You might also like
- Internal Med EORDocument57 pagesInternal Med EORAndrew BowmanNo ratings yet
- L8 - Water Soluble VitaminDocument38 pagesL8 - Water Soluble VitaminTrungNo ratings yet
- Gynaecology and Obstetrics PDFDocument50 pagesGynaecology and Obstetrics PDFabdulmoiz92No ratings yet
- Anatomy of The Coronary Arteries and VeinsDocument80 pagesAnatomy of The Coronary Arteries and Veinstreelife111No ratings yet
- BloodDocument6 pagesBloodDanielaTanase100% (1)
- CCRN-PCCN-CMC Review Cardiac Part 2Document21 pagesCCRN-PCCN-CMC Review Cardiac Part 2Giovanni Mictil100% (1)
- Pernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisDocument53 pagesPernicious Anemia: BSMT 3D Group 1 Paniza, Erika Joy Villanueva, Andrewarnold Yandan, CharisAndrew Arnold David VillanuevaNo ratings yet
- Uworld NotesDocument12 pagesUworld NotesTush Rame100% (1)
- Pediatric Cardiovascular DiseasesDocument4 pagesPediatric Cardiovascular DiseasesWendy EscalanteNo ratings yet
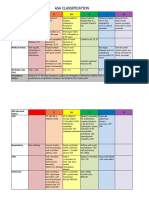
- ASA Physical Status ClassificationDocument1 pageASA Physical Status ClassificationАндрій ДанильцівNo ratings yet
- Pharmacology Quick HitsDocument6 pagesPharmacology Quick HitsHuma Hameed DogarNo ratings yet
- Clinical LaboratoriesDocument24 pagesClinical Laboratoriespdamodar200788% (8)
- Laboratory Activity No 2 - GLOVA-NDDocument4 pagesLaboratory Activity No 2 - GLOVA-NDandreyou99No ratings yet
- Vital Signs LectureDocument67 pagesVital Signs LectureJayrelle D. SafranNo ratings yet
- Trauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiDocument39 pagesTrauma Ginjal: Sub Bagian Urologi Bagian/Smf Bedah FK Uns/Rsud Dr. MoewardiAtika SugiartoNo ratings yet
- Lymphatic System of The Dog BaumDocument219 pagesLymphatic System of The Dog BaumFelipeeNo ratings yet
- ASA Physical Status Classification System - UpToDateDocument2 pagesASA Physical Status Classification System - UpToDateDaniel Rico FuentesNo ratings yet
- ASACLASS Renew3Document3 pagesASACLASS Renew3docwepNo ratings yet
- Asa Physical Status Classification System: Severely Decreased EF 30%Document1 pageAsa Physical Status Classification System: Severely Decreased EF 30%lukashenriqueNo ratings yet
- Asa Physical Status Classification SystemDocument2 pagesAsa Physical Status Classification SystemDerilandry Isham Aprildhy100% (1)
- Domingo LucianiDocument13 pagesDomingo LucianiAlex AlbornozNo ratings yet
- Medical Conditions and Illnesses-LaminatedDocument1 pageMedical Conditions and Illnesses-LaminatedxydasNo ratings yet
- ASA Classification (December 2020)Document4 pagesASA Classification (December 2020)arturo castilloNo ratings yet
- Bariatric Surgery ComplicationsDocument24 pagesBariatric Surgery ComplicationsAhmad AkaderNo ratings yet
- Care Plan 2020Document19 pagesCare Plan 2020api-547212356No ratings yet
- Disorders of Nutrition: Environmental PathologyDocument66 pagesDisorders of Nutrition: Environmental Pathologyjulo_05No ratings yet
- Ambo University: MonitoringDocument251 pagesAmbo University: Monitoringmubarek husienNo ratings yet
- PEH Page 1Document5 pagesPEH Page 1Chesley CarolinoNo ratings yet
- Vitamin Mineral Reference GuideDocument2 pagesVitamin Mineral Reference GuideEleni KostaraNo ratings yet
- 134 FullDocument2 pages134 FullSoi LidaNo ratings yet
- Anemia of Chronic DiseaseDocument13 pagesAnemia of Chronic Diseasemaverick mazeNo ratings yet
- Barış Yurtsever 142001022Document3 pagesBarış Yurtsever 142001022Barış YurtseverNo ratings yet
- Vitamin Summary SheetDocument8 pagesVitamin Summary Sheetglenn johnstonNo ratings yet
- Nursing Cram Sheet - 4Document1 pageNursing Cram Sheet - 4Reeya RayamajhiNo ratings yet
