You might also like
- England Anaerobic Endurance TestDocument6 pagesEngland Anaerobic Endurance TestRyan Gibney80% (5)
- Board Review in Preventive Medicine and Public HealthFrom EverandBoard Review in Preventive Medicine and Public HealthRating: 3.5 out of 5 stars3.5/5 (2)
- CORE4 ABS Month 1 Workouts PDFDocument9 pagesCORE4 ABS Month 1 Workouts PDFkamehouse100% (1)
- iGB Marketplace Directory iGB Marketplace Directory 2020Document132 pagesiGB Marketplace Directory iGB Marketplace Directory 2020mirrors mirrorsNo ratings yet
- World Soccer - World Cup Special - 2022Document150 pagesWorld Soccer - World Cup Special - 2022madebyagra100% (2)
- Brooks Kubik - The Dinosaur Strength Training NotebookDocument100 pagesBrooks Kubik - The Dinosaur Strength Training NotebookAlJ79100% (21)
- Pdhpe HSC MG 2013Document27 pagesPdhpe HSC MG 2013Duncan LinNo ratings yet
- Pdhpe HSC MG 2015Document26 pagesPdhpe HSC MG 2015Duncan LinNo ratings yet
- Pdhpe HSC MG 2012Document18 pagesPdhpe HSC MG 2012Duncan LinNo ratings yet
- 2018 HSC Personal Development, Health and Physical Education Marking GuidelinesDocument30 pages2018 HSC Personal Development, Health and Physical Education Marking GuidelinesCristina KadelNo ratings yet
- Pdhpe HSC MG 2010Document13 pagesPdhpe HSC MG 2010Duncan LinNo ratings yet
- Pdhpe HSC MG 2011Document14 pagesPdhpe HSC MG 2011Duncan LinNo ratings yet
- PDHPE 2015 AnswersDocument11 pagesPDHPE 2015 AnswersSophie DinaroNo ratings yet
- 2014 MG Aboriginal StudiesDocument29 pages2014 MG Aboriginal StudiesSomeguy123551234512No ratings yet
- Beacon Schools Project Health Education Level 8 Planning Guide Section 6Document8 pagesBeacon Schools Project Health Education Level 8 Planning Guide Section 6api-3803295No ratings yet
- IGPH Assignment Guidance - 2023-2024Document22 pagesIGPH Assignment Guidance - 2023-2024ashraf.uk.360No ratings yet
- 8hpe Health Promotion Assessment - Cover Sheet and TaskDocument7 pages8hpe Health Promotion Assessment - Cover Sheet and Taskapi-500494073No ratings yet
- PHPIH 2022 Summative Assignment FINAL 2023 (2) - 1464449417Document7 pagesPHPIH 2022 Summative Assignment FINAL 2023 (2) - 1464449417Assignment CriticNo ratings yet
- Section 3: Beacon Schools Project Health Education Level 8 Planning Guide 2006Document15 pagesSection 3: Beacon Schools Project Health Education Level 8 Planning Guide 2006api-3803295No ratings yet
- Prelim Topic 1 IhcsDocument27 pagesPrelim Topic 1 IhcsKim T. EstimoNo ratings yet
- Health and Social Care: Ocr Level 2 Cambridge TechnicalDocument8 pagesHealth and Social Care: Ocr Level 2 Cambridge TechnicalLiza GomezNo ratings yet
- Pdhpe 2 KiDocument14 pagesPdhpe 2 Kiapi-371716913No ratings yet
- Generic Questionnaires in Assessment of Quality of LifeDocument17 pagesGeneric Questionnaires in Assessment of Quality of LifeachyutNo ratings yet
- Week 1 PPT Community ConceptsDocument48 pagesWeek 1 PPT Community ConceptsK DNo ratings yet
- Human Health and Development 3&4Document560 pagesHuman Health and Development 3&4Patricia Willow100% (1)
