You might also like
- Helping Kids of Parents with Trauma or Mental IllnessDocument56 pagesHelping Kids of Parents with Trauma or Mental Illnesscalista3lucille100% (1)
- Axiatonal Lines Connection IntroductionDocument9 pagesAxiatonal Lines Connection IntroductionDavid Lopes100% (1)
- Quantum ComputingDocument2 pagesQuantum Computingakshit100% (3)
- Conduct Disorder: Dr. Jayanta Kurmi Junior Resident Dept of Psychiatry SMCHDocument50 pagesConduct Disorder: Dr. Jayanta Kurmi Junior Resident Dept of Psychiatry SMCHJayanta Kurmi100% (1)
- GOLDEN DAWN 3 8 Highlights of The Fourth Knowledge LectureDocument7 pagesGOLDEN DAWN 3 8 Highlights of The Fourth Knowledge LectureF_RCNo ratings yet
- Negative Childhood Experiences and Mental Health: Theoretical, Clinical and Primary Prevention ImplicationsDocument4 pagesNegative Childhood Experiences and Mental Health: Theoretical, Clinical and Primary Prevention ImplicationsSri EndriyaniNo ratings yet
- 2012 HCO Oriented Core ProceduresDocument30 pages2012 HCO Oriented Core ProceduresPancho Perez100% (1)
- Growing Up With a Psychotic MotherDocument13 pagesGrowing Up With a Psychotic MotherdrguillermomedinaNo ratings yet
- Final Research ProposalDocument14 pagesFinal Research Proposalapi-309943573100% (1)
- Crossing The Great Divide: Coproduction, Synergy, and DevelopmentDocument15 pagesCrossing The Great Divide: Coproduction, Synergy, and Development3113TNo ratings yet
- How Psychological Health Affects Your Physical Health: Toxic People Are No Good For YouFrom EverandHow Psychological Health Affects Your Physical Health: Toxic People Are No Good For YouNo ratings yet
- Understanding Depression Among StudentsDocument13 pagesUnderstanding Depression Among StudentsAriel Nube75% (72)
- Error Correction ModelDocument37 pagesError Correction ModelRollins JohnNo ratings yet
- Research Methods - Final Research ProposalDocument10 pagesResearch Methods - Final Research Proposalapi-583124304No ratings yet
- Mental DisabilitiesDocument11 pagesMental DisabilitiesKaren IrasemaNo ratings yet
- Final Research PaperDocument11 pagesFinal Research Paperapi-313003825No ratings yet
- 2012 AdolescentattitudesDocument7 pages2012 AdolescentattitudesMadawi AlotaibiNo ratings yet
- Psychiatric Services for Emotional Problems in Mental RetardationDocument11 pagesPsychiatric Services for Emotional Problems in Mental RetardationBIANA-MARIA MACOVEINo ratings yet
- Parent and Child Knowledge and Attitudes Toward Mental Illness: A Pilot StudyDocument11 pagesParent and Child Knowledge and Attitudes Toward Mental Illness: A Pilot StudySteluta AureliaNo ratings yet
- What's Driving The Rise in Teen Depression?: Examining The Contributing Factors That Have Led To The IncreaseDocument6 pagesWhat's Driving The Rise in Teen Depression?: Examining The Contributing Factors That Have Led To The IncreaseNurnajihahNo ratings yet
- Psychosocial Development Among Adolescents With Visual ImpairmentDocument6 pagesPsychosocial Development Among Adolescents With Visual ImpairmentIulia PintilieNo ratings yet
- Children With Mental Disorders: Making Sense of Their Needs and The Systems That Help ThemDocument24 pagesChildren With Mental Disorders: Making Sense of Their Needs and The Systems That Help Thembellydanceafrica9540No ratings yet
- Our Children Deserve Better Prevention Pays Annual Report of The Chief Medical Officer 2012 Chapter 10 Mental Health Problems in Children and YoungDocument13 pagesOur Children Deserve Better Prevention Pays Annual Report of The Chief Medical Officer 2012 Chapter 10 Mental Health Problems in Children and YoungSTOICESCU ANDREEA-DUMITRANo ratings yet
- Leyla - Suleymanli - Depression Among TeenagersDocument8 pagesLeyla - Suleymanli - Depression Among TeenagersLeyla SuleymanliNo ratings yet
- Chapter 1 3.Document14 pagesChapter 1 3.Renebel ClementeNo ratings yet
- Rates of Nonsuicidal Self-Injury in YouthDocument9 pagesRates of Nonsuicidal Self-Injury in YouthWilson Javier Dominguez PerezNo ratings yet
- Tapos Na PaghihirapDocument41 pagesTapos Na Paghihirapharreh hotdoggssNo ratings yet
- Associations Between Childhood Trauma, Bullying and Psychotic Symptoms Among A School-Based Adolescent SampleDocument6 pagesAssociations Between Childhood Trauma, Bullying and Psychotic Symptoms Among A School-Based Adolescent SampleChRist LumingkewasNo ratings yet