- College of Nursing: Brand Name: Cardizem Generic Name: Diltiazem Drug Classification: Calcium Channel BlockersDocument2 pagesCollege of Nursing: Brand Name: Cardizem Generic Name: Diltiazem Drug Classification: Calcium Channel BlockersChristine Pialan SalimbagatNo ratings yet
- Michael Brian Umali 3A:G6 Classification & BDocument3 pagesMichael Brian Umali 3A:G6 Classification & Bexcel21121No ratings yet
- 10.28.09 C Williams Megaloblastic AnemiasDocument25 pages10.28.09 C Williams Megaloblastic AnemiasmuliamayangsariNo ratings yet
- Barecuatro - Module 2 - Drug Study (Folic Acid)Document2 pagesBarecuatro - Module 2 - Drug Study (Folic Acid)ANGELICA CLAIRE BARECUATRONo ratings yet
- Medical Nutrition Therapy For Neurologic DisordersDocument128 pagesMedical Nutrition Therapy For Neurologic DisordersjwhssanNo ratings yet
- Pernicious Anemia Refers To A Lack of Vitamin b12 in The Body That Resulted To An Autoimmune Condition in Which The Body Does Not Produce Intrinsic Factor That Can Be AbsorbedDocument2 pagesPernicious Anemia Refers To A Lack of Vitamin b12 in The Body That Resulted To An Autoimmune Condition in Which The Body Does Not Produce Intrinsic Factor That Can Be AbsorbedJuan Miguel Caspe MangayaNo ratings yet
- NutritionDocument46 pagesNutritionPrince D. JacobNo ratings yet
- HTN & DM: Keara D. Acevedo, PTRPDocument31 pagesHTN & DM: Keara D. Acevedo, PTRPGIZELLE DELOS REYESNo ratings yet
- Adime 2 UchcDocument9 pagesAdime 2 Uchcapi-307029735No ratings yet
- Common Pediatric Nutritional Disorders 2015Document69 pagesCommon Pediatric Nutritional Disorders 2015Rhea Mii A Cruzado75% (4)
- Preoperative Evaluation HandoutDocument2 pagesPreoperative Evaluation HandoutAngelaTrinidadNo ratings yet
- Resident PresentationDocument17 pagesResident Presentationapi-610931702No ratings yet
- Farmakologi KardiovascularDocument49 pagesFarmakologi KardiovascularervinasetianingsihNo ratings yet
- Nursing Care Plan: Course InstructorsDocument11 pagesNursing Care Plan: Course InstructorsFatema AlsayariNo ratings yet
- Anesthesia Basics - AssignmentDocument3 pagesAnesthesia Basics - AssignmentTherese Jane TiradorNo ratings yet
- Hair, Nails, and Skin: Differentiating Cutaneous Manifestations of Micronutrient DeficiencyDocument14 pagesHair, Nails, and Skin: Differentiating Cutaneous Manifestations of Micronutrient DeficiencyIrving EuanNo ratings yet
- Case Study UrtiDocument9 pagesCase Study UrtiRonica GonzagaNo ratings yet
- Vegan Challenge IIVF2016Document30 pagesVegan Challenge IIVF2016Satyawira Aryawan DengNo ratings yet
- Tugas DR Nency: Oleh: Hartomas BumiharjoDocument20 pagesTugas DR Nency: Oleh: Hartomas Bumiharjohartomas bumiharjoNo ratings yet
- VitaminsDocument28 pagesVitaminsjoulen Ben LazregNo ratings yet
- Veterinary Clinics: Hypocalcemia: A Quick ReferenceDocument4 pagesVeterinary Clinics: Hypocalcemia: A Quick ReferenceDanilo JimenezNo ratings yet
- Medicine Review 2018 1Document470 pagesMedicine Review 2018 1Norjetalexis Maningo CabreraNo ratings yet
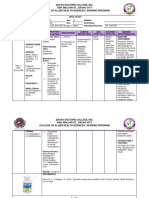
- College of Nursing: Pharmacological ManagementDocument4 pagesCollege of Nursing: Pharmacological ManagementBianca Mikaela DosdosNo ratings yet
- Pediatrics: Treatment of MalnutritionDocument4 pagesPediatrics: Treatment of Malnutritionapi-3829364No ratings yet
- Encyclopedia of Conditions and Their SupplementsDocument87 pagesEncyclopedia of Conditions and Their SupplementsSalah UddinNo ratings yet
- Vitamin EDocument29 pagesVitamin ESiva Krishna NeppaliNo ratings yet
- 1. Bài giảng Chẩn đoán và điều trị bệnh lý động mạch ngoại biênDocument112 pages1. Bài giảng Chẩn đoán và điều trị bệnh lý động mạch ngoại biênThuy LaNo ratings yet