- Nursing Care of The Community CHP 7Document20 pagesNursing Care of The Community CHP 7Patricia Mag-akatNo ratings yet
- Royal Society For Public HealthDocument13 pagesRoyal Society For Public HealthguriyaNo ratings yet
- Nursing Care of The Community CHP 7Document20 pagesNursing Care of The Community CHP 7marissaNo ratings yet
- Health Literacy: Applying Current Concepts To Improve Health Services and Reduce Health InequalitiesDocument10 pagesHealth Literacy: Applying Current Concepts To Improve Health Services and Reduce Health InequalitiesasriadiNo ratings yet
- Community ConceptsDocument45 pagesCommunity ConceptsPeach BubbleNo ratings yet
- Session Slides 2 - Understanding - HealthDocument22 pagesSession Slides 2 - Understanding - HealthOsman Abdul-MuminNo ratings yet
- Section 3: Beacon Schools Project Health Education Level 8 Planning Guide 2006Document29 pagesSection 3: Beacon Schools Project Health Education Level 8 Planning Guide 2006api-3803295No ratings yet
- Developing Health Promotion CompetencesDocument32 pagesDeveloping Health Promotion CompetencesAnwarNo ratings yet
- Pop202 - Block1 - Health, PH, PHC, Ebph, Mdgs and SdgsDocument65 pagesPop202 - Block1 - Health, PH, PHC, Ebph, Mdgs and SdgsMH ULLASHNo ratings yet
- Health Needs AssessmentDocument51 pagesHealth Needs Assessmentمحمد يوسف المصراتيNo ratings yet
- Assessment Tools in ObesityDocument39 pagesAssessment Tools in ObesityPatricio GGNo ratings yet
- Community Health Nursing 1 - 1st TopicDocument32 pagesCommunity Health Nursing 1 - 1st TopicPrincess C. SultanNo ratings yet
- CHN Lesson 6 - Edna Oct 1, 2020Document17 pagesCHN Lesson 6 - Edna Oct 1, 2020Edna Uneta RoblesNo ratings yet
- Physical Edu Sem 1Document2 pagesPhysical Edu Sem 1anushkaanandaniiiNo ratings yet
- M1U3 SolutionDocument25 pagesM1U3 SolutionaalaamahmoudNo ratings yet
- CHN LECDocument3 pagesCHN LECyasmingapaz30No ratings yet
- Community Nursing ProcessDocument10 pagesCommunity Nursing Processbuhari rabiuNo ratings yet
- Pencegahan Penyakit, Kecacatan Dan Kematian Pada Gizi Kesehatan MasyarakatDocument24 pagesPencegahan Penyakit, Kecacatan Dan Kematian Pada Gizi Kesehatan MasyarakatWina MarthaliaNo ratings yet
- The Validation of The Moorehead-Ardelt Quality of Life Questionnaire IIDocument9 pagesThe Validation of The Moorehead-Ardelt Quality of Life Questionnaire IIVictoria DowningNo ratings yet
- Learning Experience 3-wk Unit Plan RevisionDocument16 pagesLearning Experience 3-wk Unit Plan Revisionapi-704137769No ratings yet
- Introduction Ho-1Document282 pagesIntroduction Ho-1TEWODROS TADDESENo ratings yet
- Health Promotion LO1&2Document24 pagesHealth Promotion LO1&2Mohd Johari Mohd ShafuwanNo ratings yet
- Promoting Mental HealthDocument17 pagesPromoting Mental HealthDavid LyeluNo ratings yet
- ALKAN Health Science, Business & Technology College Health Education Credit Hrs-3Document55 pagesALKAN Health Science, Business & Technology College Health Education Credit Hrs-3Gizachew AsimareNo ratings yet
