You might also like
- Trauma OkuliDocument50 pagesTrauma Okuliaditya brahmantio sujakaNo ratings yet
- Dermatology Lectures JRRMMCDocument10 pagesDermatology Lectures JRRMMCGi Em100% (1)
- PEDIA - Drug Study & NCPDocument24 pagesPEDIA - Drug Study & NCPCzarina Mae Lomboy100% (1)
- CataractDocument24 pagesCataractNeela Kandan100% (1)
- Occupational Hazards in Dental, Textile Industry and MechanicDocument20 pagesOccupational Hazards in Dental, Textile Industry and MechanicimtahifNo ratings yet
- Ocular Emergencies-Sept2013 PDFDocument22 pagesOcular Emergencies-Sept2013 PDFKaramsi Gopinath NaikNo ratings yet
- Red Eye TableDocument2 pagesRed Eye TableFatimah AlsultanNo ratings yet
- ErythromycinDocument1 pageErythromycinJozarine ChelseaNo ratings yet
- Integumentary SystemDocument4 pagesIntegumentary SystemArnie Jean SalazarNo ratings yet
- Endophthalmitis: Current Trends, Drugs and Protocols: Aditya Verma, Vinata Muralidharan and Eesh NigamDocument10 pagesEndophthalmitis: Current Trends, Drugs and Protocols: Aditya Verma, Vinata Muralidharan and Eesh NigamHerman Kurt Ludvik100% (1)
- Care For Patients With Alteration in Perception and CoordinationDocument12 pagesCare For Patients With Alteration in Perception and Coordinationevlujtrep9690100% (1)
- Drug StudyDocument3 pagesDrug StudyNicole Rachelyn MartinNo ratings yet
- Name of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesDocument2 pagesName of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesMichelle Dona MirallesNo ratings yet
- Sarcoptes Scabei Var. HumanusDocument2 pagesSarcoptes Scabei Var. HumanusZai Ra DianaNo ratings yet
- Outline Notes of CS 27 - Ocular Orbital TraumaDocument8 pagesOutline Notes of CS 27 - Ocular Orbital TraumaTaif SalimNo ratings yet
- CorneaDocument5 pagesCorneaMohamed GhanemNo ratings yet
- Drug Study NurseryDocument6 pagesDrug Study NurseryTanya Victoria Lean ClaudioNo ratings yet
- Permethrin 5% Cream: Medication MOA Instruction CommentsDocument1 pagePermethrin 5% Cream: Medication MOA Instruction CommentsChron MedNo ratings yet
- Micro paraDocument2 pagesMicro parafeminaNo ratings yet
- Diabetic Foot Hajera FinalDocument38 pagesDiabetic Foot Hajera FinalAfifah SelamatNo ratings yet
- Animal BitesflowDocument1 pageAnimal BitesflowRajanNo ratings yet
- Orbital and Ocular TumorsDocument13 pagesOrbital and Ocular TumorsstarlytexpressNo ratings yet
- Care For Patients With Alteration in Perception and CoordinationDocument13 pagesCare For Patients With Alteration in Perception and Coordinationevlujtrep9690No ratings yet
- Part 1Document15 pagesPart 1solimanmahmoudaNo ratings yet
- (Ophtha) Ocular Emergenices - Dr. VillalvaDocument6 pages(Ophtha) Ocular Emergenices - Dr. VillalvaPatricia ManaliliNo ratings yet
- Conjunctivitis: Radang Konjungtiva Yang Menutupi Belakang Kelopak Dan Bola Mata, Dalam Bentuk Akut Maupun KronisDocument18 pagesConjunctivitis: Radang Konjungtiva Yang Menutupi Belakang Kelopak Dan Bola Mata, Dalam Bentuk Akut Maupun KronisnasikaceliaNo ratings yet
- 2.06 - Bacterial InfectionsDocument8 pages2.06 - Bacterial InfectionsMaria CanabeNo ratings yet
- SFATDocument9 pagesSFATKateNo ratings yet
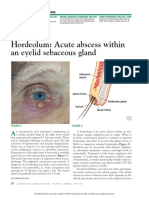
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- Endodontic Emergency (Dr. Imran)Document2 pagesEndodontic Emergency (Dr. Imran)aelessyaNo ratings yet
