You might also like
- Modern Physics - G. Aruldhas and P. RajagopalDocument88 pagesModern Physics - G. Aruldhas and P. RajagopalKoushik ThummalaNo ratings yet
- Derivation TreesDocument16 pagesDerivation TreesAnithaChristopher100% (2)
- Reinforced Concrete Design 9th Edition PDF - Google SearchDocument2 pagesReinforced Concrete Design 9th Edition PDF - Google Searchgodofredo dumaliNo ratings yet
- Prezentare ClujDocument64 pagesPrezentare ClujAndreea IrimiaNo ratings yet
- Importance of RDW Value in Differential Diagnosis of Hypochrome AnemiasDocument3 pagesImportance of RDW Value in Differential Diagnosis of Hypochrome AnemiasArisa RosyadaNo ratings yet
- Clinical Significance Blood Group AntibodiesDocument8 pagesClinical Significance Blood Group AntibodiesSudeep RathoreNo ratings yet
- Variant Analysis of COVID-19 GenomesDocument20 pagesVariant Analysis of COVID-19 GenomesBiologia CaseiraNo ratings yet
- CCO 2014 AASLD Satellite DownloadableDocument43 pagesCCO 2014 AASLD Satellite DownloadableAnonymous dkH3NSvhvANo ratings yet
- Genetic Association Between IL-21 Polymorphisms and Cryptorchidism in A Chinese Han PopulationDocument4 pagesGenetic Association Between IL-21 Polymorphisms and Cryptorchidism in A Chinese Han PopulationHugo AlvesNo ratings yet
- Hepatitis B Case StudiesDocument26 pagesHepatitis B Case StudieswqmxmNo ratings yet
- 1 - Hodgkin's LymphomaDocument12 pages1 - Hodgkin's LymphomaDiana MitreaNo ratings yet
- Association Between HLA-B 15Document3 pagesAssociation Between HLA-B 15hoshikoongNo ratings yet
- Cco Aids 2012 SlidesDocument57 pagesCco Aids 2012 SlidesArpon FilesNo ratings yet
- Mchugh 1989Document2 pagesMchugh 1989Araceli Enríquez OvandoNo ratings yet
- CCO AU 2016 HCV Plenary 1 SlidesDocument39 pagesCCO AU 2016 HCV Plenary 1 SlideshziglamNo ratings yet
- Debate On Nucs Vs INF Singapore 2014Document16 pagesDebate On Nucs Vs INF Singapore 2014Robert G. Gish, MDNo ratings yet
- Q#1: What Do Understand by Term Classification and Tabulation - Discuss Its Importance in Health Sciences?Document15 pagesQ#1: What Do Understand by Term Classification and Tabulation - Discuss Its Importance in Health Sciences?haddi awanNo ratings yet
- LFTsDocument16 pagesLFTsMuhammad AleemNo ratings yet
- HLA Class I Markers in Japanese Patients With Carbamazepine-Induced Cutaneous Adverse ReactionsDocument4 pagesHLA Class I Markers in Japanese Patients With Carbamazepine-Induced Cutaneous Adverse ReactionsGading AuroraNo ratings yet
- J Bir 2020 10 006Document5 pagesJ Bir 2020 10 006wiam zaimiNo ratings yet
- HepatitisDocument14 pagesHepatitismuvin236No ratings yet
- Supplemental Information The Neuronal Repellent SLIT2 Is A Target For Repression by EZH2 in Prostate CancerDocument11 pagesSupplemental Information The Neuronal Repellent SLIT2 Is A Target For Repression by EZH2 in Prostate Cancermicrobotica126No ratings yet
- Research ArticleDocument7 pagesResearch ArticlentnquynhproNo ratings yet
- Paediatric AML Guidance Dec 2015Document33 pagesPaediatric AML Guidance Dec 2015Genetic Clinic UKMNo ratings yet
- If HP Cancer Guide BMT ManualDocument363 pagesIf HP Cancer Guide BMT ManualZardar KNo ratings yet
- Antibody Response To Mrna Sars-Cov-2 Vaccine Among Dialysis Patients-A Prospective Cohort StudyDocument3 pagesAntibody Response To Mrna Sars-Cov-2 Vaccine Among Dialysis Patients-A Prospective Cohort StudyBala MuraliNo ratings yet
- Aslan Et Al-2002-American Journal of HematologyDocument3 pagesAslan Et Al-2002-American Journal of HematologymwaNo ratings yet
- NIHMS13776 Supplement SuppDocument7 pagesNIHMS13776 Supplement Suppmaxence tricaudNo ratings yet
- SupplementDocument9 pagesSupplementMohamed SayedNo ratings yet
