You might also like
- Bodily Changes in Pain, Hunger, Fear and Rage - An Account of Recent Researches Into the Function of Emotional Excitement (1927)From EverandBodily Changes in Pain, Hunger, Fear and Rage - An Account of Recent Researches Into the Function of Emotional Excitement (1927)Rating: 5 out of 5 stars5/5 (1)
- The Basics: A Comprehensive Outline of Nursing School ContentFrom EverandThe Basics: A Comprehensive Outline of Nursing School ContentRating: 5 out of 5 stars5/5 (3)
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
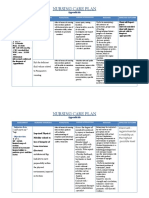
- Nursing Care Plan Age: 60 Years OldDocument4 pagesNursing Care Plan Age: 60 Years OldLouise GudmalinNo ratings yet
- NCP NewDocument16 pagesNCP Newmsfts.No ratings yet
- Name: Age/Sex: Medical Diagnosis: Nursing Diagnosis: Short Term Goal: Long Term GoalDocument5 pagesName: Age/Sex: Medical Diagnosis: Nursing Diagnosis: Short Term Goal: Long Term GoalThoLitz AguinaldoNo ratings yet
- Nursing Care Plan: Acute PainDocument4 pagesNursing Care Plan: Acute PainEvet VaxbmNo ratings yet
- College of Nursing and Allied Medical Sciences: WesleyanDocument3 pagesCollege of Nursing and Allied Medical Sciences: WesleyanPrince Juzzel Banag100% (1)
- Nursing Care PlanDocument2 pagesNursing Care PlanMariel GamaloNo ratings yet
- Subjetive: Long Term: Independent:: RationaleDocument1 pageSubjetive: Long Term: Independent:: RationaleRyann BuayaNo ratings yet
- UntitledDocument7 pagesUntitledElla MayNo ratings yet
- Tah BsoDocument27 pagesTah BsoCephradine DolienteNo ratings yet
- Appendectomy - NCPDocument6 pagesAppendectomy - NCPRhenzes HaraNo ratings yet
- Nursing Care Plan For CholecystitisDocument4 pagesNursing Care Plan For CholecystitisEemyaj Jaymee88% (8)
- NCP EctopicDocument1 pageNCP Ectopicmusicath_07No ratings yet
- NCP DiverticulitisDocument6 pagesNCP DiverticulitisLovely Cacapit100% (1)
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- SKYLA FIESTA NCP (Acute Pancreatitis)Document4 pagesSKYLA FIESTA NCP (Acute Pancreatitis)Skyla FiestaNo ratings yet
- Beronio, Gracel Caye M. CMC Module 6 GI Pedia (Nursing Care Plans)Document5 pagesBeronio, Gracel Caye M. CMC Module 6 GI Pedia (Nursing Care Plans)Gracel Caye Maon BeronioNo ratings yet
- Ineffective Tissue PerfusionDocument3 pagesIneffective Tissue Perfusionkimglaidyl bontuyanNo ratings yet
- Subjective:: Davao Doctor'S College Nursing Program Nursing Care PlanDocument4 pagesSubjective:: Davao Doctor'S College Nursing Program Nursing Care PlanJEVEE JEAN BETTERNo ratings yet
- MS Soapie #1Document2 pagesMS Soapie #1Fatima KateNo ratings yet
- Case Scenario 5 NCPDocument10 pagesCase Scenario 5 NCPkdfhjfhfNo ratings yet
- Short Term Goal: After 1 Hour of Short Term Goal: After 1Document2 pagesShort Term Goal: After 1 Hour of Short Term Goal: After 1Jordz PlaciNo ratings yet
- UntitledDocument5 pagesUntitledJayelles Dixien JuguilonNo ratings yet
- NCP Ruq PainDocument3 pagesNCP Ruq PainKristine YoungNo ratings yet
- Or NCPDocument5 pagesOr NCPjelopigar921No ratings yet
- NCP Proper Assessment Explanation of The Problem Objective Nursing Interventions Rationale EvaluationDocument4 pagesNCP Proper Assessment Explanation of The Problem Objective Nursing Interventions Rationale EvaluationMarc Jordan EstebanNo ratings yet
- Pain - Post Partum MotherDocument2 pagesPain - Post Partum Motherulrikov91% (11)
- Nursing-Care-Plan 4Document4 pagesNursing-Care-Plan 4Christine CornagoNo ratings yet
