You might also like
- Pillar Stone Case StudyDocument3 pagesPillar Stone Case StudyAlexandra IthalNo ratings yet
- H22-6 - Manual - S223.472.00 enDocument176 pagesH22-6 - Manual - S223.472.00 enLmf Daniel100% (4)
- Asm 652 Organanization AnalysisDocument8 pagesAsm 652 Organanization AnalysisSITINo ratings yet
- Construction Safety Inspection Checklist PDFDocument4 pagesConstruction Safety Inspection Checklist PDFBrazilemio RoswithaNo ratings yet
- Oktec Manual PDFDocument64 pagesOktec Manual PDFpurnomoNo ratings yet
- Projects Transmission Department HSE Inspection Report: # 3091800062 & 63 132/11kV Makhazen S/SDocument6 pagesProjects Transmission Department HSE Inspection Report: # 3091800062 & 63 132/11kV Makhazen S/SAnonymous kWfNFbNo ratings yet
- Sterile Touch - UVC Handrail Sterilization Installation InstructionsDocument12 pagesSterile Touch - UVC Handrail Sterilization Installation InstructionsGA ESNo ratings yet
- Axminster AC125BDS SanderDocument20 pagesAxminster AC125BDS Sanderj_abendstern4688No ratings yet
- HSE-F-NEOM-004 - Safety Induction FormDocument1 pageHSE-F-NEOM-004 - Safety Induction FormAhmed Mohamed100% (1)
- EN - 10 Life Saving Rules A4Document10 pagesEN - 10 Life Saving Rules A4k03055638No ratings yet
- PPE Stock ReportDocument1 pagePPE Stock ReportAPEX STRUCTURENo ratings yet
- Grinding Machine ChecklistDocument1 pageGrinding Machine ChecklistBiswaranjan SahooNo ratings yet
- Proforma-I (Counter Check & Check List of Safety Measures)Document1 pageProforma-I (Counter Check & Check List of Safety Measures)sdo jatliNo ratings yet
- Job Sheet - 3-ArcDocument3 pagesJob Sheet - 3-ArcSamerNo ratings yet
- L021 - OHSE Piling Work Permit Cum Checklist FormatDocument1 pageL021 - OHSE Piling Work Permit Cum Checklist FormatRajib MondalNo ratings yet
- Abbreviations Used in This Manual: 5. Ecu (Electronic Control Unit)Document130 pagesAbbreviations Used in This Manual: 5. Ecu (Electronic Control Unit)jhoan maestreNo ratings yet
- Single Man Cradle - Technical DataDocument5 pagesSingle Man Cradle - Technical DataFrancis BautistaNo ratings yet
- Work Method and Risk Mitigation: Brief Description: ReasonDocument2 pagesWork Method and Risk Mitigation: Brief Description: ReasonrajeevNo ratings yet
- Ceklis FBHDocument1 pageCeklis FBHandi warsitoNo ratings yet
- Safe Execution of Job ERECTIONDocument5 pagesSafe Execution of Job ERECTIONHari NairNo ratings yet
- Debit MemoDocument1 pageDebit MemoBijin BalakrishnanNo ratings yet
- Jsa Manual Excavation To Install New Fire Water Line & Fire Hydrant For New Ome Building 0000Document12 pagesJsa Manual Excavation To Install New Fire Water Line & Fire Hydrant For New Ome Building 0000thennarasuNo ratings yet
- Indermediate Shaft Bearing Svenska BearingDocument17 pagesIndermediate Shaft Bearing Svenska BearingImmorthalNo ratings yet
- Welding CheckDocument1 pageWelding CheckAgnesha A KempkesNo ratings yet
- Ohs - PR-09-14-F04 (A) Personal Protective Equipment IssueDocument1 pageOhs - PR-09-14-F04 (A) Personal Protective Equipment IssueShadeed MohammedNo ratings yet
- How Will The 5900 Meet My Needs?: Application-Based Testing SolutionsDocument1 pageHow Will The 5900 Meet My Needs?: Application-Based Testing SolutionsAnkit ChaurasiaNo ratings yet
- JSA-Fabrication, AssemblyDocument19 pagesJSA-Fabrication, AssemblyAshfaq Husain AnsariNo ratings yet
- Jobs Safety Plan - TemplateDocument16 pagesJobs Safety Plan - TemplateFairus Md Yusof100% (1)
- OCP - 21 - Safe Use of HelmetDocument2 pagesOCP - 21 - Safe Use of HelmetNagendra Kumar SinghNo ratings yet