- A 19 Year Old With Fever, Rash, and Conjunctivitis: A Connection With The HeartDocument3 pagesA 19 Year Old With Fever, Rash, and Conjunctivitis: A Connection With The HeartLeberina TunjNo ratings yet
- Abvd Plus Rituximab en LH Clasica AvnzadoDocument3 pagesAbvd Plus Rituximab en LH Clasica AvnzadoErikadelCorralNo ratings yet
- Kubsa Guyo Advance BiostatisticDocument30 pagesKubsa Guyo Advance BiostatistickubsaNo ratings yet
- Klasifikasi CTCLDocument12 pagesKlasifikasi CTCLPramita SariNo ratings yet
- ALpatientsCLABSIrisk Fev2018Document7 pagesALpatientsCLABSIrisk Fev2018intan elokNo ratings yet
- 8 - Ap 170219 0493Document8 pages8 - Ap 170219 0493hoshikoongNo ratings yet
- Atributos e Preditores Da COVID-19 de Longa Duração.Document17 pagesAtributos e Preditores Da COVID-19 de Longa Duração.Rízia SouzaNo ratings yet
- ASH Hematology Review Series - Hodgkin Lymphoma - HerreraDocument69 pagesASH Hematology Review Series - Hodgkin Lymphoma - HerreraИван НегарэNo ratings yet
- Discussion: Calculations For Combined PhenotypesDocument16 pagesDiscussion: Calculations For Combined PhenotypesPurple basketNo ratings yet
- DR - Vandana. Dept of Microbiology KMC, Manipal.: Asst ProfessorDocument72 pagesDR - Vandana. Dept of Microbiology KMC, Manipal.: Asst ProfessorAnupama NagrajNo ratings yet
- HLA Genotype and Carbamazepine-Induced Cutaneous Adverse Drug Reactions - A Systematic ReviewDocument9 pagesHLA Genotype and Carbamazepine-Induced Cutaneous Adverse Drug Reactions - A Systematic ReviewGading AuroraNo ratings yet
- 1 s2.0 S0003269722003918 MainDocument8 pages1 s2.0 S0003269722003918 MainPeem PrinNo ratings yet
- CASTLE SubanalysisDocument4 pagesCASTLE SubanalysisIsmaelJoséGonzálezGuzmánNo ratings yet
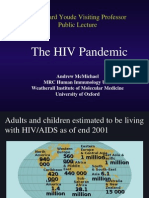
- The HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureDocument50 pagesThe HIV Pandemic: Sir Edward Youde Visiting Professor Public LectureSanthosh SubramanianNo ratings yet
- Impact DAA On Glycemic ControlDocument7 pagesImpact DAA On Glycemic ControlNi Nyoman Indirawati KusumaNo ratings yet
- (03241750 - Acta Medica Bulgarica) HLA DRB1 and HLA DQB1 Alleles in Bulgarian Patients With Primary and Secondary Antiphospholipid SyndromeDocument6 pages(03241750 - Acta Medica Bulgarica) HLA DRB1 and HLA DQB1 Alleles in Bulgarian Patients With Primary and Secondary Antiphospholipid SyndromeTeodorNo ratings yet
- Challenges in Managing Hepatitis C Virus InfectionDocument57 pagesChallenges in Managing Hepatitis C Virus InfectionAhmed ElwassiefNo ratings yet
- Clinical Characteristics of Patients With Dizziness After Motor Vehicle AccidentDocument5 pagesClinical Characteristics of Patients With Dizziness After Motor Vehicle AccidentrosaNo ratings yet
- Basics of TB, TBDocument24 pagesBasics of TB, TBzinabu tesfayeNo ratings yet
- Conference PresentationDocument19 pagesConference PresentationJamil Muqtadir BhattiNo ratings yet
- Predictive Value of IL-28B rs12979860 Variants For peg-IFN, Sofosbuvir Plus Ribavirin Treatment of HCV Infection in Pakistani PopulationDocument8 pagesPredictive Value of IL-28B rs12979860 Variants For peg-IFN, Sofosbuvir Plus Ribavirin Treatment of HCV Infection in Pakistani PopulationThanh PhongNo ratings yet
- Case ReportDocument25 pagesCase ReportFadhilah Amirah NasutionNo ratings yet
- Makcos1994 PDFDocument4 pagesMakcos1994 PDFAraceli EnríquezNo ratings yet
- 11168-Article Text-81547-2-10-20231227Document12 pages11168-Article Text-81547-2-10-20231227ppdsipd2019No ratings yet
- Human Genetic Variant E756del in The Ion Channel PDocument3 pagesHuman Genetic Variant E756del in The Ion Channel PDominic AmuzuNo ratings yet
- Hematologic Parameters in Patients With COVID-19 InfectionDocument4 pagesHematologic Parameters in Patients With COVID-19 InfectionLuisa María EstrellaNo ratings yet
