You might also like
- Solution Manual For Understanding Our Universe 3rd Edition by Stacy Palen Laura Kay George Blumenthal 9780Document8 pagesSolution Manual For Understanding Our Universe 3rd Edition by Stacy Palen Laura Kay George Blumenthal 9780MarieHughesebgjp100% (85)
- Solution Manual For Using Mis 7 e 7th Edition 0133546438Document14 pagesSolution Manual For Using Mis 7 e 7th Edition 0133546438MarieHughesebgjp100% (74)
- Solution Manual For Understanding Human Sexuality 14th Edition Janet Hydejohn DelamaterDocument37 pagesSolution Manual For Understanding Human Sexuality 14th Edition Janet Hydejohn DelamaterMarieHughesebgjp100% (80)
- Solution Manual For Understanding The Essentials of Critical Care Nursing 2nd Edition by PerrinDocument15 pagesSolution Manual For Understanding The Essentials of Critical Care Nursing 2nd Edition by PerrinMarieHughesebgjp100% (75)
- Solution Manual For Understanding and Managing Organizational Behavior 6 e 6th Edition 0132616173Document27 pagesSolution Manual For Understanding and Managing Organizational Behavior 6 e 6th Edition 0132616173MrsElizabethHooveryspxw100% (79)
- Solution Manual For Visual Basic 2012 How To Program 6 e 6th Edition 0133406954Document11 pagesSolution Manual For Visual Basic 2012 How To Program 6 e 6th Edition 0133406954MarieHughesebgjp100% (77)
- Solution Manual For Understanding Current Procedural Terminology and Hcpcs Coding Systems 6th Edition BowieDocument6 pagesSolution Manual For Understanding Current Procedural Terminology and Hcpcs Coding Systems 6th Edition BowieMrsElizabethHooveryspxw100% (85)
- Solution Manual For We The People 13th Edition Thomas PattersonDocument9 pagesSolution Manual For We The People 13th Edition Thomas PattersonMarieHughesebgjp100% (81)
- Solution Manual For Health Physical Assessment in Nursing 2 e 2nd Edition Donita Damico Colleen BarbaritoDocument15 pagesSolution Manual For Health Physical Assessment in Nursing 2 e 2nd Edition Donita Damico Colleen BarbaritoCristianRodriguezpawry100% (80)
- Solution Manual For VHDL For Engineers Kenneth L ShortDocument19 pagesSolution Manual For VHDL For Engineers Kenneth L ShortMarieHughesebgjp100% (87)
- Solutions Manual To Accompany Engineering Economy 6th Edition 9780073205342Document7 pagesSolutions Manual To Accompany Engineering Economy 6th Edition 9780073205342CrystalDavisntgrw100% (75)
- Solution Manual For Internet and World Wide Web How To Program 5 e 5th Edition 0132151006Document7 pagesSolution Manual For Internet and World Wide Web How To Program 5 e 5th Edition 0132151006LuisMurraymrzye100% (84)
- Solutions Manual To Accompany Principles of Corporate Finance 10th Edition 9780073530734Document9 pagesSolutions Manual To Accompany Principles of Corporate Finance 10th Edition 9780073530734BriannaJimenezojmrs99% (79)
- Solutions Manual For Stats Modeling The World 4th by Bock 0133864987Document26 pagesSolutions Manual For Stats Modeling The World 4th by Bock 0133864987RhondaCookqjdyg100% (77)
- Solutions Manual For Comprehensive Assurance Systems Tool 3e by Ingraham 0133099210Document10 pagesSolutions Manual For Comprehensive Assurance Systems Tool 3e by Ingraham 0133099210TimothyHilldpgoa100% (76)
- Test Bank For An Introduction To Policing 8th EditionDocument24 pagesTest Bank For An Introduction To Policing 8th EditionAaronBrownpnmb100% (44)
- Solution Manual For Theories of Personality 10th Edition by SchultzDocument8 pagesSolution Manual For Theories of Personality 10th Edition by SchultzMrsElizabethHooveryspxw100% (88)
- Solutions Manual To Accompany Molecular Biology of The Gene 6th Edition 9780805395921Document7 pagesSolutions Manual To Accompany Molecular Biology of The Gene 6th Edition 9780805395921BriannaJimenezojmrs100% (82)
- Solutions Manual For Business Statistics 3e by Norean D Sharpe 0133866912Document13 pagesSolutions Manual For Business Statistics 3e by Norean D Sharpe 0133866912TimothyHilldpgoa100% (75)
- Test Bank For Clinical Manifestations and Assessment of Respiratory Disease 6th Edition Des JardinsDocument3 pagesTest Bank For Clinical Manifestations and Assessment of Respiratory Disease 6th Edition Des JardinsValerieTaylorptszg100% (70)
