You might also like
- Manifesting Your Best Future Self: Building Adaptive ResilienceFrom EverandManifesting Your Best Future Self: Building Adaptive ResilienceNo ratings yet
- Fundamentals in Nursing Lesson #1 INTRODUCTORY CONCEPTSDocument6 pagesFundamentals in Nursing Lesson #1 INTRODUCTORY CONCEPTSSophia Duquinlay100% (1)
- Health and IllnessDocument71 pagesHealth and IllnessLondho Londho100% (2)
- FUNDA_LESSON1_HEALTH_AND_WELLNESSDocument5 pagesFUNDA_LESSON1_HEALTH_AND_WELLNESSAzTech 233No ratings yet
- Health, Wellness, and Illness What Is Health? What Is A Chronic Disease?Document5 pagesHealth, Wellness, and Illness What Is Health? What Is A Chronic Disease?Tintin EstNo ratings yet
- Reviewer Funda LecDocument71 pagesReviewer Funda LecCorillo, Fionnula JeanNo ratings yet
- FUNDAMENTALS OF NURSING PRACTICE - PrelimsDocument10 pagesFUNDAMENTALS OF NURSING PRACTICE - PrelimsGeorgia LanuzoNo ratings yet
- Concepts of Nursing Handout 3Document11 pagesConcepts of Nursing Handout 3harutochoky8No ratings yet
- Funda Lesson1 Health and WellnessDocument4 pagesFunda Lesson1 Health and WellnessSymon AmoguisNo ratings yet
- Funda Lesson1 Health and WellnessDocument4 pagesFunda Lesson1 Health and WellnessRovic GasmenNo ratings yet
- Concepts of Nursing HandoutDocument8 pagesConcepts of Nursing Handouts.orpilla.aaroncristianNo ratings yet
- Health & WellbeingDocument29 pagesHealth & WellbeingTrinadia Utami100% (1)
- FUNDAMENTALS OF NURSING 1Document15 pagesFUNDAMENTALS OF NURSING 1Carla NicoleNo ratings yet
- Concepts of Health, Illness and Wellness DefinedDocument6 pagesConcepts of Health, Illness and Wellness DefinedKhream Harvie OcampoNo ratings yet
- Mental Health and Wellness 2021Document8 pagesMental Health and Wellness 2021Nimesh KaushikNo ratings yet
- 2 - Theory of Health PromotionDocument38 pages2 - Theory of Health PromotionDaniel Anthony CabreraNo ratings yet
- BSNS6 - Key Nursing Theorists and ConceptsDocument5 pagesBSNS6 - Key Nursing Theorists and ConceptsLegendXNo ratings yet
- Ch. 1Document31 pagesCh. 1KikiNo ratings yet
- NSTPDocument3 pagesNSTPCyruz GinesNo ratings yet
- NCM 102 - Concepts of IllnessDocument68 pagesNCM 102 - Concepts of Illnessyen1988No ratings yet
- P.E 11 NotesDocument7 pagesP.E 11 NotesAmylyn CaliguiaNo ratings yet
- Concepts of Health, Wellness, and Well-BeingDocument15 pagesConcepts of Health, Wellness, and Well-BeingEarl BenedictNo ratings yet
- 1 HEALTH AND ILLNESS HandoutsDocument5 pages1 HEALTH AND ILLNESS HandoutsVanessa Mae IlaganNo ratings yet
- 1 Introduction To Mental Health and Psychiatric NursingDocument6 pages1 Introduction To Mental Health and Psychiatric NursingRose Lyn Camarista VelascoNo ratings yet
- LECTURE 2 - Concepts of Health,.ppt 2Document80 pagesLECTURE 2 - Concepts of Health,.ppt 2NIKITA NOVENO100% (2)
- Healt Social Well-Mental/ Emotional: Betty NeumannDocument21 pagesHealt Social Well-Mental/ Emotional: Betty NeumannTine GuibaoNo ratings yet
- Models of Health and WellnesDocument5 pagesModels of Health and WellnesBlaise Anne InocNo ratings yet
- Konsep Sehat dan Sakit: Homeostasis, Determinan Kesehatan, dan Model Sehat-SakitDocument28 pagesKonsep Sehat dan Sakit: Homeostasis, Determinan Kesehatan, dan Model Sehat-SakitWill HensNo ratings yet
- Concepts of Man Health and IllnessDocument48 pagesConcepts of Man Health and IllnessMartD Recalde100% (5)
- Fundamentals of Nursing Lec Lesson 1Document7 pagesFundamentals of Nursing Lec Lesson 1Zen Gesner Kenneth G. EganaNo ratings yet
- Five Areas of Personal DevelopmentDocument2 pagesFive Areas of Personal DevelopmentKristine Joy Reyes100% (1)
- FUNDADocument9 pagesFUNDAAlexsa AranteNo ratings yet
- 1 - BasicsofWellness - HandoutsDocument71 pages1 - BasicsofWellness - HandoutsKyle OrtegaNo ratings yet
- Hoang Vy Nguyen - Week 1&2 - Better Health For Individuals - (Student Booklet)Document27 pagesHoang Vy Nguyen - Week 1&2 - Better Health For Individuals - (Student Booklet)klee71353No ratings yet
