TECHNICAL DATA SHEET RELAXING MASSAGE Nº____
City and date: ___________________________________________________
PERSONAL DATA:
First and Last Name: ______________________________________________ Sex: F___ M ___
Date of Birth: ______________________________________________ Age: __________
Identification: T.I _____ C.C ____ C.E ____ Other ____ Nº_________________ From: ____________
Profession or occupation: __________________________Dirección:_________________________________
Phone: _______________ Cell. _____________________ E-mail: ___________________________
In case of emergency call: _____________________________ Relationship: _____________________ Phone (s):
_______________________
DISEASES:
Arthritis ___ Arthrosis __ Headaches __ Cancer __ Diabetes __ Dermatitis __ Scoliosis __ Fractures __ Hemophilia
__ Hepatitis __ Hyperkyphosis __ Hypertension __ Hypotension __ Herniated discs __ Where? ________________
Hyperlordosis __Metal implants __Sciatic nerve __ Osteoporosis __ Osteomyelitis __Heart problems ____ which
ones? ______________ Surgeries __ Where? ________________
Sleeping hours______ do you practice any sport: ____ have you had this type of procedure done?____ with what
results?__________________
REASON FOR THE CONSULTATION:
HYPERSENSITIVITY TO ANY COSMETIC PRODUCT:
By contact __ By inhalation __ By inhalation __ By contact __ By inhalation __ By inhalation
Oil __ Cream __Talcum __Gel __ Essence Which? _______________________________
PROCEDURE:
Relaxing massage __ General __ Localized __ Where? ________________________
Sports Massage __ General __ Localized __ Where? ________________________
Lymphatic Drainage __ General __ Localized __ Where? ________________________
REMARKS:
____________________________________________________________________________________________
____________________________________________________________________________________________
____________________________________________________________________
INFORMED CONSENT:
I__________________ identified (a) with citizenship card N°______________________ authorize the trainee
______________________ to perform the following procedure____________ and I release her from any liability that may
arise due to my own skin and outside the procedure itself I certify that I have read, I have been explained and I have
understood that the procedure has no processes, whose outcome depends on my care. My signature certifies that I agree with
the above.
____________________________ _____________________________
Signature of patient Signature of Esthetician
APPOINTMENT CONTROL
DATE PROCEDURE ESTHETICIAN SIGNATURE
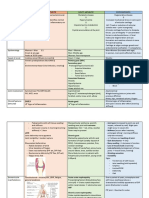
INDICATIONS CONTRAINDICATIONS
Disorders of the locomotor system: leg heaviness, Feverish states or processes that run with fever.
swelling or overloading sensation, muscle discomfort... Severe hemorrhagic alterations.
Nervous system disorders, stress, exhaustion, insomnia, Phlebitis, thrombophlebitis and lymphagitis.
nervousness, chiromassage acts as a powerful relaxation Unconsolidated bone fractures.
tool. Decompensated heart disease (collect as m
information as possible from the patient and abov
Circulatory system disorders: deficiencies in venous and the corresponding medical diagnosis; if there is
lymphatic return circulation,(TMDL), swelling of the legs, doubt, we will not act).
overloading ..... Rheumatism in its acute phase.
Disorders of the digestive system, with massage Tumor conditions and cancer.
techniques can help to a better functioning. Infectious skin diseases.
Acute trauma.
At the skin level, it improves its appearance and structure, Muscle ruptures (fibers) and tendon rupt
stimulates circulation and promotes tissue oxygenation. (disinsertions) in their acute phase.
Burns.
Calcifications of soft structures.
CONCEPTS
Muscle spasms : disarrangement of the muscle fibers losing their elongation or movements and they become disarranged. Caused by: over fatigue, repetitive
movements, exaggerated and prolonged loads or sudden unexpected news of heavy loads, e.g.: 3 hours of exercise and did not take the muscle to its maximum
stretch: 3 hours of exercise and I did not take the muscle to its maximum stretch and it becomes saturated and accumulates toxic substances and lactic or
pyruvic acid is generated as these substances have become toxins, Lack of oxygenation in the muscle or by loss of fluids (mineral salts) producing nerve
irritation.
CONTRACTURE: rupture of some muscle fibers and they are encapsulated and generated by strong movements or fibromyalgia in this case the muscle does
not heal, there is no way to rearrange.