- Solution Manual For Work Systems The Methods Measurement Management of Work Mikell P GrooverDocument12 pagesSolution Manual For Work Systems The Methods Measurement Management of Work Mikell P GrooverTimothyHilldpgoa100% (77)
- Solution Manual For Principles of Fraud Examination Wells 4th EditionDocument7 pagesSolution Manual For Principles of Fraud Examination Wells 4th EditionVeronicaBurchcekij100% (74)
- Solution Manual For Principles of Financial Accounting 11th Edition by NeedlesDocument12 pagesSolution Manual For Principles of Financial Accounting 11th Edition by NeedlesVeronicaBurchcekij100% (75)
- Solution Manual For Health Psychology 11th Edition Shelley Taylor Annette L StantonDocument11 pagesSolution Manual For Health Psychology 11th Edition Shelley Taylor Annette L StantonCristianRodriguezpawry100% (81)
- Solution Manual For Illustrated Guide To The National Electrical Code 7th Edition Charles R MillerDocument15 pagesSolution Manual For Illustrated Guide To The National Electrical Code 7th Edition Charles R MillerSamuelBrownnwoxi99% (87)
- Solution Manual For Managing Hospitality Organizations Achieving Excellence in The Guest Experience 2nd Edition Robert C Ford Michael C SturmanDocument23 pagesSolution Manual For Managing Hospitality Organizations Achieving Excellence in The Guest Experience 2nd Edition Robert C Ford Michael C SturmanAnnGregoryDDSemcxo100% (89)
- Solution Manual For Psychology Perspectives and Connections 2nd Edition by FeistDocument22 pagesSolution Manual For Psychology Perspectives and Connections 2nd Edition by FeistLauraLittleigfmz100% (84)
- Solution Manual For Introduction To Finance Markets Investments and Financial Management 14th Edition by MelicherDocument18 pagesSolution Manual For Introduction To Finance Markets Investments and Financial Management 14th Edition by MelicherLuisMurraymrzye100% (87)
- Solution Manual For Practice of Public Relations 12 e 12th Edition 0133083578Document8 pagesSolution Manual For Practice of Public Relations 12 e 12th Edition 0133083578VeronicaBurchcekij100% (79)
- Test Bank For Adult Health Nursing 6th Edition ChristensenDocument15 pagesTest Bank For Adult Health Nursing 6th Edition ChristensenValerieTaylorptszg100% (73)
- Solution Manual For Understanding Human Sexuality 14th Edition Janet Hydejohn DelamaterDocument36 pagesSolution Manual For Understanding Human Sexuality 14th Edition Janet Hydejohn DelamaterKarenHancockwksgm100% (43)
- Solutions Manual To Accompany Design and Analysis of Experiments 6th Edition 9780471487357Document6 pagesSolutions Manual To Accompany Design and Analysis of Experiments 6th Edition 9780471487357CrystalDavisntgrw100% (77)
- Solution Manual For Microeconomics Theory and Applications Browning Zupan 11th EditionDocument10 pagesSolution Manual For Microeconomics Theory and Applications Browning Zupan 11th EditionElizabethSteelefocgk100% (74)
- Solution Manual For Cognition 6 e Mark H Ashcraft Gabriel A RadvanskyDocument6 pagesSolution Manual For Cognition 6 e Mark H Ashcraft Gabriel A RadvanskyAngelKelleycfayo100% (79)
- Solution Manual For Survey of Economics Principles Applications and Tools 5th Edition by OsullivanDocument14 pagesSolution Manual For Survey of Economics Principles Applications and Tools 5th Edition by OsullivanAudreyRayqowjd100% (75)
- Solution Manual For Terrorism and Homeland Security 9th EditionDocument24 pagesSolution Manual For Terrorism and Homeland Security 9th EditionJessicaTorresxkqa100% (44)
- Solution Manual For Organic Structural Spectroscopy 2 e 2nd Edition Joseph B Lambert Scott Gronert Herbert F Shurvell David Lightner Robert Graham CooksDocument8 pagesSolution Manual For Organic Structural Spectroscopy 2 e 2nd Edition Joseph B Lambert Scott Gronert Herbert F Shurvell David Lightner Robert Graham CooksChristinaMitchellxjker99% (75)
- Solutions Manual To Accompany A First Course in Probability 8th Edition 013603313xDocument14 pagesSolutions Manual To Accompany A First Course in Probability 8th Edition 013603313xRhondaCookqjdyg100% (74)
