You might also like
- Skip Lid Sling CertificateDocument1 pageSkip Lid Sling CertificateIsaac NnakwuNo ratings yet
- Skip Lid-03P1 TO 03P4Document1 pageSkip Lid-03P1 TO 03P4Isaac NnakwuNo ratings yet
- Holding Tank AGS-HT-001Document1 pageHolding Tank AGS-HT-001Isaac NnakwuNo ratings yet
- Round Webbing Sling - 26782Document1 pageRound Webbing Sling - 26782Godfred QuarmNo ratings yet
- Centrifuge StandDocument1 pageCentrifuge StandIsaac NnakwuNo ratings yet
- Beam Clamp Thorough Exam ReportsDocument21 pagesBeam Clamp Thorough Exam Reportsdele jimohNo ratings yet
- A-Star Testing & Inspection (S) Pte LTD: Magnetic Particle Testing ReportDocument4 pagesA-Star Testing & Inspection (S) Pte LTD: Magnetic Particle Testing ReportHari KarthickNo ratings yet
- Casing Stabbing BoardDocument1 pageCasing Stabbing BoardRanjithNo ratings yet
- 8689-2018 Sixco Chain SlingDocument2 pages8689-2018 Sixco Chain SlingAnonymous wuugFvOBjZNo ratings yet
- LIFTING EQUIPMENT INSPECTION REPORTDocument3 pagesLIFTING EQUIPMENT INSPECTION REPORTMohamed Yasir100% (1)
- Wheel Loader Forklift Thorough Exam ReportDocument2 pagesWheel Loader Forklift Thorough Exam ReportRanjithNo ratings yet
- LIFTING EQUIPMENT INSPECTION REPORTDocument10 pagesLIFTING EQUIPMENT INSPECTION REPORTRanjithNo ratings yet
- 3. MANUAL CHAIN BLOCK 1.5T - CopyDocument2 pages3. MANUAL CHAIN BLOCK 1.5T - Copyengr.haseebbalochNo ratings yet
- LIFTING EQUIPMENT INSPECTION REPORTDocument4 pagesLIFTING EQUIPMENT INSPECTION REPORTRanjithNo ratings yet
- CHECKLIST - FORK LIFT UpdatedDocument4 pagesCHECKLIST - FORK LIFT UpdatedAkhilNo ratings yet
- Webbing SlingDocument2 pagesWebbing Slingengr.haseebbalochNo ratings yet
- 18 - Fork Lift Defect - OptDocument4 pages18 - Fork Lift Defect - OptMoataz NazeemNo ratings yet
- Podium Ladder 25-05-2022Document2 pagesPodium Ladder 25-05-2022dele jimohNo ratings yet
- IRM3427 Ensco Ensco5002 Installation of Padeyes Ad Load TestDocument40 pagesIRM3427 Ensco Ensco5002 Installation of Padeyes Ad Load TestAfzaalUmairNo ratings yet
- Installation of Padeyes Ad Load Test: Front CoverDocument40 pagesInstallation of Padeyes Ad Load Test: Front CoverAhmedA.HassanNo ratings yet
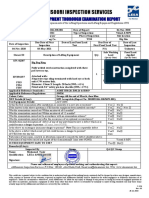
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument3 pagesAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- BOP Lifting Plate VisualDocument1 pageBOP Lifting Plate Visualyasir kunnathNo ratings yet
- 0328) CRADLE RACK 4x4-6 - SN 69 (ANEKA GAS-PTERO GAMA INDUSTRI) PDFDocument3 pages0328) CRADLE RACK 4x4-6 - SN 69 (ANEKA GAS-PTERO GAMA INDUSTRI) PDFfaisalNo ratings yet
- 410 CTDocument2 pages410 CTSARAVANAN ANo ratings yet
- 300-02 # ST 1220, Four Leg Wire Rope SlingDocument3 pages300-02 # ST 1220, Four Leg Wire Rope SlingAgeng LaksitoNo ratings yet
- BOP Plate VisualDocument1 pageBOP Plate VisualRanjithNo ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument5 pagesAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Ocean Baroness. Load Test - Teste de Carga (INCLUIR FOTO DA UNIDADE DO CLIENTE) Date - Data - Jun, 2015. Doc. N - N Do Documento - IRM4504 Rev.Document26 pagesOcean Baroness. Load Test - Teste de Carga (INCLUIR FOTO DA UNIDADE DO CLIENTE) Date - Data - Jun, 2015. Doc. N - N Do Documento - IRM4504 Rev.Gabriela MotaNo ratings yet
