You might also like
- Serv7107 V05N01 TXT7Document32 pagesServ7107 V05N01 TXT7azry_alqadry100% (6)
- Essene Moses Ten CommandmentsDocument4 pagesEssene Moses Ten Commandmentsjeryon91No ratings yet
- Copy Resit APLC MiniAssignmentDocument5 pagesCopy Resit APLC MiniAssignmentChong yaoNo ratings yet
- Ebook PDF Traditions Encounters A Brief Global History 4th Edition PDFDocument41 pagesEbook PDF Traditions Encounters A Brief Global History 4th Edition PDFmarvin.anwar208100% (31)
- Ebook PDF Understanding Biology 3rd Edition by Kenneth Mason PDFDocument41 pagesEbook PDF Understanding Biology 3rd Edition by Kenneth Mason PDFrichard.rogers744100% (33)
- Ebook PDF Traffic and Highway Engineering Enhanced Edition 5th Edition PDFDocument29 pagesEbook PDF Traffic and Highway Engineering Enhanced Edition 5th Edition PDFmarvin.anwar208100% (32)
- Hajj A Practical Guide-Imam TahirDocument86 pagesHajj A Practical Guide-Imam TahirMateen YousufNo ratings yet
- Boraschi PDFDocument476 pagesBoraschi PDFmbiancar100% (1)
- Ebook PDF Understanding Assessing and Teaching Reading A Diagnostic Approach 7th Edition PDFDocument41 pagesEbook PDF Understanding Assessing and Teaching Reading A Diagnostic Approach 7th Edition PDFjimmie.smith693100% (31)
- Akhmatova, Anna - 45 Poems With Requiem PDFDocument79 pagesAkhmatova, Anna - 45 Poems With Requiem PDFAnonymous 6N5Ew3No ratings yet
- Ebook PDF Twenty Lessons in Environmental Sociology 2nd PDFDocument41 pagesEbook PDF Twenty Lessons in Environmental Sociology 2nd PDFalicia.mclaughlin973100% (30)
- ACL GRC Risk Manager - Usage Guide V1.1Document28 pagesACL GRC Risk Manager - Usage Guide V1.1Rohit ShettyNo ratings yet
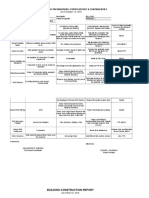
- Class Opening Preparations Status ReportDocument3 pagesClass Opening Preparations Status ReportMaria Theresa Buscato86% (7)
- Variables in Language Teaching - The Role of The TeacherDocument34 pagesVariables in Language Teaching - The Role of The TeacherFatin AqilahNo ratings yet
- Ebook PDF The Inclusive Classroom Strategies For Effective Differentiated Instruction 6th Edition PDFDocument41 pagesEbook PDF The Inclusive Classroom Strategies For Effective Differentiated Instruction 6th Edition PDFscott.stokley449100% (34)
- Ebook PDF Turbulence An Introduction For Scientists and Engineers 2nd Edition PDFDocument41 pagesEbook PDF Turbulence An Introduction For Scientists and Engineers 2nd Edition PDFalicia.mclaughlin973100% (29)
- Ebook PDF Twentieth Century World An International History PDFDocument41 pagesEbook PDF Twentieth Century World An International History PDFalicia.mclaughlin973100% (30)
- Ebook PDF Troubling Education Queer Activism and Anti Oppressive Pedagogy PDFDocument47 pagesEbook PDF Troubling Education Queer Activism and Anti Oppressive Pedagogy PDFalicia.mclaughlin973100% (31)
- Ebook PDF Turbomachinery Basic Theory and Applications Second Edition PDFDocument41 pagesEbook PDF Turbomachinery Basic Theory and Applications Second Edition PDFalicia.mclaughlin973100% (30)
- Ebook PDF Twenty First Century Musicals From Stage To Screen PDFDocument41 pagesEbook PDF Twenty First Century Musicals From Stage To Screen PDFalicia.mclaughlin973100% (32)
- Ebook PDF Trigonometry 4th by Mark Dugopolski PDFDocument41 pagesEbook PDF Trigonometry 4th by Mark Dugopolski PDFalicia.mclaughlin973100% (31)
- Ebook PDF Ultrasound For Advanced Practitioners in Pregnancy and Womens Health PDFDocument48 pagesEbook PDF Ultrasound For Advanced Practitioners in Pregnancy and Womens Health PDFjimmie.smith693100% (30)
- Ebook PDF Trends of Environmental Forensics in Pakistan PDFDocument47 pagesEbook PDF Trends of Environmental Forensics in Pakistan PDFernest.kirschenbaum650100% (32)
- Ebook PDF Transportation A Global Supply Chain Perspective 9th Edition PDFDocument41 pagesEbook PDF Transportation A Global Supply Chain Perspective 9th Edition PDFernest.kirschenbaum650100% (36)
