You might also like
- Quick Study Guide To The Integumentary SystemDocument3 pagesQuick Study Guide To The Integumentary SystemMc Luis Glen AserdanoNo ratings yet
- The Integumentary System: Prepared byDocument12 pagesThe Integumentary System: Prepared byErick Torres Gozum100% (1)
- Lab Act 3 - Integumentary SystemdocxDocument8 pagesLab Act 3 - Integumentary SystemdocxmendozakaceeyNo ratings yet
- CH 5: Integumentary SystemDocument36 pagesCH 5: Integumentary SystemHurtlock HurtlockNo ratings yet
- Integumentary Lab ActDocument5 pagesIntegumentary Lab ActJASMINE LAURONNo ratings yet
- Burns SemDocument29 pagesBurns SemEsther Marie SazonNo ratings yet
- Journal Written Report - Scar Prevention With Prolonged Use of Tissue AdhesiveDocument13 pagesJournal Written Report - Scar Prevention With Prolonged Use of Tissue AdhesiveNeill CelesteNo ratings yet
- Integument System ActivityDocument5 pagesIntegument System ActivityeywatsarawatNo ratings yet
- Chapter 4 Integumentary SystemDocument5 pagesChapter 4 Integumentary SystemClarisse Anne QuinonesNo ratings yet
- SkinDocument22 pagesSkinloginhani40No ratings yet
- Topic 5 & 6Document18 pagesTopic 5 & 6PhoebeNo ratings yet
- Anatomy and Physiology of the Integumentary SystemDocument5 pagesAnatomy and Physiology of the Integumentary SystemVERGEL, Sophia Luis V.No ratings yet
- HUMAN ORGAN SYSTEMS: INTEGUMENTARY AND SKELETALDocument3 pagesHUMAN ORGAN SYSTEMS: INTEGUMENTARY AND SKELETALDenine Dela Rosa OrdinalNo ratings yet
- CH - 04 - SKIN AND BODY MEMBRANESDocument76 pagesCH - 04 - SKIN AND BODY MEMBRANESCheska DillupacNo ratings yet
- Skin Structure and FunctionsDocument25 pagesSkin Structure and FunctionsUniversal DiscoveringNo ratings yet
- Anaphy Mia Rev4Document4 pagesAnaphy Mia Rev4antonettevegamia3No ratings yet
- Anaphy Lab QuizDocument12 pagesAnaphy Lab QuizScout Beauty JHOINo ratings yet
- Anatomy & Physiology With Pathophysiology Lecture (Midterms)Document4 pagesAnatomy & Physiology With Pathophysiology Lecture (Midterms)Millen ArenasNo ratings yet
- Safari - Feb 21, 2024 at 11:56 AMDocument1 pageSafari - Feb 21, 2024 at 11:56 AMsyansyncNo ratings yet
- A&P Replaced Cheat SheetDocument6 pagesA&P Replaced Cheat SheetNihal AlamNo ratings yet
- Histology Department Medical Faculty Padjadjaran UniversityDocument40 pagesHistology Department Medical Faculty Padjadjaran Universityanisya venyNo ratings yet
- The Integumentary SystemDocument2 pagesThe Integumentary SystemKARYLLE JUNE PONTERASNo ratings yet
- IntegumentaryDocument5 pagesIntegumentaryNovie Roycell Fernandez RueloNo ratings yet
- Structure of Skin, Skin Problems, Hair Structure and Hair Growth CycleDocument8 pagesStructure of Skin, Skin Problems, Hair Structure and Hair Growth CycleRakshita GroverNo ratings yet
- Chapter 9: Skin and ITS APPENDAGES: (Vital Organs)Document4 pagesChapter 9: Skin and ITS APPENDAGES: (Vital Organs)Hannah Beatrice Adame TamayoNo ratings yet
- NeoNotes Derma HighlightedDocument32 pagesNeoNotes Derma Highlightedyomna.saaNo ratings yet