- Kul Mata Merah PDFDocument56 pagesKul Mata Merah PDFMuhammad HasanNo ratings yet
- Insect Bites Stings 11 530kDocument2 pagesInsect Bites Stings 11 530kCM GonzalezNo ratings yet
- Periodontal Abscess Gingival AbscessDocument2 pagesPeriodontal Abscess Gingival AbscessNur Kamaliah100% (1)
- Tinywow Communicable-Diseases 48897647 4Document1 pageTinywow Communicable-Diseases 48897647 4JULIUS CEZAR QUINAYNo ratings yet
- Bacterial Skin Infections BmlsDocument5 pagesBacterial Skin Infections Bmls97w25v8c82No ratings yet
- Drug Study With NCPDocument4 pagesDrug Study With NCPJoanne Kathleen SantolicesNo ratings yet
- Ophthalmology NotesDocument79 pagesOphthalmology NotesWise AmroNo ratings yet
- Skin AbnormalsDocument2 pagesSkin AbnormalsJp CasperNo ratings yet
- Causative Agent Characteristic Symptom 1 Management: Surgery Is The Most Important Modality For MalignantDocument2 pagesCausative Agent Characteristic Symptom 1 Management: Surgery Is The Most Important Modality For MalignantJp CasperNo ratings yet
- Disease and Cause Manifestation Treatment Prevention Bacteria SignsDocument14 pagesDisease and Cause Manifestation Treatment Prevention Bacteria SignsMc MagtibayNo ratings yet
- ConjunctivitisDocument4 pagesConjunctivitisKumar ShivamNo ratings yet
- Acne, Physical Dermatoses, Bacterial InfectiosDocument35 pagesAcne, Physical Dermatoses, Bacterial InfectiosRiena Austine Leonor NarcillaNo ratings yet
- CD Additional LessonsDocument13 pagesCD Additional LessonsAlma Janella TOSINONo ratings yet
- Wound Care ProductsDocument7 pagesWound Care ProductsKaye Marie OportoNo ratings yet
- Open Fractures in Ortho PatientsDocument23 pagesOpen Fractures in Ortho PatientsCharisse Ann GasatayaNo ratings yet
- Animal Bite Flowchart: Patient Comes in at ER With Animal BiteDocument1 pageAnimal Bite Flowchart: Patient Comes in at ER With Animal BiteJonathan JumalonNo ratings yet
- Aseptic Technique: Wound Assessment On A Patient (Open or Closed)Document4 pagesAseptic Technique: Wound Assessment On A Patient (Open or Closed)AbigailNo ratings yet
- Gochi Notes: Immuno-Allergy Part Vi Lecturer: Dra. Eva DizonDocument2 pagesGochi Notes: Immuno-Allergy Part Vi Lecturer: Dra. Eva DizonJustin TayabanNo ratings yet
- Ipo 14 2 081Document2 pagesIpo 14 2 081Debora AzevedoNo ratings yet
- Fiche Diphoterine enDocument2 pagesFiche Diphoterine enpeksNo ratings yet
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocument3 pagesThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9No ratings yet
- Skin Care For HealthDocument3 pagesSkin Care For HealthGin MananganNo ratings yet
- COMPLICATIONSDocument41 pagesCOMPLICATIONSChethana NagaNo ratings yet
- Acute Periodontal Conditions: Sheet 11Document3 pagesAcute Periodontal Conditions: Sheet 11Jwana MahafzaNo ratings yet
- ToddlerDocument15 pagesToddlerCARL JOHN MANALONo ratings yet
- Ophtha ReviewerDocument3 pagesOphtha ReviewerToni Sy EncinaresNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJulia Michelle SerranoNo ratings yet
- Rash Diagnosis Cheat Sheet: EmergencyDocument1 pageRash Diagnosis Cheat Sheet: Emergencykdlsfk kajjksolsNo ratings yet
- Ozempic 1mg Cmi v3.0Document11 pagesOzempic 1mg Cmi v3.0Kenny KeganNo ratings yet
- Checklist PULSE RATE.V2Document1 pageChecklist PULSE RATE.V2chanise casemNo ratings yet