- Health Natl Ed Standards 2007Document4 pagesHealth Natl Ed Standards 2007api-369626876No ratings yet
- Nutrition Assessment IDocument59 pagesNutrition Assessment IAlanoud AlnuaimiNo ratings yet
- The Essential Role of The Nurse in Improving Health OutcomesDocument38 pagesThe Essential Role of The Nurse in Improving Health OutcomesYAMINIPRIYANNo ratings yet
- Promoting Health in Australia: Assessment TaskDocument4 pagesPromoting Health in Australia: Assessment TaskFlaaffyNo ratings yet
- Chapter 2 - History of Health Education as an Emerging ProfessionDocument2 pagesChapter 2 - History of Health Education as an Emerging ProfessionKheizelleMaeEscanillaNo ratings yet
- mnt2 In-ServiceDocument16 pagesmnt2 In-Serviceapi-581342636No ratings yet
- 2023 - CHN - Topic 1Document55 pages2023 - CHN - Topic 1Mc Cobert AlipioNo ratings yet
- Theories in CHNDocument61 pagesTheories in CHNkennethNo ratings yet
- g11 Health Unit PlanDocument7 pagesg11 Health Unit Planapi-263590842100% (1)
- Health Promotion 2Document7 pagesHealth Promotion 2Murad KurdiNo ratings yet
- Leadership Skills For Interprofessional PracticeDocument24 pagesLeadership Skills For Interprofessional Practiceapi-643822510No ratings yet
- NCM 113 Study Guide 5Document8 pagesNCM 113 Study Guide 5christine mercadoNo ratings yet
- Unit-2 - Lecturer-1Document17 pagesUnit-2 - Lecturer-1Manish SinghNo ratings yet
- Cph Lab Midterm TransesDocument12 pagesCph Lab Midterm Transeslewistulio004No ratings yet
- Population and Community Health Nursing 6Th Edition Clark Solutions Manual Full Chapter PDFDocument30 pagesPopulation and Community Health Nursing 6Th Edition Clark Solutions Manual Full Chapter PDFreality.brutmhk10100% (8)
- Community Nutrition Module Syllabus Update2021Document11 pagesCommunity Nutrition Module Syllabus Update2021Brit MorganNo ratings yet
- Pdhpe HSC MG 2014Document26 pagesPdhpe HSC MG 2014Duncan LinNo ratings yet
- Pdhpe HSC Sa 2009Document8 pagesPdhpe HSC Sa 2009Duncan LinNo ratings yet
- Pdhpe HSC Notes 2007Document27 pagesPdhpe HSC Notes 2007Duncan LinNo ratings yet
- Pdhpe HSC Sa 2009Document8 pagesPdhpe HSC Sa 2009Duncan LinNo ratings yet
- Upper SixthDocument11 pagesUpper SixthDuncan LinNo ratings yet
- Chapter 12: Gravity: Answers To Even-Numbered Conceptual QuestionsDocument22 pagesChapter 12: Gravity: Answers To Even-Numbered Conceptual QuestionsDuncan LinNo ratings yet
- Pre Thermodynamic PracticeDocument8 pagesPre Thermodynamic PracticeDuncan LinNo ratings yet
- 6.test Mix 2 (1h)Document4 pages6.test Mix 2 (1h)Duncan LinNo ratings yet
- Homework 1Document2 pagesHomework 1Duncan LinNo ratings yet
- Motion GraphDocument5 pagesMotion GraphDuncan LinNo ratings yet
- CamScanner 10-01-2021 14.26Document13 pagesCamScanner 10-01-2021 14.26Duncan LinNo ratings yet
- Logo of MalaysiaDocument10 pagesLogo of MalaysiaDuncan LinNo ratings yet
- Physic ElementryDocument3 pagesPhysic ElementryDuncan LinNo ratings yet
- 1.pre STPM Matrix Bridging Free Seminar 22 - 7 - 2021Document8 pages1.pre STPM Matrix Bridging Free Seminar 22 - 7 - 2021Duncan LinNo ratings yet