- Article crtique 1Document3 pagesArticle crtique 1isharajput29No ratings yet
- Its Okay To Not Be Okay An Analysis of Teen Mental HealthDocument14 pagesIts Okay To Not Be Okay An Analysis of Teen Mental Healthapi-539090707No ratings yet
- TM Revised Student Final 2017Document75 pagesTM Revised Student Final 2017conheoconNo ratings yet
- Publishable FinalzDocument19 pagesPublishable FinalzDanica Joy Vinluan JacobaNo ratings yet
- Bullying During Childhood Linked to Risk of Self-Harm in AdolescenceDocument13 pagesBullying During Childhood Linked to Risk of Self-Harm in AdolescenceBarry BurijonNo ratings yet
- What Is Causing The Increase in TeenDocument13 pagesWhat Is Causing The Increase in TeenBrittney LancasterNo ratings yet
- Child Abuse & Neglect: Johan Melander Hagborg, Inga Tidefors, Claudia FahlkeDocument11 pagesChild Abuse & Neglect: Johan Melander Hagborg, Inga Tidefors, Claudia FahlkeYee Mon AungNo ratings yet
- Social Anxiety in AdolescentsDocument8 pagesSocial Anxiety in AdolescentsMuskan SinghNo ratings yet
- Research Essay - Maggie Ott 8Document12 pagesResearch Essay - Maggie Ott 8api-609693092No ratings yet
- Behavioural, Emotional and Social Development of Children Who StutterDocument10 pagesBehavioural, Emotional and Social Development of Children Who StutterMagaliNo ratings yet
- Mood Disorders in YouthDocument10 pagesMood Disorders in Youthapi-401935214No ratings yet
- Mental HealthDocument6 pagesMental HealthLiza Mae PisiaoNo ratings yet
- Iceberg Model of WellnessDocument10 pagesIceberg Model of WellnessUnihealth Southwoods NursingNo ratings yet
- The Experiences of Fathers With Psychosis: Erik Evenson, John Rhodes, Janet Feigenbaum, & Anna SollyDocument15 pagesThe Experiences of Fathers With Psychosis: Erik Evenson, John Rhodes, Janet Feigenbaum, & Anna SollyAbhinavNo ratings yet
- Wahl, O. E. (2002) - Children's Views of Mental Illness A Review of the Literature. ν PDFDocument26 pagesWahl, O. E. (2002) - Children's Views of Mental Illness A Review of the Literature. ν PDFchrissanthiNo ratings yet
- 69 A 81410 Ee 84 A 94942 CDDocument10 pages69 A 81410 Ee 84 A 94942 CDapi-551175314No ratings yet
- schizophrenia evaluation 1Document4 pagesschizophrenia evaluation 1hajarazam04No ratings yet
- Effects of Dysfunctional Families on TeenagersDocument3 pagesEffects of Dysfunctional Families on TeenagersBlackdeath RoyaltyNo ratings yet
- Research Study PaperDocument16 pagesResearch Study Papergisselle.gigi.ortegaNo ratings yet
- Child Maltreatment and Mental Health Problems in Adulthood Birth Cohort StudyDocument6 pagesChild Maltreatment and Mental Health Problems in Adulthood Birth Cohort Studyfotosiphone 8No ratings yet
- DCFS: Medical Lens IRRDocument6 pagesDCFS: Medical Lens IRRdiyaNo ratings yet
- Childhood Trauma:Impact On Personality/Role in Personality DisordersDocument13 pagesChildhood Trauma:Impact On Personality/Role in Personality DisordersNancee Y.No ratings yet
- Cognitive Therapy For Social Anxiety Disorder in Adolescents A Development Case SeriesDocument17 pagesCognitive Therapy For Social Anxiety Disorder in Adolescents A Development Case Serieskahfi HizbullahNo ratings yet
- Adolescence Reviewer Physical DevelopmentDocument6 pagesAdolescence Reviewer Physical DevelopmentAngela JuanitoNo ratings yet
- Bailey Holland - A Good OneDocument6 pagesBailey Holland - A Good Oneapi-550077467No ratings yet
- Webinar Slides: Eileen Elias, M. Ed. and Douglas Waite, M.D.Document28 pagesWebinar Slides: Eileen Elias, M. Ed. and Douglas Waite, M.D.fasdunited100% (1)
- Adhd, Self-Harm, and Suicide: Risk Factors and Recommendations For ParentsDocument3 pagesAdhd, Self-Harm, and Suicide: Risk Factors and Recommendations For ParentsAtharvaNo ratings yet
- Mental Health Summit Dra. MedinaDocument14 pagesMental Health Summit Dra. MedinaMICHELLE GUMANGANNo ratings yet
- Psychologica Stress Childhood Dev MyopiaDocument8 pagesPsychologica Stress Childhood Dev MyopiaMartín GonzálezNo ratings yet
- Guiding PrinciplesDocument17 pagesGuiding PrinciplesLuna ValoNo ratings yet