- Solution Manual For Brief Principles of Macroeconomics 7th EditionDocument13 pagesSolution Manual For Brief Principles of Macroeconomics 7th EditionJasonRicebicrq100% (79)
- Solution Manual For The Essentials of Political Analysis 6th Edition Philip H Pollock Barry C EdwardsDocument8 pagesSolution Manual For The Essentials of Political Analysis 6th Edition Philip H Pollock Barry C EdwardsAudreyRayqowjd100% (70)
- Solutions Manual To Accompany Cost Benefit Analysis 4th Edition 0137002696Document10 pagesSolutions Manual To Accompany Cost Benefit Analysis 4th Edition 0137002696CrystalDavisntgrw100% (89)
- Solution Manual Individuals Section For Prentice Halls Federal Taxation 2013 26 e 26th Edition 0133040674Document30 pagesSolution Manual Individuals Section For Prentice Halls Federal Taxation 2013 26 e 26th Edition 0133040674TimothyHilldpgoa100% (74)
- Solution Manual For The Basic Practice of Statistics 8th Edition David S MooreDocument13 pagesSolution Manual For The Basic Practice of Statistics 8th Edition David S MooreAudreyRayqowjd100% (78)
- Solution Manual For Introduction To Javascript Programming With XML and PHP 0133068307Document3 pagesSolution Manual For Introduction To Javascript Programming With XML and PHP 0133068307RobertSchmidtfenxm100% (75)
- Solution Manual For Deviance Conformity and Social Control in Canada 4 e 4th Edition Tami M BereskaDocument9 pagesSolution Manual For Deviance Conformity and Social Control in Canada 4 e 4th Edition Tami M BereskaRandallValdezypfqw100% (75)
- Solution Manual For Managerial Economics and Organizational Architecture 5th Edition by BrickleyDocument8 pagesSolution Manual For Managerial Economics and Organizational Architecture 5th Edition by BrickleyAnnGregoryDDSemcxo100% (88)
- Solution Manual For Systems Analysis and Design 12th Edition Scott TilleyDocument13 pagesSolution Manual For Systems Analysis and Design 12th Edition Scott TilleyAudreyRayqowjd100% (79)
- Solution Manual For Macroeconomics Principles Applications and Tools 8 e 8th Edition Arthur Osullivan Steven Sheffrin Stephen PerezDocument11 pagesSolution Manual For Macroeconomics Principles Applications and Tools 8 e 8th Edition Arthur Osullivan Steven Sheffrin Stephen PerezRalphLaneifrte100% (85)
- Solution Manual For Interactive Statistics Classic Version 3rd Edition Martha AliagaDocument17 pagesSolution Manual For Interactive Statistics Classic Version 3rd Edition Martha AliagaJosephWilliamsjfyae100% (74)
- Test Bank For Adolescence 10th Edition Laurence SteinbergDocument59 pagesTest Bank For Adolescence 10th Edition Laurence SteinbergValerieTaylorptszg100% (74)
- Solution Manual For Dosage Calculations A Multi Method Approach 0132158620Document13 pagesSolution Manual For Dosage Calculations A Multi Method Approach 0132158620RandallValdezypfqw100% (86)
- Test Bank For M Finance Applications and Theory 1st Edition CornettDocument24 pagesTest Bank For M Finance Applications and Theory 1st Edition CornettStephanieRosemzdke100% (39)
- Test Bank For Auditing and Assurance Services in Australia by Grant Gay Roger Simnett 4th EditionDocument59 pagesTest Bank For Auditing and Assurance Services in Australia by Grant Gay Roger Simnett 4th EditionValerieTaylorptszg100% (72)
- Solution Manual For Managerial Decision Modeling With Spreadsheets 3rd Edition by BalakrishnanDocument4 pagesSolution Manual For Managerial Decision Modeling With Spreadsheets 3rd Edition by BalakrishnanAnnGregoryDDSemcxo100% (71)
- Discovering The Lifespan Canadian 2nd Edition Feldman Solutions ManualDocument26 pagesDiscovering The Lifespan Canadian 2nd Edition Feldman Solutions ManualSoniaLeecfab100% (56)
- Solution Manual For Mis Cases Decision Making 4th Edition by MillerDocument8 pagesSolution Manual For Mis Cases Decision Making 4th Edition by MillerElizabethSteelefocgk100% (81)
- Solution Manual For Civil Litigation 7th EditionDocument5 pagesSolution Manual For Civil Litigation 7th EditionAngelKelleycfayo100% (88)
- Solution Manual For Internal Auditing Assurance and Consulting Services 2nd Edition by RedingDocument13 pagesSolution Manual For Internal Auditing Assurance and Consulting Services 2nd Edition by RedingJosephWilliamsjfyae100% (85)