- Disember ClassDocument1 pageDisember ClassDuncan LinNo ratings yet
- Grade 7-10 - 2ND Quarter MapehDocument18 pagesGrade 7-10 - 2ND Quarter MapehJunard CenizaNo ratings yet
- WhatsApp TajiDocument3 pagesWhatsApp Tajileeying limNo ratings yet
- Gedorered 2019 GR SDocument200 pagesGedorered 2019 GR SGeorge LogoNo ratings yet
- Old Top Gear GuideDocument163 pagesOld Top Gear Guideernststavroblofeld39No ratings yet
- CNKB - Faixas Pretas Ativos Fkba-CnkbDocument7 pagesCNKB - Faixas Pretas Ativos Fkba-CnkbDaniel TeixeiraNo ratings yet
- Line Up Full TimeDocument1 pageLine Up Full TimeSapwan AhmedNo ratings yet
- Commonwealth Games 2010Document3 pagesCommonwealth Games 201025965757No ratings yet
- Shimla Himachal Pradesh: 25Th All India Kumar Surendra Singh Inter School Shooting Championship 05-10-2023 - 14-10-2023Document28 pagesShimla Himachal Pradesh: 25Th All India Kumar Surendra Singh Inter School Shooting Championship 05-10-2023 - 14-10-2023himanshushooter375No ratings yet
- Unit Test 1 Present Tenses-RemedialDocument2 pagesUnit Test 1 Present Tenses-RemedialTulus J. SiregarNo ratings yet
- 2unit 2 Gifts of Youth Exercises 8Document2 pages2unit 2 Gifts of Youth Exercises 8oumaima moursiaNo ratings yet
- Stanley Rous: Sir Stanley Ford Rous, CBE (25 April 1895 - 18 July 1986) Was AnDocument4 pagesStanley Rous: Sir Stanley Ford Rous, CBE (25 April 1895 - 18 July 1986) Was AnNageshrau KarmaliNo ratings yet
- Unit 5Document4 pagesUnit 5George Kevin TomasNo ratings yet
- Sachin InterviewDocument2 pagesSachin InterviewAvik MondalNo ratings yet
- 2020-21 Detroit Red Wings Training Camp RosterDocument1 page2020-21 Detroit Red Wings Training Camp RosterClickon DetroitNo ratings yet
- Languagecert Achiever B1 Entry Level 3 International Esol (Listening, Reading, Writing) Practice Paper 6Document17 pagesLanguagecert Achiever B1 Entry Level 3 International Esol (Listening, Reading, Writing) Practice Paper 6GordonPhillipsNo ratings yet
- Lotustoyota2zz FinalDocument8 pagesLotustoyota2zz FinalManuel Elias Espinoza HuamanNo ratings yet
- PhpgEaEC0 Olimpiada Po Anglijskomu Yazyku 5 KlassDocument12 pagesPhpgEaEC0 Olimpiada Po Anglijskomu Yazyku 5 KlassРыскул ИбайдуллаеваNo ratings yet
- Additional Mathematics SBA: Trivek RamballyDocument20 pagesAdditional Mathematics SBA: Trivek RamballyPner JInklageNo ratings yet
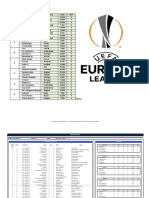
- UEFA Europa League 2019-2020 V1.67Document5 pagesUEFA Europa League 2019-2020 V1.67Gomv ConsNo ratings yet
- 14 Ninja300 4PBR en PDFDocument4 pages14 Ninja300 4PBR en PDFJuank Pulecio ReyesNo ratings yet
- FITTDocument1 pageFITTPhilip MarotoNo ratings yet
- Biomechanics of Javelin Throwing: Hans-Joachim MenzelDocument14 pagesBiomechanics of Javelin Throwing: Hans-Joachim MenzelAnonymous sYX58BrtcNo ratings yet
- UK & Ireland Client List SEP 2022Document4 pagesUK & Ireland Client List SEP 2022Azie AziatiNo ratings yet
- History of SwimmingDocument6 pagesHistory of SwimmingSkyNayvieNo ratings yet
- As TRC2 Mid-Year TestDocument2 pagesAs TRC2 Mid-Year TesttanyaNo ratings yet