TEAR: Rupture of the muscle belly is broken and there is an internal bleeding and there is nothing that can join it again is wrapped in a layer called muscular
facet and loses mobility and leads to contracture if it is muscular there is not so much problem but if it is tendon only recovers in 10%.
You might also like
- Ata 51 Airbus TrainingDocument710 pagesAta 51 Airbus TrainingKliment Voroshilov100% (1)
- Cell Riddles Answer KeyDocument1 pageCell Riddles Answer KeyJonNelson GarciaNo ratings yet
- Chapter 9 - Soft Tissue Damage and HealingDocument28 pagesChapter 9 - Soft Tissue Damage and HealingdafortminorNo ratings yet
- Case Study - The Case of The Painful Hands - SPR 2021Document5 pagesCase Study - The Case of The Painful Hands - SPR 2021Nicholas LeeNo ratings yet
- Case Study - The Case of The Painful Hands - SPR 2021Document5 pagesCase Study - The Case of The Painful Hands - SPR 2021Nicholas LeeNo ratings yet
- Soft Tissue Damage and HealingDocument6 pagesSoft Tissue Damage and HealingPamela CoralNo ratings yet
- Rheumatoid ArthritisDocument11 pagesRheumatoid Arthritisicecreamcone_201No ratings yet
- Effect of Injury and Immobilization On MuscleDocument19 pagesEffect of Injury and Immobilization On Musclesonali tushamerNo ratings yet
- Soft Tissue PrinciplesDocument41 pagesSoft Tissue PrinciplesZgama AbdulrahmanNo ratings yet
- Lower Leg Pain Differential Diagnosis - OtherDocument13 pagesLower Leg Pain Differential Diagnosis - Otherapi-619359087No ratings yet
- Presentation (MUSCULOSKELETAL AND CONNECTIVE TISSUESDocument37 pagesPresentation (MUSCULOSKELETAL AND CONNECTIVE TISSUESDaniellaNo ratings yet
- Skin PhysiologyDocument6 pagesSkin PhysiologyLicia GabrielleNo ratings yet
- Joint Pain One PagerDocument3 pagesJoint Pain One PagermustafaNo ratings yet
- Soft Tissue LesionsDocument33 pagesSoft Tissue Lesionsnimra khaliqNo ratings yet
- DermatomyositisDocument2 pagesDermatomyositisFarrukh MuzaffarNo ratings yet
- MJM ClinicalDocument14 pagesMJM Clinicalarjun.k5796No ratings yet
- Chapter 5 Tissue Healing and Wound CareDocument17 pagesChapter 5 Tissue Healing and Wound CareDrKrishna DasNo ratings yet
- Fascia Flowe Checklist 2394Document18 pagesFascia Flowe Checklist 2394agus berteNo ratings yet
- Oh Yeah Anatomy BBDocument3 pagesOh Yeah Anatomy BBJason ChenNo ratings yet
- Fractures and Principles in Management (Thari Raman - S Conflicted Copy 2016-05-07Document59 pagesFractures and Principles in Management (Thari Raman - S Conflicted Copy 2016-05-07Suganeya UdiasoorianNo ratings yet
- DR Bachrach Explains Prolo, ThoroughlyDocument14 pagesDR Bachrach Explains Prolo, Thoroughlycindy.laverty5406No ratings yet
- Notes On AmputationsDocument3 pagesNotes On AmputationsShaileeNo ratings yet
- Fracture RehabilitationDocument43 pagesFracture Rehabilitationnanahossam12345No ratings yet
- Osteoarthritis AapmrDocument5 pagesOsteoarthritis AapmrBiandaNo ratings yet
- Carpal Tunnel SyndromeDocument15 pagesCarpal Tunnel SyndromeDavin Caturputra SetiamanahNo ratings yet
- Osteoarthritis (Oa) : Prakash Thakulla InternDocument48 pagesOsteoarthritis (Oa) : Prakash Thakulla InternPrakash ThakullaNo ratings yet
- Rheumatoid ArthritisDocument30 pagesRheumatoid ArthritisMelisaNo ratings yet
- Paramedic Soft Tissue InjuryDocument60 pagesParamedic Soft Tissue InjuryPaulhotvw67100% (5)
- Acute Therapeutic ExerciseDocument32 pagesAcute Therapeutic ExerciseDuncan D'AmicoNo ratings yet