- Gpti Qicl 032Document2 pagesGpti Qicl 032uselessinstaid52No ratings yet
- Certificate of Examination and Test of Engine Generator: Certificate No.:DG/C1 Job No.: ASC-18N-0262Document2 pagesCertificate of Examination and Test of Engine Generator: Certificate No.:DG/C1 Job No.: ASC-18N-0262RavijNo ratings yet
- PIPELINEMAN NO.2876Document3 pagesPIPELINEMAN NO.2876Hussein HishamNo ratings yet
- 35 - 4 Leg Wire Rope Sling - TP-5456Document1 page35 - 4 Leg Wire Rope Sling - TP-5456Muhamed TarekeNo ratings yet
- Adaptor Spool (Wdrs-As-4062)Document1 pageAdaptor Spool (Wdrs-As-4062)stephanie sitompulNo ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument1 pageAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument1 pageAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Certificate of Proof Test of Lifting EquipmentDocument22 pagesCertificate of Proof Test of Lifting EquipmentnanoelbobNo ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument1 pageAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Gpti Qicl J931 Mut 019Document3 pagesGpti Qicl J931 Mut 019uselessinstaid52No ratings yet
- Man Rider Winch VisualDocument6 pagesMan Rider Winch VisualRanjithNo ratings yet
- Lift Equipment Inspection ReportsDocument3 pagesLift Equipment Inspection ReportsRanjithNo ratings yet
- International LTD: Report of Thorough ExaminationDocument1 pageInternational LTD: Report of Thorough ExaminationChisom IkengwuNo ratings yet
- C-Ingta-041-Francisco Javier Aguilar PadillaDocument2 pagesC-Ingta-041-Francisco Javier Aguilar Padillarobertorf04No ratings yet
- Lift Equipment Inspection ReportDocument1 pageLift Equipment Inspection ReportRanjithNo ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument4 pagesAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument9 pagesAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- 1 - Lock CertificateDocument5 pages1 - Lock CertificateALENo ratings yet
- 2178Document1 page2178qc_531040655No ratings yet
- Wire Rope Slings-Report UpdatedDocument2 pagesWire Rope Slings-Report UpdatedAkhilNo ratings yet
- 02 - Shackle T601-4 12 TonDocument1 page02 - Shackle T601-4 12 TonAsh Ra FNo ratings yet
- Snatch Block VisualDocument10 pagesSnatch Block VisualRanjithNo ratings yet
- 08 - Security Tower-4Document2 pages08 - Security Tower-4Muhamed TarekeNo ratings yet
- Gpti Qicl J931 Mut 041Document3 pagesGpti Qicl J931 Mut 041uselessinstaid52No ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument1 pageAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Procedure Qualification Record (PQR) Khewari Development ProjectDocument2 pagesProcedure Qualification Record (PQR) Khewari Development Projectsar sarNo ratings yet
- Gpti Qicl J931 Mut 004Document3 pagesGpti Qicl J931 Mut 004uselessinstaid52No ratings yet
- Almansoori Inspection Services: Lifting Equipment Thorough Examination ReportDocument2 pagesAlmansoori Inspection Services: Lifting Equipment Thorough Examination ReportRanjithNo ratings yet
- Adaptor Spool (Wdrs-As-4040)Document1 pageAdaptor Spool (Wdrs-As-4040)stephanie sitompulNo ratings yet