- Ebook PDF TX Gov 1st Edition by William Earl Maxwell PDFDocument41 pagesEbook PDF TX Gov 1st Edition by William Earl Maxwell PDFjimmie.smith693100% (36)
- Ebook PDF Treating Those With Mental Disorders A Comprehensive Approac 2nd Edition PDFDocument42 pagesEbook PDF Treating Those With Mental Disorders A Comprehensive Approac 2nd Edition PDFernest.kirschenbaum650100% (29)
- Ebook PDF Transforming Learning With New Technologies 3rd Edition PDFDocument41 pagesEbook PDF Transforming Learning With New Technologies 3rd Edition PDFernest.kirschenbaum650100% (31)
- Ebook PDF Understanding and Managing Diversity Readings Cases and Exercises 6th Edition PDFDocument41 pagesEbook PDF Understanding and Managing Diversity Readings Cases and Exercises 6th Edition PDFjimmie.smith69397% (31)
- Ebook PDF Understandable Statistics Concepts and Methods 12th Edition PDFDocument41 pagesEbook PDF Understandable Statistics Concepts and Methods 12th Edition PDFjimmie.smith693100% (30)
- Ebook PDF Understanding and Applying Medical Anthropology 3rd Edition PDFDocument41 pagesEbook PDF Understanding and Applying Medical Anthropology 3rd Edition PDFjimmie.smith693100% (31)
- Ebook PDF Understandable Statistics 11th Edition by Charles Henry Brase PDFDocument41 pagesEbook PDF Understandable Statistics 11th Edition by Charles Henry Brase PDFjimmie.smith693100% (32)
- Ebook PDF Translational Medicine in Cns Drug Development Volume 29 PDFDocument41 pagesEbook PDF Translational Medicine in Cns Drug Development Volume 29 PDFernest.kirschenbaum650100% (33)
- Ebook PDF Transnational Management Text and Cases in Cross Border Management 8th Edition PDFDocument41 pagesEbook PDF Transnational Management Text and Cases in Cross Border Management 8th Edition PDFernest.kirschenbaum650100% (33)
- Ebook PDF Understanding Audio Getting The Most Out of Your Project or Professional Recording Studio 2nd Edition PDFDocument42 pagesEbook PDF Understanding Audio Getting The Most Out of Your Project or Professional Recording Studio 2nd Edition PDFjimmie.smith693100% (30)
- Ebook PDF Transition Economies Political Economy in Russia Eastern Europe and Central Asia PDFDocument41 pagesEbook PDF Transition Economies Political Economy in Russia Eastern Europe and Central Asia PDFernest.kirschenbaum650100% (33)
- Ebook PDF Understanding Basic Statistics 7th Edition PDFDocument41 pagesEbook PDF Understanding Basic Statistics 7th Edition PDFrichard.rogers744100% (35)
- Ebook PDF Understanding Bioinformatics by Marketa Zvelebil PDFDocument41 pagesEbook PDF Understanding Bioinformatics by Marketa Zvelebil PDFrichard.rogers744100% (31)
- Ebook PDF Training in Interpersonal Skills Tips For Managing People at Work 6th Edition PDFDocument41 pagesEbook PDF Training in Interpersonal Skills Tips For Managing People at Work 6th Edition PDFernest.kirschenbaum650100% (32)
- Ebook PDF Traditions Encounters A Global Perspective On The Past 6th Edition PDFDocument42 pagesEbook PDF Traditions Encounters A Global Perspective On The Past 6th Edition PDFmarvin.anwar208100% (31)
- Ebook PDF Ultimate Limit State Analysis and Design of Plated Structures 2nd Edition PDFDocument41 pagesEbook PDF Ultimate Limit State Analysis and Design of Plated Structures 2nd Edition PDFjimmie.smith693100% (33)
- Ebook PDF Transfer Pricing and The Arms Length Principle After Beps PDFDocument35 pagesEbook PDF Transfer Pricing and The Arms Length Principle After Beps PDFernest.kirschenbaum650100% (29)
- Ebook PDF Understanding Biology 2nd Edition PDFDocument41 pagesEbook PDF Understanding Biology 2nd Edition PDFrichard.rogers744100% (28)
- Ebook PDF Understanding Business Statistics 1st Edition PDFDocument41 pagesEbook PDF Understanding Business Statistics 1st Edition PDFrichard.rogers744100% (28)