- Chapter Four HealingDocument70 pagesChapter Four HealingAhmed AzeezNo ratings yet
- Shoulder Conditions in Agility Dogs: T T T TDocument5 pagesShoulder Conditions in Agility Dogs: T T T TJuan-PabloChaperoArenasNo ratings yet
- Fix Presentasi IntegumenDocument31 pagesFix Presentasi IntegumenElla SaliiNo ratings yet
- Day 7 - KIN 4200 - 2024 - Corrective Exercise - Inhibition and LengtheningDocument25 pagesDay 7 - KIN 4200 - 2024 - Corrective Exercise - Inhibition and Lengtheningavocado 677No ratings yet
- Bio 2Document3 pagesBio 2jmNo ratings yet
- Unit 2 - Physiological Reaction To InjuryDocument90 pagesUnit 2 - Physiological Reaction To InjuryFabian Chapima100% (1)
- Musculoskeletal Disorders FRACTURESDocument10 pagesMusculoskeletal Disorders FRACTURESرافت العواضيNo ratings yet
- Surgery - Principle of Wound Healing and ManagementDocument39 pagesSurgery - Principle of Wound Healing and Managementjue_mardhiahNo ratings yet
- PEH Causes of Sports InjuriesDocument7 pagesPEH Causes of Sports InjuriesFaye TiuNo ratings yet
- Pe MT ReviewerDocument2 pagesPe MT ReviewerPhiloNo ratings yet
- Muscle Strain Injuries: Tero A.H. Järvinen, Minna Kääriäinen, Markku Järvinen,,, and Hannu KalimoDocument7 pagesMuscle Strain Injuries: Tero A.H. Järvinen, Minna Kääriäinen, Markku Järvinen,,, and Hannu Kalimonnick0No ratings yet
- Healing RepairDocument39 pagesHealing RepairRakeesh VeeraNo ratings yet
- Fracture PresentationDocument58 pagesFracture Presentationshejila c hNo ratings yet
- Tissue RepairDocument45 pagesTissue RepairTewodros Teshome100% (1)
- 2 NCM114Document24 pages2 NCM114Adrian SantiagoNo ratings yet
- Chapter 4-Task2Document8 pagesChapter 4-Task2CHRISTIAN CALAMBANo ratings yet
- Muscular SystemDocument23 pagesMuscular SystemHarol CaballeroNo ratings yet
- Bone Fracture Grp3Document12 pagesBone Fracture Grp3Marjian BaruaNo ratings yet
- ErgoDocument2 pagesErgoNajwa AthirahNo ratings yet
- IASTM Assam Workshop ManualDocument67 pagesIASTM Assam Workshop ManualNicola100% (1)
- 2 Bone Joint and Muscle Disorders of DogsDocument15 pages2 Bone Joint and Muscle Disorders of DogsKoleen Lopez ÜNo ratings yet
- Earth and Life ScienceDocument13 pagesEarth and Life ScienceShareah Faith BalanguiNo ratings yet
- WK 2 NFK 202Document88 pagesWK 2 NFK 202JSeasharkNo ratings yet
- Osteoarthritis Dan RA FKIKDocument89 pagesOsteoarthritis Dan RA FKIKVaniaNo ratings yet
- Ms 1 Lec Integumentary Disorders 1Document35 pagesMs 1 Lec Integumentary Disorders 1Denise LacapNo ratings yet
- Bones and Joints: Bone Is A Specialised Connective Tissue Which HasDocument34 pagesBones and Joints: Bone Is A Specialised Connective Tissue Which HasvaishnaviNo ratings yet
- Musculoskeletal DisordersDocument8 pagesMusculoskeletal DisordersShaina Joy SaballoNo ratings yet
- Complications of FracturesDocument29 pagesComplications of FracturesAlina Panciuc100% (1)
- Case 1 Revision 1Document4 pagesCase 1 Revision 1Peter McManusNo ratings yet
- Orthopedic RheumatologyDocument9 pagesOrthopedic RheumatologyAngelinaNo ratings yet
- Principles of Fractures: (Continued)Document44 pagesPrinciples of Fractures: (Continued)Abdi Ñãśìr Møhàmèď ŚàĺàhNo ratings yet
- Gout Presence of Symptoms Affecting The Whole Body (Systemic)Document5 pagesGout Presence of Symptoms Affecting The Whole Body (Systemic)Swastika Sekar AstriNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Rpas Exam Syllabus SOLVED - WordDocument9 pagesRpas Exam Syllabus SOLVED - WordScribdTranslationsNo ratings yet