- Assessment Planning Intervention Evaluation: Subjective Short Term Goal: Independent Short Term GoalDocument2 pagesAssessment Planning Intervention Evaluation: Subjective Short Term Goal: Independent Short Term GoalGlaiza FabiaNo ratings yet
- Appendix B Nursing Care Plan Clinical Portait Assessment: Received PatientDocument14 pagesAppendix B Nursing Care Plan Clinical Portait Assessment: Received Patientjopearl18No ratings yet
- Springfield Technical Community College School of Nursing NURS 202-Nursing Care PlanDocument1 pageSpringfield Technical Community College School of Nursing NURS 202-Nursing Care Plannata654dNo ratings yet
- Corrected NCP Case 3 Intrapartum NCPDocument2 pagesCorrected NCP Case 3 Intrapartum NCPReyzel PahunaoNo ratings yet
- Nursing Care Plan For Angina Pectoris NCPDocument2 pagesNursing Care Plan For Angina Pectoris NCPkarthi karthi100% (1)
- Revised NCP 1-3Document6 pagesRevised NCP 1-3MarcieNo ratings yet
- BSN 1 H Case Application Nursing Care PlanDocument3 pagesBSN 1 H Case Application Nursing Care PlanAntonio EscotoNo ratings yet
- NCP (Appendicitis)Document3 pagesNCP (Appendicitis)Jenny Ajoc100% (1)
- Abortion BSN 0PR-2: Case Study of BelleDocument27 pagesAbortion BSN 0PR-2: Case Study of BellekervinNo ratings yet
- 2 PlanDocument8 pages2 PlanAyobami AdeleyeNo ratings yet
- Acute Pain Related To Complications of Dengue Hemorrhagic Fever As Evidenced by Enlarged LiverDocument3 pagesAcute Pain Related To Complications of Dengue Hemorrhagic Fever As Evidenced by Enlarged LiverAlyssa marieNo ratings yet
- Cues and Objectives Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationDocument4 pagesCues and Objectives Explanation of The Problem Goals and Objectives Interventions Rationale EvaluationShaina Fe RabaneraNo ratings yet
- Norbe COMFORT MEASURESDocument10 pagesNorbe COMFORT MEASURESMarlo Dañez NorbeNo ratings yet
- CS NCPDocument2 pagesCS NCPElbert ViernezaNo ratings yet
- Ob NCP 2Document2 pagesOb NCP 2Kimberly Mondala (SHS)No ratings yet
- Nursing Care Plan Related To Pospartum HemmorhageDocument5 pagesNursing Care Plan Related To Pospartum HemmorhageAsmin BalahNo ratings yet
- NCPDocument18 pagesNCPStephanie Villanueva AdvinculaNo ratings yet
- Case StudyDocument8 pagesCase Studyjds6z4sgfwNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanShania Erika EnajeNo ratings yet
- NCP 1Document4 pagesNCP 1Jezrale FameNo ratings yet
- NCP Severe Labor PainDocument3 pagesNCP Severe Labor PainPaolo EspinosaNo ratings yet
- NCP Acute PainDocument3 pagesNCP Acute PainSony Montaño CañeteNo ratings yet
- NCP For CholecystitisDocument9 pagesNCP For Cholecystitisjmravago220% (1)
- Nursing Care PlanDocument4 pagesNursing Care PlanChrizelle FlorentinoNo ratings yet
- Data Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDocument4 pagesData Nursing Diagnos IS Scientific Backgrou ND Goal/Objective Nursing Interventions Rationale EvaluationDienizs LabiniNo ratings yet
- Acutepain RevisedDocument3 pagesAcutepain RevisedAndrea AutorNo ratings yet
- Cues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale EvaluationDocument11 pagesCues Nursing Diagnosis Scientific Basis Objectives Nursing Intervention Rationale Evaluationjoyrena ochondraNo ratings yet
- On the Curability of Certain Forms of Insanity, Epilepsy, Catalepsy, and Hysteria in FemalesFrom EverandOn the Curability of Certain Forms of Insanity, Epilepsy, Catalepsy, and Hysteria in FemalesNo ratings yet