- NUTRIIIDocument5 pagesNUTRIIIShania CabucosNo ratings yet
- Iron Deficiency Anemia: A Clinical Case StudyDocument4 pagesIron Deficiency Anemia: A Clinical Case StudyMela IndriyaniNo ratings yet
- Drug StudyDocument8 pagesDrug StudyRosemarie CarpioNo ratings yet
- A Simple Guide to Vitamin B12 Anemia, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Vitamin B12 Anemia, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Barriers To Exclusive Breastfeeding Among Urban Mothers: Original ArticleDocument5 pagesBarriers To Exclusive Breastfeeding Among Urban Mothers: Original ArticleEno RLNo ratings yet
- Adult Intussusception: A Retrospective ReviewDocument5 pagesAdult Intussusception: A Retrospective ReviewkameliasitorusNo ratings yet
- Journal of Behavior Therapy and Experimental PsychiatryDocument7 pagesJournal of Behavior Therapy and Experimental PsychiatryBella ZulitaNo ratings yet
- Drugs Used in Otology and Their FormulationsDocument4 pagesDrugs Used in Otology and Their FormulationsAnish RajNo ratings yet
- 3 Q Epidemiology Part 1Document26 pages3 Q Epidemiology Part 1Prince GoelNo ratings yet
- OSCE ProceduresDocument16 pagesOSCE ProceduresQueen ShNo ratings yet
- CTK-USA (Aria) : End User Price List-Rapid TestDocument2 pagesCTK-USA (Aria) : End User Price List-Rapid TestAbdalazeez AlsayedNo ratings yet
- A Study To Assess The Prevalence of TattDocument5 pagesA Study To Assess The Prevalence of Tatt高權梁No ratings yet
- LKPD - Recount Text 2Document2 pagesLKPD - Recount Text 2Sabian KalifiNo ratings yet
- Mechanism Readmisi Referral Pattern Degenerative Diseases With The Claim of Bpjs in In-Patient Departement Rsud DR.H Soewondo Kendal The Year 2015Document8 pagesMechanism Readmisi Referral Pattern Degenerative Diseases With The Claim of Bpjs in In-Patient Departement Rsud DR.H Soewondo Kendal The Year 2015ᎷᏒ.ᏴᎬᎪᏚᎢ.No ratings yet
- INFERTILITYDocument31 pagesINFERTILITYShivam. KumarNo ratings yet
- Approach To A Patient With AstigmatismDocument57 pagesApproach To A Patient With AstigmatismNarendra N Naru100% (1)
- Week 1 IntroductionDocument13 pagesWeek 1 Introductionobai AlhwimelNo ratings yet
- Alcohol Withdrawal - StatPearls - NCBI BookshelfDocument7 pagesAlcohol Withdrawal - StatPearls - NCBI BookshelfDAFNE FRANÇA SANTANANo ratings yet
- NCP and Patients Profile - Pre Clinical Duty2006Document4 pagesNCP and Patients Profile - Pre Clinical Duty2006api-3718174No ratings yet
- Hospital Diet and Oral Nutritional Supplements (Sip Feeds)Document16 pagesHospital Diet and Oral Nutritional Supplements (Sip Feeds)Patrick nyawiraNo ratings yet
- 3 Lebanese Code of EthicsDocument72 pages3 Lebanese Code of Ethicsali abdel hadiNo ratings yet
- Complex Regional Pain Syndrome (CRPS) : CausesDocument1 pageComplex Regional Pain Syndrome (CRPS) : CausesMarisa OktavianaNo ratings yet
- Lab Flow SheetDocument2 pagesLab Flow SheetRyan LazatinNo ratings yet
- Adequacy of PerfusionDocument11 pagesAdequacy of PerfusionLaiba SiddiqueNo ratings yet
- Educational Manual Masterword SCD English FINALDocument111 pagesEducational Manual Masterword SCD English FINALbranchardmushabeNo ratings yet
- The Internet The Main Source of HIV AIDS Information On StudentsDocument5 pagesThe Internet The Main Source of HIV AIDS Information On StudentsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- LAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloDocument4 pagesLAS HEALTH 6 Q4 Wk5 Cherlyn. RonquilloANGELINA RAMBOYONGNo ratings yet
- Epidemiology NewDocument26 pagesEpidemiology NewBabita DhruwNo ratings yet
- Clinical Group Study Case 1Document8 pagesClinical Group Study Case 1Olivia JagroopNo ratings yet