- Case Study - Solution - Alternative FinancingDocument6 pagesCase Study - Solution - Alternative FinancingScribdTranslationsNo ratings yet
- Concept Map T8.2Document2 pagesConcept Map T8.2ScribdTranslationsNo ratings yet
- DD124 Exam 2Document7 pagesDD124 Exam 2ScribdTranslationsNo ratings yet
- Aa Preventive Maintenance Report - ItpDocument32 pagesAa Preventive Maintenance Report - ItpScribdTranslationsNo ratings yet
- Case 4 ASICS QuestionsDocument1 pageCase 4 ASICS QuestionsScribdTranslationsNo ratings yet
- Colun Market ResearchDocument9 pagesColun Market ResearchScribdTranslationsNo ratings yet
- PC3 Simulation Tools For Decision MakingDocument9 pagesPC3 Simulation Tools For Decision MakingScribdTranslationsNo ratings yet
- Network Layers ExplanationDocument3 pagesNetwork Layers ExplanationScribdTranslationsNo ratings yet
- Session My Name Is Special and UniqueDocument2 pagesSession My Name Is Special and UniqueScribdTranslationsNo ratings yet
- EXCEL PracticeDocument10 pagesEXCEL PracticeScribdTranslationsNo ratings yet
- Final Exam - Financial Administration - Group N°11Document9 pagesFinal Exam - Financial Administration - Group N°11ScribdTranslationsNo ratings yet
- Final Work - Applied Statistics For Business.Document28 pagesFinal Work - Applied Statistics For Business.ScribdTranslationsNo ratings yet
- M2 - TI - Skills For Oral and Written Communication PDFDocument5 pagesM2 - TI - Skills For Oral and Written Communication PDFScribdTranslationsNo ratings yet
- Bank Questions PC Virtual Unit 2Document13 pagesBank Questions PC Virtual Unit 2ScribdTranslationsNo ratings yet
- Response To Demand Rendering of Accounts.Document9 pagesResponse To Demand Rendering of Accounts.ScribdTranslationsNo ratings yet
- Risk Matrix Going On African Photo SafariDocument15 pagesRisk Matrix Going On African Photo SafariScribdTranslationsNo ratings yet
- Furuno FMD ECDIS PDFDocument14 pagesFuruno FMD ECDIS PDFScribdTranslations100% (1)
- Workshop 13 Situations Requirements HSEQDocument14 pagesWorkshop 13 Situations Requirements HSEQScribdTranslationsNo ratings yet
- Coca Cola Performance EvaluationDocument1 pageCoca Cola Performance EvaluationScribdTranslationsNo ratings yet
- Final Questionnaire Module 1 CNDH Prevention of TortureDocument5 pagesFinal Questionnaire Module 1 CNDH Prevention of TortureScribdTranslationsNo ratings yet
- Administration Financière t2 UPNDocument10 pagesAdministration Financière t2 UPNScribdTranslationsNo ratings yet
- TaskDocument2 pagesTaskScribdTranslationsNo ratings yet
- Exercises and ProblemsDocument65 pagesExercises and ProblemsScribdTranslationsNo ratings yet
- Final Work Caixabank CaseDocument7 pagesFinal Work Caixabank CaseScribdTranslationsNo ratings yet
- Legal Analysis of George OrwellsDocument10 pagesLegal Analysis of George OrwellsScribdTranslationsNo ratings yet
- Life Center - Worthy Are You - Forever PDFDocument1 pageLife Center - Worthy Are You - Forever PDFScribdTranslationsNo ratings yet
- Solved T-Student Distribution ExercisesDocument4 pagesSolved T-Student Distribution ExercisesScribdTranslationsNo ratings yet
- SEQUENCE The Process of Construction of The Argentine National State (1853-1880) - 6th MODIFIEDDocument13 pagesSEQUENCE The Process of Construction of The Argentine National State (1853-1880) - 6th MODIFIEDScribdTranslationsNo ratings yet