- Solution Manual For Principles of Chemistry A Molecular Approach 3Rd Edition Tro 0321971949 9780321971944 Full Chapter PDFDocument36 pagesSolution Manual For Principles of Chemistry A Molecular Approach 3Rd Edition Tro 0321971949 9780321971944 Full Chapter PDFlaurie.dolezal936100% (11)
- Ebook PDF Traditions Encounters Volume 1 From The Beginning To 1500 6th Edition PDFDocument42 pagesEbook PDF Traditions Encounters Volume 1 From The Beginning To 1500 6th Edition PDFmarvin.anwar208100% (31)
- Basic Business Statistics 13Th Edition Berenson Test Bank Full Chapter PDFDocument36 pagesBasic Business Statistics 13Th Edition Berenson Test Bank Full Chapter PDFchristina.stinchcomb993100% (12)
- International Economics 14Th Edition Robert Carbaugh Solutions Manual Full Chapter PDFDocument26 pagesInternational Economics 14Th Edition Robert Carbaugh Solutions Manual Full Chapter PDFclifford.eakin819100% (14)
- Ebook PDF Traditions and Encounters A Brief Global History Vol 1 4th Edition PDFDocument41 pagesEbook PDF Traditions and Encounters A Brief Global History Vol 1 4th Edition PDFmarvin.anwar208100% (37)
- Basic Chemistry 4Th Edition Timberlake Test Bank Full Chapter PDFDocument36 pagesBasic Chemistry 4Th Edition Timberlake Test Bank Full Chapter PDFchristina.stinchcomb993100% (10)
- International Economics 12Th Edition Salvatore Test Bank Full Chapter PDFDocument41 pagesInternational Economics 12Th Edition Salvatore Test Bank Full Chapter PDFclifford.eakin819100% (12)
- Ebook PDF The Humanities Culture Continuity and Change Volume 1 3rd Edition PDFDocument41 pagesEbook PDF The Humanities Culture Continuity and Change Volume 1 3rd Edition PDFscott.stokley449100% (33)
- Carpentry Canadian 3Rd Edition Vogt Test Bank Full Chapter PDFDocument35 pagesCarpentry Canadian 3Rd Edition Vogt Test Bank Full Chapter PDFclaudette.sundermeyer830100% (9)
- Ebook PDF Traffic Engineering 5th Edition by Roger P Roess PDFDocument47 pagesEbook PDF Traffic Engineering 5th Edition by Roger P Roess PDFmarvin.anwar20897% (29)
- Canadian Income Taxation 2014 2015 Planning and Decision Making Canadian 17Th Edition Buckwold Test Bank Full Chapter PDFDocument36 pagesCanadian Income Taxation 2014 2015 Planning and Decision Making Canadian 17Th Edition Buckwold Test Bank Full Chapter PDFkenneth.cappello861100% (12)
- Cb4 4Th Edition Babin Test Bank Full Chapter PDFDocument36 pagesCb4 4Th Edition Babin Test Bank Full Chapter PDFclaudette.sundermeyer830100% (11)
- Ebook Ebook PDF Principles of Psychology by Marc Breedlove PDFDocument41 pagesEbook Ebook PDF Principles of Psychology by Marc Breedlove PDFpatrick.weber681100% (37)
- Download ebook Farm Management Pdf full chapter pdfDocument67 pagesDownload ebook Farm Management Pdf full chapter pdfmark.callis118100% (21)
- Download ebook Expertddx Chest Pdf full chapter pdfDocument67 pagesDownload ebook Expertddx Chest Pdf full chapter pdfscott.garcia931100% (20)
- International Economics 14Th Edition Robert Carbaugh Test Bank Full Chapter PDFDocument36 pagesInternational Economics 14Th Edition Robert Carbaugh Test Bank Full Chapter PDFclifford.eakin819100% (13)
- CB 6 6Th Edition Babin Solutions Manual Full Chapter PDFDocument36 pagesCB 6 6Th Edition Babin Solutions Manual Full Chapter PDFclaudette.sundermeyer830100% (13)
- Carpers Understanding The Law 7Th Edition Mckinsey Test Bank Full Chapter PDFDocument36 pagesCarpers Understanding The Law 7Th Edition Mckinsey Test Bank Full Chapter PDFclaudette.sundermeyer830100% (13)
- Download ebook Planetary Exploration Horizon 2061 A Long Term Perspective For Planetary Exploration Pdf full chapter pdfDocument67 pagesDownload ebook Planetary Exploration Horizon 2061 A Long Term Perspective For Planetary Exploration Pdf full chapter pdfjuan.holliday540100% (25)
- EBOOK Outcome Based Massage Putting Evidence Into Practice Third Edition Download Full Chapter PDF KindleDocument61 pagesEBOOK Outcome Based Massage Putting Evidence Into Practice Third Edition Download Full Chapter PDF Kindlemelody.todd120100% (33)