- Adolescent Depression Literature ReviewDocument8 pagesAdolescent Depression Literature Reviewc5hzgcdj100% (1)
- Impact of Epilepsy in Adolescence: A Uk Controlled Study: Gus A. Baker, Shiri Spector, Yuko Mcgrath, Helen SoteriouDocument7 pagesImpact of Epilepsy in Adolescence: A Uk Controlled Study: Gus A. Baker, Shiri Spector, Yuko Mcgrath, Helen SoteriouSamantha EronNo ratings yet
- Chapter 1 3 ThesisDocument21 pagesChapter 1 3 ThesisJohn Patriarca0% (1)
- Pepsi ScreeningDocument12 pagesPepsi Screeningapi-549779066No ratings yet
- (696557968) Sifra JurnalDocument9 pages(696557968) Sifra JurnalSifra Turu AlloNo ratings yet
- Teenage Suicide Research PaperDocument5 pagesTeenage Suicide Research Paperefdkhd4e100% (1)
- Ege Land 2009Document5 pagesEge Land 2009RavennaNo ratings yet
- BCS - SS-CRM 460 - 2 Jun2019Document2 pagesBCS - SS-CRM 460 - 2 Jun2019Peterson SudlabNo ratings yet
- Klein After BachelardDocument13 pagesKlein After Bachelardyupengw122No ratings yet
- Evaluation of Green Building in The Existing Building of The Department of The Environment of DKI Jakarta Province in The Order of Reducing Greenhouse Gas EmissionsDocument5 pagesEvaluation of Green Building in The Existing Building of The Department of The Environment of DKI Jakarta Province in The Order of Reducing Greenhouse Gas EmissionsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Big Data Maturity ModelDocument6 pagesBig Data Maturity Modelkatherine976No ratings yet
- Human Strategies For A Virtual World: Baldwin BergesDocument32 pagesHuman Strategies For A Virtual World: Baldwin BergesmoisesNo ratings yet
- Digital Signal Processing Exam QuestionsDocument8 pagesDigital Signal Processing Exam QuestionsecehodaietNo ratings yet
- Security in Communications and StorageDocument27 pagesSecurity in Communications and StorageAfonso DelgadoNo ratings yet
- Identifikasi Risiko Pada Proyek KonstruksiDocument6 pagesIdentifikasi Risiko Pada Proyek Konstruksiair_langgNo ratings yet
- Colonial Philippines in Transition - SEA StudiesDocument197 pagesColonial Philippines in Transition - SEA StudiesYong Mosqueda100% (1)
- Experiment No. 2 Introduction To Combinational Circuits: Group Name: Group 7 Group Leader: JOSE DOROSAN Group MemberDocument11 pagesExperiment No. 2 Introduction To Combinational Circuits: Group Name: Group 7 Group Leader: JOSE DOROSAN Group MemberJoy PeconcilloNo ratings yet
- Inside Earth's LayersDocument2 pagesInside Earth's Layersansh parasharNo ratings yet
- Ogp1 Pintura PDFDocument19 pagesOgp1 Pintura PDFEl_memito100% (1)
- Project Plan For Implementation of ISO 20000 20000academy ENDocument7 pagesProject Plan For Implementation of ISO 20000 20000academy ENit20645984 Imashi H.M.G.G.M.No ratings yet
- R6020ANX - 12 Datasheet (PDF) - RohmDocument14 pagesR6020ANX - 12 Datasheet (PDF) - RohmNguyen Lan RivaretNo ratings yet
- Delhi Skill and Entrepreneurship University: Application Form Session 2021-2022Document3 pagesDelhi Skill and Entrepreneurship University: Application Form Session 2021-2022Shyam DubeyNo ratings yet
- კემპბელი თ16 353 363 დნმ და რეპლიკაციაDocument11 pagesკემპბელი თ16 353 363 დნმ და რეპლიკაციაSosoNo ratings yet
- Chapter 9 & Chapter 10 SolutionsDocument7 pagesChapter 9 & Chapter 10 SolutionsSaeed IqbalNo ratings yet
- TX AsiaDemandForecast 2018Document12 pagesTX AsiaDemandForecast 2018Muhammad AsadNo ratings yet
- Bank Reconciliation Step-By-Step TutorialDocument20 pagesBank Reconciliation Step-By-Step TutorialTạ Tuấn DũngNo ratings yet
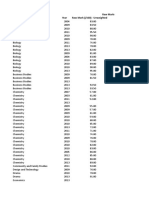
- Raw To Scaled Mark DatabaseDocument10 pagesRaw To Scaled Mark DatabaseKelly ChuNo ratings yet
- Development of High Temperature Superconducting Transformers PDFDocument6 pagesDevelopment of High Temperature Superconducting Transformers PDFBen McConnellNo ratings yet
- Fluxus F/G722: Non-Intrusive Ultrasonic Flow Meter For Highly Dynamic FlowsDocument2 pagesFluxus F/G722: Non-Intrusive Ultrasonic Flow Meter For Highly Dynamic FlowslossaladosNo ratings yet
- Igcse Chemistry Topic 13 Carbonates AnsDocument7 pagesIgcse Chemistry Topic 13 Carbonates AnsCClfourNo ratings yet
- Acknowledgements: Godrej & Boyce MFG - Co.LtdDocument83 pagesAcknowledgements: Godrej & Boyce MFG - Co.LtdSamarth TuliNo ratings yet