- Final Questionnaire Module 2 CNDH Prevention of TortureDocument7 pagesFinal Questionnaire Module 2 CNDH Prevention of TortureScribdTranslationsNo ratings yet
- Chemlast 0-RingsDocument2 pagesChemlast 0-RingsPeter PondianNo ratings yet
- DI - Millennials and BeyondDocument10 pagesDI - Millennials and BeyondNagaraj NavalgundNo ratings yet
- NEET For PlanDocument1 pageNEET For PlanshivendrakumarNo ratings yet
- Activity 1 BarreraDocument40 pagesActivity 1 BarreraCess RiveroNo ratings yet
- Notes (Synthetic Fibres and Plastics) PDFDocument7 pagesNotes (Synthetic Fibres and Plastics) PDFSonia100% (2)
- CLARIFYING YOUR VALUES (Adapted From Tobias Lundgren's Bull's Eye Worksheet)Document2 pagesCLARIFYING YOUR VALUES (Adapted From Tobias Lundgren's Bull's Eye Worksheet)Lan HoàngNo ratings yet
- EatonDocument157 pagesEatonMauro MonsalveNo ratings yet
- Jaw Crusher Model 2650 Spec Sheet: Base LubricationDocument2 pagesJaw Crusher Model 2650 Spec Sheet: Base LubricationDilnesa EjiguNo ratings yet
- 26ft Springer Cruiser Stern Narrowboat For SaleDocument2 pages26ft Springer Cruiser Stern Narrowboat For SaleDominic MilesNo ratings yet
- Sensitive Periods: Sensitivity To OrderDocument3 pagesSensitive Periods: Sensitivity To OrderSindhuNo ratings yet
- J ctv18gfz7c 21Document13 pagesJ ctv18gfz7c 21BOUAKKAZ NAOUALNo ratings yet
- Motor Es CatDocument42 pagesMotor Es CatfelixezamoraNo ratings yet
- Cleaning-Instructions-Fi-5750c Scanner PDFDocument2 pagesCleaning-Instructions-Fi-5750c Scanner PDFlftrevNo ratings yet
- Submersible Cable Joints 3M Scotchcast 82F1 82F2 82BF1Document4 pagesSubmersible Cable Joints 3M Scotchcast 82F1 82F2 82BF1Ernest9No ratings yet
- Cadbury Dairy Milk's Advertising Campaigns in IndiaDocument35 pagesCadbury Dairy Milk's Advertising Campaigns in IndiaRohit GomesNo ratings yet
- Control Self Assessment (CSA) : JUNI 2020Document18 pagesControl Self Assessment (CSA) : JUNI 2020Frissca PrawithaNo ratings yet
- How To Use Vernier Caliper - MicrometerDocument35 pagesHow To Use Vernier Caliper - MicrometerJuan Manuel Ortega PérezNo ratings yet
- OHAS Final Quiz 1 - Attempt ReviewDocument6 pagesOHAS Final Quiz 1 - Attempt ReviewNot Racist By The Way100% (1)
- AL Chemistry 1995-1998 Paper 1Document18 pagesAL Chemistry 1995-1998 Paper 1api-3734333No ratings yet
- FM200Document20 pagesFM200Matthew BennettNo ratings yet
- Sol-Gel Processing Is One of The Routes For The Preparation of Porous Materials by Their Solidification From A True Solution PhaseDocument6 pagesSol-Gel Processing Is One of The Routes For The Preparation of Porous Materials by Their Solidification From A True Solution Phaseancastami100% (1)
- Fire Safety in The Home - JGDocument2 pagesFire Safety in The Home - JGJamieGillumNo ratings yet
- Refresher Day 1Document6 pagesRefresher Day 1Jevan A. CalaqueNo ratings yet
- How To Use Whirlpool Microwave Oven Magicook 20gDocument4 pagesHow To Use Whirlpool Microwave Oven Magicook 20gShreyas1690No ratings yet
- Water: Carah Fe Bacus, RNDocument24 pagesWater: Carah Fe Bacus, RNcoosa liquorsNo ratings yet
- DR Dance Dosi Me Tryin Digital MammographyDocument54 pagesDR Dance Dosi Me Tryin Digital MammographyAnonymous 2gLSPeNo ratings yet
- Laporan Pendahuluan Demensia - Id.enDocument11 pagesLaporan Pendahuluan Demensia - Id.enRaudatul jannahNo ratings yet
- Echoupal S PresentationDocument24 pagesEchoupal S PresentationPrabhat KumarNo ratings yet