- Inspection Report: Ret-3 Enf # 54Document23 pagesInspection Report: Ret-3 Enf # 54nabi.elmansourNo ratings yet
- MAGNETIC PARTICLE INSPECTION REPORT FINDINGSDocument163 pagesMAGNETIC PARTICLE INSPECTION REPORT FINDINGSNico Achmad ZulviansyahNo ratings yet
- Astm D2321Document12 pagesAstm D2321Emre AkınayNo ratings yet
- Centro de Soporte de HPE: HP 5800/5830 Switch/6600 Router Series - BGP Configuration: BGP Configuration ExamplesDocument14 pagesCentro de Soporte de HPE: HP 5800/5830 Switch/6600 Router Series - BGP Configuration: BGP Configuration ExamplesJavierLozaLlucoNo ratings yet
- Type BSDType CSD Self Drilling ScrewsDocument2 pagesType BSDType CSD Self Drilling Screwscheow jongNo ratings yet
- NIST Water sp250 - 73 PDFDocument45 pagesNIST Water sp250 - 73 PDFSatit hunsaNo ratings yet
- VMVS2A150GP-RD70 LuminariaDocument8 pagesVMVS2A150GP-RD70 LuminariaivanNo ratings yet
- Catalog Ipaso IxDocument2 pagesCatalog Ipaso IxmathNo ratings yet
- R911379309 04 PDFDocument140 pagesR911379309 04 PDFcano720No ratings yet
- Scaling Effects in MOS DevicesDocument15 pagesScaling Effects in MOS DevicesVikram KumarNo ratings yet
- MSS SP-42-1999Document16 pagesMSS SP-42-1999Surat ButtarasriNo ratings yet
- EDI Flexair MiniPanel Spec SheetDocument2 pagesEDI Flexair MiniPanel Spec SheetKalyan Patil0% (1)
- SP SQLDocument40 pagesSP SQLd2145100% (1)
- The Ul Safety Mark: On Time Market Access To North America and BeyondDocument8 pagesThe Ul Safety Mark: On Time Market Access To North America and BeyondALI MAKRINo ratings yet
- Jericho 941 PDFDocument28 pagesJericho 941 PDFbladeliger2283% (6)
- Cellular Glass DatasheetDocument2 pagesCellular Glass DatasheetmishraenggNo ratings yet
- MK3021GAS Userguide Rev02Document11 pagesMK3021GAS Userguide Rev02nicolatesla1No ratings yet
- Net CommerceDocument560 pagesNet CommercenityavinodNo ratings yet
- Ap7173 35627Document16 pagesAp7173 35627Jose Barroso GuerraNo ratings yet
- Cubot X9 CeDocument4 pagesCubot X9 CeSaqib HussainNo ratings yet
- OMF010002 Handover-training-20031001-A-1.5Document94 pagesOMF010002 Handover-training-20031001-A-1.5Shery ChNo ratings yet
- nonVSD ElektronikonDocument60 pagesnonVSD Elektronikonchadta100% (1)
- MongoDB Quick GuideDocument61 pagesMongoDB Quick GuideDulari Bosamiya BhattNo ratings yet
- CRDI Seminar ReportDocument19 pagesCRDI Seminar ReportPrateek Gandhi100% (8)
- Iso 9001 KeyDocument13 pagesIso 9001 KeyShubhamShuklaNo ratings yet
- TwigDocument195 pagesTwigBB PrasadNo ratings yet
- Caterpillar 226B3 Skid Steer Loader Parts ManualDocument857 pagesCaterpillar 226B3 Skid Steer Loader Parts ManualГалина КарташоваNo ratings yet
- Manual BannerDocument74 pagesManual Bannercristian_ric_russoNo ratings yet
- Metsec Framing Detail sf255 PDFDocument1 pageMetsec Framing Detail sf255 PDFBanditAkosNo ratings yet
- Process and Material SpecificationDocument14 pagesProcess and Material Specificationsajithv78No ratings yet
- Safety: Important Safety Instructions What Ships in The BoxDocument4 pagesSafety: Important Safety Instructions What Ships in The BoxMarraNo ratings yet
- Sigraflex UniversalDocument6 pagesSigraflex UniversalJan SmitNo ratings yet