- Canadian Income Taxation 2014 2015 Planning and Decision Making Canadian 17Th Edition Buckwold Solutions Manual Full Chapter PDFDocument36 pagesCanadian Income Taxation 2014 2015 Planning and Decision Making Canadian 17Th Edition Buckwold Solutions Manual Full Chapter PDFkenneth.cappello861100% (14)
- Ebook PDF The International Business Environment 4th Edition PDFDocument41 pagesEbook PDF The International Business Environment 4th Edition PDFscott.stokley449100% (38)
- International Marketing 17Th Edition Cateora Test Bank Full Chapter PDFDocument36 pagesInternational Marketing 17Th Edition Cateora Test Bank Full Chapter PDFshaun.sebastian977100% (13)
- Cb4 4Th Edition Babin Solutions Manual Full Chapter PDFDocument36 pagesCb4 4Th Edition Babin Solutions Manual Full Chapter PDFclaudette.sundermeyer830100% (12)
- Solution Manual For Applied Social Research A Tool For The Human Services 9Th Edition Monette Sullivan Dejong 128507551X 9781285075518Document26 pagesSolution Manual For Applied Social Research A Tool For The Human Services 9Th Edition Monette Sullivan Dejong 128507551X 9781285075518julie.kindred302100% (15)
- Cyber Security 2017Document8 pagesCyber Security 2017Anonymous i1ClcyNo ratings yet
- Common Pesticides in AgricultureDocument6 pagesCommon Pesticides in AgricultureBMohdIshaqNo ratings yet
- GKInvest Market ReviewDocument66 pagesGKInvest Market ReviewjhonxracNo ratings yet
- A61C00100 Communication and Employee Engagement by Mary Welsh 2Document19 pagesA61C00100 Communication and Employee Engagement by Mary Welsh 2Moeshfieq WilliamsNo ratings yet
- SolarBright MaxBreeze Solar Roof Fan Brochure Web 1022Document4 pagesSolarBright MaxBreeze Solar Roof Fan Brochure Web 1022kewiso7811No ratings yet
- ElectricalDocument30 pagesElectricalketerNo ratings yet
- C11 Strategy DevelopmentDocument30 pagesC11 Strategy DevelopmentPARTI KEADILAN RAKYAT NIBONG TEBALNo ratings yet
- Guitar Chords:: Chorus: CF CF FCFC CFGC Verse: CF CF FCFC CFGCDocument17 pagesGuitar Chords:: Chorus: CF CF FCFC CFGC Verse: CF CF FCFC CFGCKhuanZumeNo ratings yet
- Lecture 29: Curl, Divergence and FluxDocument2 pagesLecture 29: Curl, Divergence and FluxKen LimoNo ratings yet
- Final - WPS PQR 86Document4 pagesFinal - WPS PQR 86Parag WadekarNo ratings yet
- Power Team PE55 ManualDocument13 pagesPower Team PE55 ManualTitanplyNo ratings yet
- Siga-Cc1 12-22-2010Document6 pagesSiga-Cc1 12-22-2010Felipe LozanoNo ratings yet
- Design ThinkingDocument16 pagesDesign ThinkingbhattanitanNo ratings yet
- PediculosisDocument14 pagesPediculosisREYMARK HACOSTA100% (1)
- GD&T WIZ Tutor Covers The Vast Breadth of Geometric Dimensioning and Tolerancing Without Compromising On The Depth. The Topics Covered AreDocument1 pageGD&T WIZ Tutor Covers The Vast Breadth of Geometric Dimensioning and Tolerancing Without Compromising On The Depth. The Topics Covered AreVinay ManjuNo ratings yet
- Oas Community College: Republic of The Philippines Commission On Higher Education Oas, AlbayDocument22 pagesOas Community College: Republic of The Philippines Commission On Higher Education Oas, AlbayJaycel NepalNo ratings yet
- An Overview of The FUPLA 2 Tools: Project DatabaseDocument2 pagesAn Overview of The FUPLA 2 Tools: Project DatabaseJulio Cesar Rojas SaavedraNo ratings yet
- Types of Speech StylesDocument31 pagesTypes of Speech StylesRomnick BistayanNo ratings yet
- TNG UPDATE InstructionsDocument10 pagesTNG UPDATE InstructionsDiogo Alexandre Crivelari CrivelNo ratings yet
- TNTCL Cost Data 2021 22Document95 pagesTNTCL Cost Data 2021 22Akd DeshmukhNo ratings yet
- Tuberculin Skin Test: Facilitator GuideDocument31 pagesTuberculin Skin Test: Facilitator GuideTiwi NaloleNo ratings yet
- 1571-1635319494618-Unit 04 Leadership and ManagementDocument48 pages1571-1635319494618-Unit 04 Leadership and ManagementdevindiNo ratings yet