- Chapter 6: Integumentary SystemDocument12 pagesChapter 6: Integumentary SystemHoney VargasNo ratings yet
- 10 Patho Skin PathologyDocument27 pages10 Patho Skin PathologyMartin Tan100% (1)
- Activity 2 Part 1Document4 pagesActivity 2 Part 1Alejandra IndaNo ratings yet
- Workbook Activity #13: Integumentary System (Skin) General ObjectiveDocument5 pagesWorkbook Activity #13: Integumentary System (Skin) General ObjectiveAmbaw PutiiNo ratings yet
- Structure & Function of The SkinDocument9 pagesStructure & Function of The SkincNo ratings yet
- 5 - IntegDocument8 pages5 - IntegGel Austin PascuaNo ratings yet
- Skin and Its AppendagesDocument3 pagesSkin and Its AppendagesMarchylle Faye JimenezNo ratings yet
- Schwartz Cpap 16 Skin and Subcutaneous TissueDocument16 pagesSchwartz Cpap 16 Skin and Subcutaneous TissueRem AlfelorNo ratings yet
- Giải phẫu ứng dụngDocument54 pagesGiải phẫu ứng dụngDũng Hoàng Nghĩa TríNo ratings yet
- Integumentary System IncludesDocument29 pagesIntegumentary System IncludesRhena TogoresNo ratings yet
- 0.07 - 0.12 MM in Thickness But May Reach UpDocument8 pages0.07 - 0.12 MM in Thickness But May Reach UpCoy NuñezNo ratings yet
- Lai Cheong2013Document4 pagesLai Cheong2013Nirwana SeptianiNo ratings yet
- Activity 2 Part 1Document5 pagesActivity 2 Part 1Alejandra IndaNo ratings yet
- Chap3 Integ Anaphy NotesDocument11 pagesChap3 Integ Anaphy NotesAxel Neil VidalNo ratings yet
- Microscopic Analysis of The Integumentary SystemDocument9 pagesMicroscopic Analysis of The Integumentary SystemAgatha joy MadrazoNo ratings yet
- Integuementary System ReviewerDocument10 pagesInteguementary System ReviewerChloe Mikaela MonsantoNo ratings yet
- Anatomical Layers of The SkinDocument5 pagesAnatomical Layers of The SkinRyzelle Louise SorianoNo ratings yet
- Integumentary and Nervous System: 5141 CN 111 - Anatomy and PhysiologyDocument8 pagesIntegumentary and Nervous System: 5141 CN 111 - Anatomy and PhysiologyAlthea Joyce OngNo ratings yet
- Skin Appendages and FunctionsDocument24 pagesSkin Appendages and FunctionsChris Jardine LiNo ratings yet
- Intergumentary SystemDocument8 pagesIntergumentary SystemJSeasharkNo ratings yet
- Integumentary System (Lecture Outline) PDFDocument4 pagesIntegumentary System (Lecture Outline) PDFAndrea Yzabell CortezNo ratings yet
- PowerPoint - Presentation - About - Integumentary - SystemDocument27 pagesPowerPoint - Presentation - About - Integumentary - SystemPrayl Hope NapanoNo ratings yet
- Integumentary SystemDocument3 pagesIntegumentary SystemCarmela Cordon FelixNo ratings yet
- Integumentary System Epidermis Dermis: Stratum Corneum Stratum Lucidum Stratum Granulosum Papillary LayerDocument4 pagesIntegumentary System Epidermis Dermis: Stratum Corneum Stratum Lucidum Stratum Granulosum Papillary LayerNu Ri LeeNo ratings yet
- Structure and Function of the Skin ExplainedDocument9 pagesStructure and Function of the Skin Explainednh2411No ratings yet
