AstillaNo ratings yet
- Philhealth FormDocument2 pagesPhilhealth FormJordan CabreraNo ratings yet
- R E M Ind Er S:: UHC v.1 January 2020Document2 pagesR E M Ind Er S:: UHC v.1 January 2020Melody Frac ZapateroNo ratings yet
- Math Q1W8Document2 pagesMath Q1W8Arvin DayagNo ratings yet
- Action Plan Math 5Document1 pageAction Plan Math 5Arvin Dayag100% (1)
- Acknowledgement-receipt-School 2 (2) 365Document4 pagesAcknowledgement-receipt-School 2 (2) 365Arvin DayagNo ratings yet
- Lesson Plan For Making Extension COT Sir AlexDocument3 pagesLesson Plan For Making Extension COT Sir AlexArvin Dayag75% (4)
- 2019 Moving Up Ceremony and Recognition RitesDocument8 pages2019 Moving Up Ceremony and Recognition RitesArvin DayagNo ratings yet
- Department of Education: Republic of The PhilippinesDocument2 pagesDepartment of Education: Republic of The PhilippinesArvin DayagNo ratings yet
- Grades 1 To 12 Daily Lesson Log: I.Layunin (Objectives)Document2 pagesGrades 1 To 12 Daily Lesson Log: I.Layunin (Objectives)Arvin Dayag100% (1)
- 2019 Ipcrf Defense-ArvinDocument7 pages2019 Ipcrf Defense-ArvinArvin DayagNo ratings yet
- School Form 2 (SF2) Daily Attendance Report of Learners: 102868 2020 - 2021 Bauan ES Grade 6 SapphireDocument3 pagesSchool Form 2 (SF2) Daily Attendance Report of Learners: 102868 2020 - 2021 Bauan ES Grade 6 SapphireArvin DayagNo ratings yet
- EO On Establishment of Kasambahay DeskDocument2 pagesEO On Establishment of Kasambahay DeskCarmelita Agudana100% (2)
- Flow Chart On PresumptionsDocument1 pageFlow Chart On PresumptionsishanNo ratings yet
- Endorsement Letter From The Head of InstitutionDocument2 pagesEndorsement Letter From The Head of InstitutionkavinNo ratings yet
- Hijinks and Spy RingsDocument4 pagesHijinks and Spy RingsRandemetsadNo ratings yet
- High Court Case Types and Their Full FormsDocument56 pagesHigh Court Case Types and Their Full FormssoneflyerNo ratings yet
- Robinsons LLP: From: Sam Smith To: Rebecca Jones Subject: Review of N265 List of Documents Ref. No. AJ/AIL/18/.425Document8 pagesRobinsons LLP: From: Sam Smith To: Rebecca Jones Subject: Review of N265 List of Documents Ref. No. AJ/AIL/18/.425Okew SojaNo ratings yet
- Term Time OnlyDocument9 pagesTerm Time Onlyips.tineretNo ratings yet
- Santos Jr. Vs LlamasDocument2 pagesSantos Jr. Vs LlamasLu CasNo ratings yet
- Radical Tasmania Volume 2 The Selected HistoriesDocument196 pagesRadical Tasmania Volume 2 The Selected HistoriesFred StevensonNo ratings yet
- Bayan V Ermita G.R. NO. 169838 April 25, 2006Document19 pagesBayan V Ermita G.R. NO. 169838 April 25, 2006MWinbee VisitacionNo ratings yet
- 3.ESTATE OF K. H. HEMADY, Deceased, vs. LUZON SURETY CO., INC.Document2 pages3.ESTATE OF K. H. HEMADY, Deceased, vs. LUZON SURETY CO., INC.Yvon BaguioNo ratings yet
- Mahatma GandhiDocument2 pagesMahatma GandhiN seriesNo ratings yet
- Mitchell Press ReleaseDocument4 pagesMitchell Press ReleaseWSLSNo ratings yet
- Case CommentDocument2 pagesCase Commentsanjana sethNo ratings yet
- Association of Small Land Owners VS Secretary of Agrarian Reform - Police Power and Eminent DomainDocument2 pagesAssociation of Small Land Owners VS Secretary of Agrarian Reform - Police Power and Eminent DomainJuvial Guevarra BostonNo ratings yet
- OA.886.17.J.4.2019-SHSakharwade-DD of PromotionDocument16 pagesOA.886.17.J.4.2019-SHSakharwade-DD of PromotionssandeepNo ratings yet
- © 2018 CengageDocument25 pages© 2018 CengageAditya NatalNo ratings yet
- Sentence Correction - English Aptitude MCQ Questions and Answers Page-3 Section-1 - 1603796318303Document4 pagesSentence Correction - English Aptitude MCQ Questions and Answers Page-3 Section-1 - 1603796318303LikeNo ratings yet
- European External Action ServiceDocument6 pagesEuropean External Action Servicekarma.designer.01No ratings yet
- Motion For Postponement - Quintin Pagulayan Jr.Document3 pagesMotion For Postponement - Quintin Pagulayan Jr.Salvado and Chua Law OfficesNo ratings yet
- Termination of Korporate KontractsDocument7 pagesTermination of Korporate KontractsRosetta Rashid’s McCowan ElNo ratings yet
- Frustration of Partnership Firm - : Aishani Chakraborty (2019118)Document4 pagesFrustration of Partnership Firm - : Aishani Chakraborty (2019118)Aishani ChakrabortyNo ratings yet
- Ronald Reagan and The Rise of ConservatismDocument7 pagesRonald Reagan and The Rise of ConservatismCeles noNo ratings yet
- Smith Bell v. Sotelo Matti, 44 Phil 874Document9 pagesSmith Bell v. Sotelo Matti, 44 Phil 874BernsNo ratings yet
- Bonafide Certificate RequestDocument1 pageBonafide Certificate RequestAkshit PatelNo ratings yet
- Case Commentary On M Nagraj V UOIDocument11 pagesCase Commentary On M Nagraj V UOIAmartya Vikram SinghNo ratings yet
- Legal Practice and Ethics Notesp PDFDocument4 pagesLegal Practice and Ethics Notesp PDFRishwanteeNo ratings yet
- Land Acquisition in India PDFDocument11 pagesLand Acquisition in India PDFswaraj patilNo ratings yet