- Basics of RainforestsDocument14 pagesBasics of RainforestspsrelianceNo ratings yet
- Ocrsm Assignment 1Document13 pagesOcrsm Assignment 1Vaishnavi LoyaNo ratings yet
- I - Infowatch 16-30 Jun 2023Document141 pagesI - Infowatch 16-30 Jun 2023Suman MondalNo ratings yet
- CC W3 AWS Basic InfraDocument57 pagesCC W3 AWS Basic InfraMuhammad Tehseen KhanNo ratings yet
- Dokumen - Tips Strength of Materials 5691845f3ea8eDocument13 pagesDokumen - Tips Strength of Materials 5691845f3ea8eJay GeeNo ratings yet
- Azam in 30 DuaDocument3 pagesAzam in 30 DuafaizaninNo ratings yet
- AC405 Assignment R185840RDocument3 pagesAC405 Assignment R185840RDiatomspinalcordNo ratings yet
- STEP English (1-18) All Worksheets 2020Document134 pagesSTEP English (1-18) All Worksheets 2020Shema ZulfiqarNo ratings yet
- Teaching & Learning Activities: Biology (Sb015) - PelajarDocument2 pagesTeaching & Learning Activities: Biology (Sb015) - PelajarLeevandraaNo ratings yet
- Architectural Thesis PDFDocument7 pagesArchitectural Thesis PDFSuresh Balaji0% (1)
- Drawing List: Infrastructure / 7100 - MV Power Duct Network Rev. NoDocument2 pagesDrawing List: Infrastructure / 7100 - MV Power Duct Network Rev. NosayedNo ratings yet
- ISTH v50 Porto Rico 2006 Trabalho Filme Morango OFSDocument169 pagesISTH v50 Porto Rico 2006 Trabalho Filme Morango OFSAlexandra MamedeNo ratings yet
- Modules in Grade 12: Quarter 1 - Week 3 Academic Track - StemDocument23 pagesModules in Grade 12: Quarter 1 - Week 3 Academic Track - StemZenarose MirandaNo ratings yet
- Churros (Homemade Recipe With Step by Step Photos) - Cooking ClassyDocument1 pageChurros (Homemade Recipe With Step by Step Photos) - Cooking ClassyRyleigh NoelNo ratings yet
- Suction Pile and FoundationDocument19 pagesSuction Pile and FoundationhaydarburedahNo ratings yet
- Offer and Acceptance:: Lapse of An OfferDocument12 pagesOffer and Acceptance:: Lapse of An OfferPriya AroraNo ratings yet
- RoE - T9 & T10 Research v.2Document1 pageRoE - T9 & T10 Research v.2Susa Na100% (1)
- Resume - Lifestyle Medicine RDDocument1 pageResume - Lifestyle Medicine RDapi-338995106No ratings yet
- Design Calculation of Gantry GirderDocument7 pagesDesign Calculation of Gantry GirderKushal ChhetriNo ratings yet
- DEH-1250MPG DEH-1250MP: Owner's Manual Manual de Instrucciones Manual Do ProprietárioDocument80 pagesDEH-1250MPG DEH-1250MP: Owner's Manual Manual de Instrucciones Manual Do ProprietárioMoezz Asif Research Associate-Faculty of Avionics EngineeringNo ratings yet
- Affordable HousingDocument12 pagesAffordable HousingTenzin KesangNo ratings yet
- BAMBOO U - 5 Ways To Process BambooDocument11 pagesBAMBOO U - 5 Ways To Process BambooeShappy HomeNo ratings yet
- Your Paragraph TextDocument11 pagesYour Paragraph TextTalha AamirNo ratings yet
- Dzone Refcard 292 Advanced Kubernetes 2020 PDFDocument9 pagesDzone Refcard 292 Advanced Kubernetes 2020 PDFLeonardo Moreno ForeroNo ratings yet
- Chapter 1: IntroductionDocument34 pagesChapter 1: IntroductionIntan AifatikaNo ratings yet
- Blitzscales 14Document72 pagesBlitzscales 14Andrej Bašić100% (3)
- Project Report On Working-CapitalDocument74 pagesProject Report On Working-Capitalravikant2105100% (1)
- 118CP Selection of CP Systems For Reinforced Concrete StructuresDocument15 pages118CP Selection of CP Systems For Reinforced Concrete StructuresWill NashNo ratings yet
- Proposal 4psDocument6 pagesProposal 4psCaridad Avila67% (3)
- Kernel One SBDocument140 pagesKernel One SBronanNo ratings yet