- BM1011 2020 Study Guide For Module 3 The Integumentary SystemDocument14 pagesBM1011 2020 Study Guide For Module 3 The Integumentary SystemLaetitia ReyesNo ratings yet
- Skin and Its AppendagesDocument7 pagesSkin and Its AppendagesSheena PasionNo ratings yet
- Physical Assessment Final 1Document1 pagePhysical Assessment Final 1Shane ann BragaNo ratings yet
- Integumentary SystemDocument7 pagesIntegumentary Systemkuroko tetsuya100% (2)
- General Anatomy 1 With NotesDocument23 pagesGeneral Anatomy 1 With NotesCesar marquesesNo ratings yet
- Safari - Feb 21, 2024 at 11:49 AM 2Document1 pageSafari - Feb 21, 2024 at 11:49 AM 2syansyncNo ratings yet
- Reviewer Integumentary DigestiveDocument11 pagesReviewer Integumentary DigestiveMariah Alexa LibaoNo ratings yet
- (OB) 1.03 Maternal Physiology - Dr. QuilangDocument6 pages(OB) 1.03 Maternal Physiology - Dr. QuilangMarlon BauagNo ratings yet
- (OB) 1.02 Maternal Anatomy - Dr. DamasoDocument10 pages(OB) 1.02 Maternal Anatomy - Dr. DamasoMarlon BauagNo ratings yet
- Principles of Agglutination ReactionsDocument5 pagesPrinciples of Agglutination ReactionsMarlon BauagNo ratings yet
- Serological Test On Bacterial Infections-Streptococcal InfectionDocument5 pagesSerological Test On Bacterial Infections-Streptococcal InfectionMarlon BauagNo ratings yet
- Principles of Precipitation ReactionsDocument6 pagesPrinciples of Precipitation ReactionsMarlon BauagNo ratings yet
- Blood Flukes: Schistosomiasis JaponicaDocument6 pagesBlood Flukes: Schistosomiasis JaponicaMarlon BauagNo ratings yet
- Lung Fluke Disease: ParagonimiasisDocument4 pagesLung Fluke Disease: ParagonimiasisMarlon BauagNo ratings yet
- Principles of Precipitation Reactions-Part 2Document3 pagesPrinciples of Precipitation Reactions-Part 2Marlon BauagNo ratings yet
- (Pcol) 5.01 Chemotherapeutic DrugsDocument10 pages(Pcol) 5.01 Chemotherapeutic DrugsMarlon BauagNo ratings yet
- (PARA) 2.04 - Intestinal Flukes - Dr. AlvaradoDocument4 pages(PARA) 2.04 - Intestinal Flukes - Dr. AlvaradoMarlon BauagNo ratings yet
- (Pcol) Cancer ChemotherapyDocument23 pages(Pcol) Cancer ChemotherapyMarlon BauagNo ratings yet
- Basal Ganglia and Telencephalon AnatomyDocument11 pagesBasal Ganglia and Telencephalon AnatomyMarlon BauagNo ratings yet
- (PARA) 2.06 - Liver Flukes - Dr. AlvaradoDocument7 pages(PARA) 2.06 - Liver Flukes - Dr. AlvaradoMarlon BauagNo ratings yet
- Neuro 3.06 Neurologic Exam DR - CalimagDocument16 pagesNeuro 3.06 Neurologic Exam DR - CalimagMarlon BauagNo ratings yet
- NEURO 3.04 ANSLimbic System HypothalamusDocument10 pagesNEURO 3.04 ANSLimbic System HypothalamusMarlon BauagNo ratings yet
- How to Get a High Score on the OET Writing Sub-TestDocument6 pagesHow to Get a High Score on the OET Writing Sub-TestRosselini EspinedaNo ratings yet
- Klinik Utama Ilona Daftar ItemDocument12 pagesKlinik Utama Ilona Daftar ItemListia NingsihNo ratings yet
- Chapter IV - Dermatology: Common Skin Procedures BiopsyDocument6 pagesChapter IV - Dermatology: Common Skin Procedures BiopsyIndranil SinhaNo ratings yet