- Chapter 1-Concept of Health & IllnessDocument117 pagesChapter 1-Concept of Health & IllnessJAHERA NACO100% (1)
- NUR 221 Chapter 17 Health, Wellness, and IllnessDocument5 pagesNUR 221 Chapter 17 Health, Wellness, and IllnessJonathan Aguirre P.No ratings yet
- Fundamentals of nursing practice lecture reviewerDocument5 pagesFundamentals of nursing practice lecture reviewerAebee AlcarazNo ratings yet
- Health Information System Prelim GuideDocument2 pagesHealth Information System Prelim GuideMica CapistranoNo ratings yet
- Man's Basic Needs as a Biopsychosocial and Spiritual BeingDocument5 pagesMan's Basic Needs as a Biopsychosocial and Spiritual BeingNina Anne Paracad100% (1)
- Unit VII Mental Health and Mental HealthDocument13 pagesUnit VII Mental Health and Mental HealthOmprakash Swami89% (9)
- Dlstudocu.com Concept of Man Health and IllnessDocument4 pagesDlstudocu.com Concept of Man Health and IllnessHurricane AlvarezNo ratings yet
- FNP Act.1 - Group 9 BDocument8 pagesFNP Act.1 - Group 9 BQuiane IcaNo ratings yet
- Konsep Sehat & Sakit: Rosyidah ArafatDocument15 pagesKonsep Sehat & Sakit: Rosyidah ArafatUni AyatiNo ratings yet
- Health and WellnessDocument19 pagesHealth and WellnessChatie PipitNo ratings yet
- ADR - Concept of Man, Health and Illness - StudentDocument52 pagesADR - Concept of Man, Health and Illness - StudentRaRe TV100% (1)
- Unit VII Mental Health and Mental HealthDocument12 pagesUnit VII Mental Health and Mental HealthOmprakash Swami100% (1)
- Lifestyle Medicine: Lifestyle Medicine Focuses On 6 Areas To Improve HealthDocument2 pagesLifestyle Medicine: Lifestyle Medicine Focuses On 6 Areas To Improve HealthYan Camilo Vergara GalloNo ratings yet
- Concept of ManDocument4 pagesConcept of ManAllanah Beatriz TubalNo ratings yet
- Presented by Babita Dhrue Ankita Panigrahi MSC Nursing Previous YearDocument15 pagesPresented by Babita Dhrue Ankita Panigrahi MSC Nursing Previous YearBabita DhruwNo ratings yet
- SocialWorkerPowerPointCO-OP PresentationDocument13 pagesSocialWorkerPowerPointCO-OP PresentationAngela Blanco-RamosNo ratings yet
- Core 1 - Better Health For IndividualsDocument19 pagesCore 1 - Better Health For IndividualsJasnoor MatharuNo ratings yet
- Models of PreventionDocument25 pagesModels of PreventionAMY LALRINGHLUANI M.Sc. Child Health (Paediatric ) NursingNo ratings yet
- Needs and Wellness ModelsDocument8 pagesNeeds and Wellness ModelsMing100% (1)
- Psychiatric NursingDocument10 pagesPsychiatric NursingmendozaayajulienneNo ratings yet
- Divine Word College of Legazpi College of Nursing: Franco L. Razon, Man, RNDocument91 pagesDivine Word College of Legazpi College of Nursing: Franco L. Razon, Man, RNFranco Razon100% (1)
- A Wellness Approach: Psychiatric Rehabilitation Journal February 2006Document5 pagesA Wellness Approach: Psychiatric Rehabilitation Journal February 2006ChristianJayValdezNo ratings yet
- Curriculum Map G7 HealthDocument60 pagesCurriculum Map G7 HealthsweetymerzsuarinNo ratings yet
- How Individuals Perceive and Are Influenced by HealthDocument8 pagesHow Individuals Perceive and Are Influenced by HealthJessica GannonNo ratings yet
- Concepts of Health, Wellness and Dimensions of Well-BeingDocument4 pagesConcepts of Health, Wellness and Dimensions of Well-BeingEthel May AlabastroNo ratings yet
- Physical Education and Health 12Document2 pagesPhysical Education and Health 12Jenia Alexis CapaNo ratings yet
- 2013 KTM 350 EXC Shop-Repair ManualDocument310 pages2013 KTM 350 EXC Shop-Repair ManualTre100% (7)
- Water As A Weapon - Israel National NewsDocument11 pagesWater As A Weapon - Israel National NewsJorge Yitzhak Pachas0% (1)
- Fishblade RPGDocument1 pageFishblade RPGthe_doom_dudeNo ratings yet
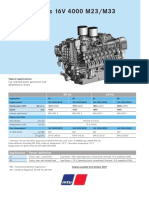
- Diesel Engines 16V 4000 M23/M33: 50 HZ 60 HZDocument2 pagesDiesel Engines 16V 4000 M23/M33: 50 HZ 60 HZAlberto100% (1)
- SoalDocument4 pagesSoalkurikulum man2wonosoboNo ratings yet