- Ai Ek1-221 EngDocument27 pagesAi Ek1-221 EngRadek BabuszkiewiczNo ratings yet
- 615-Hydraulic Pipe Changing of SCR#3Document5 pages615-Hydraulic Pipe Changing of SCR#3Buddy HartNo ratings yet
- Confined Space PermitDocument3 pagesConfined Space PermitDhaneswar SwainNo ratings yet
- Work Procedure Handrails and HandrailsDocument14 pagesWork Procedure Handrails and HandrailsScribdTranslationsNo ratings yet
- MS For Public Address System InstallationDocument9 pagesMS For Public Address System Installationanver.yusifNo ratings yet
- All ChecklistDocument31 pagesAll Checklistsunil KumarSwainNo ratings yet
- (A Govt. of India Enterprise) NTPC Gadarwara 2 800 MW STPP: Safety Checklist For Welding Safety ChecklistDocument1 page(A Govt. of India Enterprise) NTPC Gadarwara 2 800 MW STPP: Safety Checklist For Welding Safety ChecklistDheeraj KumarNo ratings yet
- Supplemental Inflatable Restraints (Sir)Document7 pagesSupplemental Inflatable Restraints (Sir)David Wise-MannNo ratings yet
- 10 - WMS - Turpentine - Tie BeamDocument6 pages10 - WMS - Turpentine - Tie BeamVikramaditya NayakNo ratings yet
- Checklist For Cutting MachineDocument1 pageChecklist For Cutting Machinepritamkd201No ratings yet
- M/S Ankit Metals Doc. No.: Sapety Items StandardDocument1 pageM/S Ankit Metals Doc. No.: Sapety Items StandardPratap MalikNo ratings yet
- SWMS05 - Manual HandlingDocument15 pagesSWMS05 - Manual HandlingmaryNo ratings yet
- EHS Statistics ReportDocument2 pagesEHS Statistics ReportAPEX STRUCTURENo ratings yet
- Motorized Welding Machine Monthly ChecklistDocument2 pagesMotorized Welding Machine Monthly ChecklistDAOUMY YOUNESSNo ratings yet
- Vepl 2Document15 pagesVepl 2Manas Ranjan NayakNo ratings yet
- Checklist For Electric Arc Welding and CuttingDocument1 pageChecklist For Electric Arc Welding and CuttingsafarazalijanNo ratings yet
- Contractor Job Safety PlanDocument15 pagesContractor Job Safety PlanAnonymous ocCa18RNo ratings yet
- ERECTION, MODIFICATION & DISMANTLING OF SCAFFOLDING WORKS - Risk Assessment - REV01Document10 pagesERECTION, MODIFICATION & DISMANTLING OF SCAFFOLDING WORKS - Risk Assessment - REV01SolimanNo ratings yet
- Smu014269 AtsDocument6 pagesSmu014269 Atsadelaida cohen cantilloNo ratings yet
- Contractor Job Safety Inspection Checklist For 06.02.2021 (For ANWAR)Document5 pagesContractor Job Safety Inspection Checklist For 06.02.2021 (For ANWAR)Mohammad Anwar HossainNo ratings yet
- Annexure 2 SafetyDocument8 pagesAnnexure 2 SafetyArjun SenNo ratings yet
- Installation of Copper Pipes and Fittings.: Barq Group Risk AssessmentDocument8 pagesInstallation of Copper Pipes and Fittings.: Barq Group Risk AssessmentYousaf Richu67% (3)
- Pre-Start Checklist For Hydraulic (Mobile) Crane: Form: HDEC-HSE-CE-005 (E)Document3 pagesPre-Start Checklist For Hydraulic (Mobile) Crane: Form: HDEC-HSE-CE-005 (E)Nurma Rifah100% (4)
- JSA - ELLECTRICAL AINDAR LAYING TERMINATION - CompressedDocument8 pagesJSA - ELLECTRICAL AINDAR LAYING TERMINATION - Compressedmalikshoaib8528No ratings yet
- HR 01 TNI AssociatesDocument1 pageHR 01 TNI AssociatesDeepakNo ratings yet
- PBSSFTJSA005-Work at HighDocument4 pagesPBSSFTJSA005-Work at HighHSE Pakubumi SemestaNo ratings yet
- HSE Equipment QuotationDocument1 pageHSE Equipment QuotationAhmed NasserNo ratings yet
- Hitac SpecsDocument14 pagesHitac SpecsIan FancubitNo ratings yet
- Ppe Tool Box Talk 01Document4 pagesPpe Tool Box Talk 01arunNo ratings yet
- Project Work InstructionDocument5 pagesProject Work InstructionRAJU RAJPUTNo ratings yet
- PPE Inspection Report-AuditDocument1 pagePPE Inspection Report-AuditR Sahadeo ReddyNo ratings yet