- Major ProjectDocument11 pagesMajor Projectapi-662080993No ratings yet
- Child Abuse Is Any Behaviour That Harms A ChildDocument2 pagesChild Abuse Is Any Behaviour That Harms A ChildThenaNo ratings yet
- Self Completion Medical History Form - PregnancyDocument4 pagesSelf Completion Medical History Form - PregnancymerjenNo ratings yet
- Upper Gastrointestinal Bleeding (UGIB) : Practice EssentialsDocument52 pagesUpper Gastrointestinal Bleeding (UGIB) : Practice EssentialsrishaNo ratings yet
- Laporan Pemantauan Terapi Obat 2022Document728 pagesLaporan Pemantauan Terapi Obat 2022hamidahNo ratings yet
- NCM 109Document14 pagesNCM 109Christine Lindsey BenaroNo ratings yet
- Code Blue Group-Psychiatry History FormatDocument10 pagesCode Blue Group-Psychiatry History FormatsakariyeNo ratings yet
- Report HPV, Shingles and Chicken PoxDocument4 pagesReport HPV, Shingles and Chicken PoxJarold PerezNo ratings yet
- Eczema DR Ahmed KamelDocument52 pagesEczema DR Ahmed KamelMostafa EidNo ratings yet
- Brain On FireDocument5 pagesBrain On FireJane LaquihonNo ratings yet
- 2 - Comprehension Passage - XiDocument5 pages2 - Comprehension Passage - XiAfarna The TrioNo ratings yet
- Pediatric Lymphomas and Solid Tumors 0Document153 pagesPediatric Lymphomas and Solid Tumors 0yogendra madanNo ratings yet
- QuizDocument3 pagesQuizKomella PrakasamNo ratings yet
- Good Thesis Statement For Heart DiseaseDocument5 pagesGood Thesis Statement For Heart Diseasemarilynmarieboston100% (2)
- Tetanus Neonatorum LectureDocument11 pagesTetanus Neonatorum LectureJackNo ratings yet
- Blood Product Transfusion in Adults: Indications, Adverse Reactions, and ModificationsDocument9 pagesBlood Product Transfusion in Adults: Indications, Adverse Reactions, and ModificationsYeseniaNo ratings yet
- 07 Blood Pressure Abnormality 1-8-2021 配布用Document22 pages07 Blood Pressure Abnormality 1-8-2021 配布用Lan NguyenNo ratings yet
- Physical Rehabilitation Medicine Terms - THERAPY INSIGHTSDocument11 pagesPhysical Rehabilitation Medicine Terms - THERAPY INSIGHTSbaji sharifNo ratings yet
- Anti Cancer HerbsDocument15 pagesAnti Cancer HerbsElena EvtimovaNo ratings yet
- PAR Q FORM (Pre Activity Readiness Questionnaire) With COVID-19 (FINAL)Document2 pagesPAR Q FORM (Pre Activity Readiness Questionnaire) With COVID-19 (FINAL)Jhona Marie FuellasNo ratings yet
- 07 Sepsis - Dr. Sutrisno, M.Kes., SP - OG., Subsp. ONK.Document31 pages07 Sepsis - Dr. Sutrisno, M.Kes., SP - OG., Subsp. ONK.Syahid PutraNo ratings yet
- Peoria County Booking Sheet 08/05/13Document6 pagesPeoria County Booking Sheet 08/05/13Journal Star police documentsNo ratings yet
- UNC Childrens Diagnosis and Management HAP VAP Nov 2021Document7 pagesUNC Childrens Diagnosis and Management HAP VAP Nov 2021adhitiaNo ratings yet
- Thesis On Acne ProblemDocument4 pagesThesis On Acne Problemveronicagarciaalbuquerque100% (2)
- Sinonasal Outcome Test (SNOT) ScoreDocument1 pageSinonasal Outcome Test (SNOT) ScoreElfawizzyNo ratings yet
- DyslipidemiaDocument21 pagesDyslipidemiaBasil HussamNo ratings yet
- Hypertension in PregnancyDocument29 pagesHypertension in PregnancyArchana KumariNo ratings yet
- Oral Squamous Cell Carcinoma in Patients Twenty Years of Age orDocument6 pagesOral Squamous Cell Carcinoma in Patients Twenty Years of Age orSezen AltındişNo ratings yet