- Review of Esu Yoruba God Power and The IDocument7 pagesReview of Esu Yoruba God Power and The IBoris MilovicNo ratings yet
- Australian Securities and Investments Commission V KingDocument47 pagesAustralian Securities and Investments Commission V KingCourtni HolderNo ratings yet
- Kepler's ProblemDocument21 pagesKepler's ProblemGustavo MiasatoNo ratings yet
- Performance Theory For Hot Air Balloons: The Balloon Works, Inc., Statesville, N.CDocument4 pagesPerformance Theory For Hot Air Balloons: The Balloon Works, Inc., Statesville, N.CEbubekir ErkanNo ratings yet
- Common Expressions in Business 2Document2 pagesCommon Expressions in Business 2abdeljelil manelNo ratings yet
- Processing, Handling and Storage of Agricultural Product 2Document6 pagesProcessing, Handling and Storage of Agricultural Product 2LittleagleNo ratings yet
- Reported SpeechDocument2 pagesReported SpeechlacasabaNo ratings yet
- Harsheen Kaur BhasinDocument20 pagesHarsheen Kaur Bhasincalvin kleinNo ratings yet
- Chimdesa J. Functional FoodsDocument201 pagesChimdesa J. Functional FoodsChimdesa100% (1)
- 1868 Sop Work at HeightDocument10 pages1868 Sop Work at HeightAbid AzizNo ratings yet
- Impacts of Gmos On Golden RiceDocument3 pagesImpacts of Gmos On Golden RiceDianna Rose Villar LaxamanaNo ratings yet
- CV HannahDocument3 pagesCV HannahRoxan DosdosNo ratings yet
- How to Launder Money in Real EstateDocument58 pagesHow to Launder Money in Real EstateSpeedyGonsalesNo ratings yet
- Are The Risk Management Tools at Your Law Firm Working?Document17 pagesAre The Risk Management Tools at Your Law Firm Working?vantoffNo ratings yet
- How to Stop Overthinking and Make DecisionsDocument39 pagesHow to Stop Overthinking and Make DecisionsDeepak SinghNo ratings yet
- MSc Thesis on VAW in PhilippinesDocument100 pagesMSc Thesis on VAW in Philippineselma cutamoraNo ratings yet
- SDM - Session 6Document21 pagesSDM - Session 6Rohith NairNo ratings yet
- NCP GeriaDocument6 pagesNCP GeriaKeanu ArcillaNo ratings yet
- Skills Test Unit 1 Test A EmailDocument4 pagesSkills Test Unit 1 Test A EmailЛиза ОмельченкоNo ratings yet
- BIODATADocument1 pageBIODATAzspi rotc unitNo ratings yet
- Types of Motivation in Language LearningDocument8 pagesTypes of Motivation in Language LearningAlya IrmasyahNo ratings yet
- Landman Training ManualDocument34 pagesLandman Training Manualflashanon100% (2)
- Lead and Manage Team Effectiveness for BSBWOR502Document38 pagesLead and Manage Team Effectiveness for BSBWOR502roopaNo ratings yet
- Nursing Process & Patient Care ModalitiesDocument6 pagesNursing Process & Patient Care ModalitiesNur SanaaniNo ratings yet
- RetailMarketinginIndia 1Document158 pagesRetailMarketinginIndia 1RamanNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Insecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItFrom EverandInsecure in Love: How Anxious Attachment Can Make You Feel Jealous, Needy, and Worried and What You Can Do About ItRating: 4.5 out of 5 stars4.5/5 (84)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)
- Winning the War in Your Mind: Change Your Thinking, Change Your LifeFrom EverandWinning the War in Your Mind: Change Your Thinking, Change Your LifeRating: 5 out of 5 stars5/5 (558)
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- Smart Phone Dumb Phone: Free Yourself from Digital AddictionFrom EverandSmart Phone Dumb Phone: Free Yourself from Digital AddictionRating: 5 out of 5 stars5/5 (11)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Fighting Words Devotional: 100 Days of Speaking Truth into the DarknessFrom EverandFighting Words Devotional: 100 Days of Speaking Truth into the DarknessRating: 5 out of 5 stars5/5 (6)
- Are You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersFrom EverandAre You Really OK?: Getting Real About Who You Are, How You’re Doing, and Why It MattersRating: 5 out of 5 stars5/5 (28)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1243)