- No Product Name Qty: Berita Acara Uji FungsiDocument7 pagesNo Product Name Qty: Berita Acara Uji FungsiAditya-Oza PNo ratings yet
- Surgical Pathology of the Skin: Diseases and DisordersDocument11 pagesSurgical Pathology of the Skin: Diseases and DisordersPipoy Amy100% (1)
- Ask A Dermatologist Online For FreeDocument1 pageAsk A Dermatologist Online For FreeVispera HealthNo ratings yet
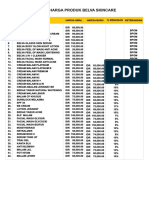
- Belva Skincare Product Prices ListDocument1 pageBelva Skincare Product Prices Listmas adiNo ratings yet
- qt5xd8t1t3 NosplashDocument3 pagesqt5xd8t1t3 NosplashDeb halderNo ratings yet
- Photographic Illustrations of Skin DiseasesDocument316 pagesPhotographic Illustrations of Skin DiseasessfranchiniNo ratings yet
- 10 Effective Homeopathic Medicines For Pityriasis Alba - DrHomeoDocument4 pages10 Effective Homeopathic Medicines For Pityriasis Alba - DrHomeoGer DersenNo ratings yet
- Rash Diagnosis Cheat Sheet: EmergencyDocument1 pageRash Diagnosis Cheat Sheet: Emergencykdlsfk kajjksolsNo ratings yet
- Fungal Skin Infections-1Document27 pagesFungal Skin Infections-1Fabb Nelson100% (1)
- Sunscreen PresentationDocument10 pagesSunscreen PresentationNurin Insyirah ShafieeNo ratings yet
- Disorders of Hair FollicleDocument41 pagesDisorders of Hair Folliclerejuven100% (2)
- Hair RemovalDocument28 pagesHair RemovalMARIALUPE ESTOQUENo ratings yet
- 15 Amazing Benefits of Beeswax for Skin HealthDocument8 pages15 Amazing Benefits of Beeswax for Skin HealthInspire NationsNo ratings yet
- Understanding Burn DegreesDocument2 pagesUnderstanding Burn DegreesAnu TripathiNo ratings yet
- Fitzpatricks Dermatology 9th Edition 3121Document1 pageFitzpatricks Dermatology 9th Edition 3121DennisSujayaNo ratings yet
- Doctor LLLLL 4Document54 pagesDoctor LLLLL 4loveNo ratings yet
- Daftar Harga CV FaeysaDocument4 pagesDaftar Harga CV FaeysaMo Kas Ku GarageNo ratings yet
- Skin Cancer Types, Risk Factors, Diagnosis & TreatmentDocument53 pagesSkin Cancer Types, Risk Factors, Diagnosis & TreatmentMohammadSAL-RawashdehNo ratings yet
- Heat Rash Prickly Heat Customer Version V2Document4 pagesHeat Rash Prickly Heat Customer Version V2Fitri 1997No ratings yet
- Nimisha Parekh's Narayani Remedies ExcerptDocument3 pagesNimisha Parekh's Narayani Remedies ExcerptFaomix de la House0% (1)
- Rosacea Fulminans Triggered by High-Dose Vitamins B6 and B12Document2 pagesRosacea Fulminans Triggered by High-Dose Vitamins B6 and B12PlantBasedNutritionNo ratings yet
- Dermatology 2010 2011Document28 pagesDermatology 2010 2011Qasim HaleimiNo ratings yet
- Treatment of PsoriasisDocument2 pagesTreatment of PsoriasisB.R SinghNo ratings yet
- Dermoscopy Guide Skin Cancer Non-MelanomaDocument63 pagesDermoscopy Guide Skin Cancer Non-MelanomaZain ButtNo ratings yet
- PL Jastiper MSBB JXB (Excel)Document3 pagesPL Jastiper MSBB JXB (Excel)Milou BeatriceNo ratings yet
- Pityriasis AlbaDocument6 pagesPityriasis AlbaLee Eng SiangNo ratings yet
- GROUP 2 Turmeric Facial SoapDocument3 pagesGROUP 2 Turmeric Facial SoapG20 Sumibcay FionaNo ratings yet