- Work Permit Format - Jul 2014Document2 pagesWork Permit Format - Jul 2014NilamSanjeev Kumar SinghNo ratings yet
- Breakaways enDocument20 pagesBreakaways enAcid HadiNo ratings yet
- Roofing Fact Sheet-2 Column Format052820final PDFDocument6 pagesRoofing Fact Sheet-2 Column Format052820final PDFDiego Quiroga CruzNo ratings yet
- Modular Shared HomeDocument45 pagesModular Shared Homejames makauNo ratings yet
- 05 Detailing Zinc and Sheet Metal CladdingDocument15 pages05 Detailing Zinc and Sheet Metal CladdingvaleriialukianNo ratings yet
- Ua Uc DLCL 06 03 2024Document6 pagesUa Uc DLCL 06 03 2024Anvarsha SharafudheenNo ratings yet
- SATIP-Q-006-02 Rev 8 Conventional & Sulfur Extended Asphalt Paving FinalDocument3 pagesSATIP-Q-006-02 Rev 8 Conventional & Sulfur Extended Asphalt Paving FinalSehna SerajNo ratings yet
- Rem Koolhaas: Architect By: Adam Brillhart, John Anthal, Sean Obrian, Kenny ModrowDocument17 pagesRem Koolhaas: Architect By: Adam Brillhart, John Anthal, Sean Obrian, Kenny ModrowSebastiano PorcuNo ratings yet
- Internship Report 17l-4621 2020Document33 pagesInternship Report 17l-4621 2020Mirza TalhaNo ratings yet
- 6 Ead 88Document52 pages6 Ead 88Muhamad AlHajjiNo ratings yet
- Elkomix-60 Quickmaster With Conveyor - StojanovicDocument5 pagesElkomix-60 Quickmaster With Conveyor - StojanovicBorivoje StojanovicNo ratings yet
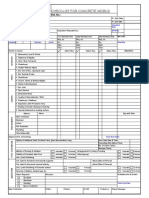
- Checklist For Concrete Works: Name of Work: Employer: Contract No.: ContractorDocument1 pageChecklist For Concrete Works: Name of Work: Employer: Contract No.: Contractormallikarjuna ketheNo ratings yet
- 1.14.6C003 Material Submission of Precast Concrete Pipe For Drainage WorksDocument1 page1.14.6C003 Material Submission of Precast Concrete Pipe For Drainage WorksCheongNo ratings yet
- Bid Notice Abstract: Invitation To Bid (ITB)Document3 pagesBid Notice Abstract: Invitation To Bid (ITB)John Rheynor MayoNo ratings yet
- Fine Woodworking - April 2020Document88 pagesFine Woodworking - April 2020Paulina Barszez100% (1)
- D Eugp1 TPT G 000 Gen FWG 001 R01Document1 pageD Eugp1 TPT G 000 Gen FWG 001 R01debapriyoNo ratings yet
- Drafting Aijunful TabayDocument4 pagesDrafting Aijunful TabayAijunful TabayNo ratings yet
- ARaymondTinnerman 2016 Catalog 34Document2 pagesARaymondTinnerman 2016 Catalog 34Gustavo HofstatterNo ratings yet
- Bansal Roofing ProductsDocument15 pagesBansal Roofing ProductsChirag SharmaNo ratings yet
- CMDF-AMO SPECS Presentation 2016Document47 pagesCMDF-AMO SPECS Presentation 2016Cherry DuldulaoNo ratings yet
- KP Jasim UsmanDocument7 pagesKP Jasim UsmanbobbyNo ratings yet
- Pink ToiletDocument3 pagesPink ToiletDanysh ShafeeNo ratings yet
- Basf Masterflow 700 TdsDocument2 pagesBasf Masterflow 700 Tdsalan2191100% (1)
- Partnership Deed Format in English (Construction)Document3 pagesPartnership Deed Format in English (Construction)Princess FarahNo ratings yet
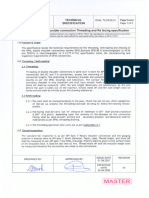
- DP2S Rethreading Technical SpecificationDocument2 pagesDP2S Rethreading Technical SpecificationRodrigoNo ratings yet
- Scope of Works: TOTAL AMOUNT .Document2 pagesScope of Works: TOTAL AMOUNT .alvin bautistaNo ratings yet
- WORK RELATED TO PREPARATION of BILL OF QUANTITY & TENDER DOCUMENTDocument31 pagesWORK RELATED TO PREPARATION of BILL OF QUANTITY & TENDER DOCUMENTUtkarsh GautamNo ratings yet
- 02-02 Building Systems DesignDocument11 pages02-02 Building Systems DesignKimmae Academic ServiceNo ratings yet
- Construction Engineer Learning Development GuideDocument45 pagesConstruction Engineer Learning Development Guidescott karamoy24No ratings yet