- Solution Manual For Managerial Acct2 2nd Edition by SawyersDocument28 pagesSolution Manual For Managerial Acct2 2nd Edition by SawyersAnnGregoryDDSemcxo100% (82)
- Hand Outs Oncologic Brain DsoDocument9 pagesHand Outs Oncologic Brain DsoJessa AdenigNo ratings yet
- Reflective Writing 3Document2 pagesReflective Writing 3Luiza NiyazmetovaNo ratings yet
- Incision and Drainage 2Document26 pagesIncision and Drainage 2Sandeep Kumar SenguptaNo ratings yet
- Human Anatomy Objectives WAPT 2022Document5 pagesHuman Anatomy Objectives WAPT 2022ExcelNo ratings yet
- Standardized Color-Coding Solution Labeling in The Operating RoomDocument3 pagesStandardized Color-Coding Solution Labeling in The Operating Roomcumar cabdicazizNo ratings yet
- RANZCO 2012 PosterDocument7 pagesRANZCO 2012 PosterGray Design GroupNo ratings yet
- Plastic SurgeryDocument20 pagesPlastic SurgeryGEETA MOHAN100% (1)
- Total Gastrectomy - Options For The Restoration of Gastrointestinal Continuity PDFDocument6 pagesTotal Gastrectomy - Options For The Restoration of Gastrointestinal Continuity PDFJorge SalinasNo ratings yet
- Care Client of Myomectomy.Document3 pagesCare Client of Myomectomy.joel david knda mjNo ratings yet
- Pediatric Advanced Life Support (PALS) - UpToDateDocument49 pagesPediatric Advanced Life Support (PALS) - UpToDateANGIE SIDNEY NARANJO GARCIANo ratings yet
- LASA Blood SamplingDocument4 pagesLASA Blood SamplinggursinNo ratings yet
- TKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Document6 pagesTKA Scope Arthrolysis Knee Surg Sports Traumatol Arthrosc 2010 Mar 18 (3) 346-351Fayza RihastaraNo ratings yet
- Current Concepts in Alveolar Ridge AugmentationDocument12 pagesCurrent Concepts in Alveolar Ridge AugmentationAthenaeum Scientific PublishersNo ratings yet
- Lumbar PunctureDocument6 pagesLumbar PunctureMahesh Chand100% (4)
- Admission To ICUDocument4 pagesAdmission To ICUSapiah RamanNo ratings yet
- RCOG Air Travel PregnancyDocument5 pagesRCOG Air Travel PregnancyElsaIsabelSilaenNo ratings yet
- How To Monitor Cardiovascular Function in Critical Illness in Resource-Limited SettingsDocument8 pagesHow To Monitor Cardiovascular Function in Critical Illness in Resource-Limited SettingsHendra DarmawanNo ratings yet
- 16 CONSENT FOR SURGICAL OPERATION (New)Document2 pages16 CONSENT FOR SURGICAL OPERATION (New)Aina HaravataNo ratings yet
- FORM F NewDocument2 pagesFORM F NewNilesh Ghadge50% (2)
- Ophtha Imp MCQ FmgeDocument54 pagesOphtha Imp MCQ Fmgevikas prajapatNo ratings yet
- Nursing Care of Clients On Mechanical Ventilator For BSN IV StudentsDocument52 pagesNursing Care of Clients On Mechanical Ventilator For BSN IV Studentsspanishthingz01No ratings yet
- UWORLDNCLEXreview2021 PDFDocument100 pagesUWORLDNCLEXreview2021 PDFmahshid kianiNo ratings yet
- The 2017 Inter-School First Aid Competition Guidelines: ObjectivesDocument4 pagesThe 2017 Inter-School First Aid Competition Guidelines: ObjectivesAbog Sa YutaNo ratings yet
- Revisiting The Vertebral Venous Plexus BatsonDocument15 pagesRevisiting The Vertebral Venous Plexus BatsonMorteza Mazloom Farsi BafNo ratings yet
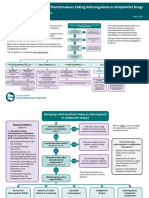
- Sdcep Anticoagulants Quick Reference Guide 2nd EditionDocument5 pagesSdcep Anticoagulants Quick Reference Guide 2nd EditionMeryem LahlouNo ratings yet
- Presurgical Orthopedics Case ReportDocument6 pagesPresurgical Orthopedics Case ReportDiana PredaNo ratings yet
- WWW Mohfw Nic In/cghs HTMLDocument7 pagesWWW Mohfw Nic In/cghs HTMLtukuNo ratings yet
- Core Topics in Congenital Cardiac SurgeryDocument148 pagesCore Topics in Congenital Cardiac SurgeryLyse lilyNo ratings yet
- May 07 Hippos InfoDocument9 pagesMay 07 Hippos InfonovitalumintusariNo ratings yet
- Sinus Node Ablation For Inappropriate Sinus Tachycardia (Mantovan)Document3 pagesSinus Node Ablation For Inappropriate Sinus Tachycardia (Mantovan)Raymond BernardusNo ratings yet
- Nail Avulsion and Chemical MatricectomyDocument4 pagesNail Avulsion and Chemical MatricectomyDavid Cáceres100% (1)