- HCV Genotype ThesisDocument4 pagesHCV Genotype Thesistonyacartererie100% (2)
- HLA No B 27Document7 pagesHLA No B 27Ali ChaconNo ratings yet
- EBCR Hepatologi - Edel Herbitya 1706098814Document34 pagesEBCR Hepatologi - Edel Herbitya 1706098814Fita FitriantiNo ratings yet
- Aian 22 377Document11 pagesAian 22 377hoshikoongNo ratings yet
- RDW - SD, CVDocument8 pagesRDW - SD, CValimalekiNo ratings yet
- Results of Cancer Treatment at DarfDocument4 pagesResults of Cancer Treatment at DarfWashington AmericaNo ratings yet
- PatientconferenceM Adadkmnguyen HBV Treatment 06Document100 pagesPatientconferenceM Adadkmnguyen HBV Treatment 06Sakeer PeringodanNo ratings yet
- Hydrolysis and Fermentation of Sweetpotatoes For Production of Fermentable Sugars and EthanolDocument11 pagesHydrolysis and Fermentation of Sweetpotatoes For Production of Fermentable Sugars and Ethanolkelly betancurNo ratings yet
- Outstandingacademicachievementawardtill 2021 Ver 0723Document15 pagesOutstandingacademicachievementawardtill 2021 Ver 0723A DNo ratings yet
- Zforce Touch FINAL REPORTDocument20 pagesZforce Touch FINAL REPORTSWAPNILJUMALE75% (4)
- Une en Iso 898-7 TorqueDocument7 pagesUne en Iso 898-7 TorqueMiguel QueirosNo ratings yet
- Electricity MCQ'SDocument131 pagesElectricity MCQ'SSalik SalikNo ratings yet
- Embedded Design Engineer: Mrs - Vidyasagar Ashok GaikwadDocument2 pagesEmbedded Design Engineer: Mrs - Vidyasagar Ashok GaikwadandrueNo ratings yet
- Match The Opening Greeting With The Most Suitable CloseDocument4 pagesMatch The Opening Greeting With The Most Suitable Closealif afdilahNo ratings yet
- Miq Eng 18.07.2022Document8 pagesMiq Eng 18.07.2022VafaNo ratings yet
- List of Power Stations in India - Wikipedia, The Free EncyclopediaDocument19 pagesList of Power Stations in India - Wikipedia, The Free EncyclopediaRihlesh Parl0% (1)
- Lucas Graceful Labeling For Some GraphsDocument19 pagesLucas Graceful Labeling For Some GraphsDon HassNo ratings yet
- Macmillan English 1 Unit 18 Worksheet Teaching Notes: 3 MarksDocument2 pagesMacmillan English 1 Unit 18 Worksheet Teaching Notes: 3 MarksFlorea MonicaNo ratings yet
- Day 2 - Tension and Compression Member PDFDocument40 pagesDay 2 - Tension and Compression Member PDFSann MyintmgNo ratings yet
- Vector AnalysisDocument24 pagesVector AnalysisHoàng Nguyễn ĐìnhNo ratings yet
- Tu Dien Oto PDFDocument400 pagesTu Dien Oto PDFVương HoàngNo ratings yet
- EE 321: Communication Systems I: L1 - IntroductionDocument28 pagesEE 321: Communication Systems I: L1 - IntroductionFengxing ZhuNo ratings yet
- 793D SERV1817-01 - SLIDE - Aug2006Document233 pages793D SERV1817-01 - SLIDE - Aug2006Ishan IqbalNo ratings yet
- ## JSA - 008 - Hydraulic Rig and Mobile Crane MarchingDocument1 page## JSA - 008 - Hydraulic Rig and Mobile Crane MarchingAbhijit JanaNo ratings yet
- Es 14Document394 pagesEs 14carlodolciNo ratings yet
- Redx LogisticsDocument29 pagesRedx Logisticsbabu chyNo ratings yet
- Assignment#1Document2 pagesAssignment#1ramNo ratings yet
- App-005 Practical Research 111Document7 pagesApp-005 Practical Research 111Armhay Loraine DuavezNo ratings yet
- CMINDS AdmissionTest - SYLLABUS Apr22Document4 pagesCMINDS AdmissionTest - SYLLABUS Apr22Soham DattaNo ratings yet
- Current IssuesDocument21 pagesCurrent IssuesJFS100% (4)
- Sumedha - Final Audio Assignment - Written ComponentDocument3 pagesSumedha - Final Audio Assignment - Written Componentsumedhagupta.sias22No ratings yet
- 22BEE13Document4 pages22BEE13New GenieNo ratings yet
- I3 MEGA Quick GuideDocument1 pageI3 MEGA Quick GuideJuan Manuel TalaveraNo ratings yet
- Syllabus Cet 362Document8 pagesSyllabus Cet 362dipinnediyaparambathNo ratings yet