You might also like
- New Guide To Rational Living Albert EllisDocument131 pagesNew Guide To Rational Living Albert EllisPsuja89100% (9)
- The Cult of The Moon GodDocument15 pagesThe Cult of The Moon GodJesus LivesNo ratings yet
- Parrino 2e PowerPoint Review Ch13Document55 pagesParrino 2e PowerPoint Review Ch13Khadija AlkebsiNo ratings yet
- Shock: Dr. Bambang Priyanto SpanDocument67 pagesShock: Dr. Bambang Priyanto Spannunki aprillitaNo ratings yet
- 2b 10 Circ APRIL 2013-Diproteksi UnlockedDocument66 pages2b 10 Circ APRIL 2013-Diproteksi UnlockedMaulana Muhtadin SuryansyahNo ratings yet
- Drugs For Heart FailureDocument39 pagesDrugs For Heart FailureOngKahYeeNo ratings yet
- Foreward Failure: Cardiac OutputDocument1 pageForeward Failure: Cardiac Outputmaria ngongoNo ratings yet
- Cardiovascular SystemDocument20 pagesCardiovascular SystemFisco DessereiNo ratings yet
- Hemodinamik Dasar Invasive 2Document27 pagesHemodinamik Dasar Invasive 2Tkv UhamkaNo ratings yet
- Setting Up Emergency Medical Service: Intensive Course & WorkshopDocument41 pagesSetting Up Emergency Medical Service: Intensive Course & WorkshopOliver GiroudNo ratings yet
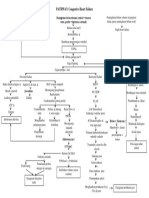
- Pa Tho Physiology of Congestive Heart FailureDocument3 pagesPa Tho Physiology of Congestive Heart FailureErin MarieNo ratings yet
- Multisystem ProblemsDocument90 pagesMultisystem ProblemsAlexander Blanche PajelaNo ratings yet
- Cardiac SystemDocument7 pagesCardiac Systemsccctutor100% (3)
- Cv-4 PHDocument28 pagesCv-4 PHaya najemNo ratings yet
- System and Disease III ComprehensiveDocument46 pagesSystem and Disease III Comprehensivenasr234No ratings yet
- Edema Dan PerdarahanDocument13 pagesEdema Dan PerdarahanKost Vila SakinahNo ratings yet
- Blood PressureDocument27 pagesBlood PressureSreedeep TejaNo ratings yet
- HypertensionDocument90 pagesHypertensionmybrainpower99999No ratings yet
- Circulație CoroarăDocument2 pagesCirculație CoroarăAurelia AlexandraNo ratings yet
- CardiologyslidesDocument1,035 pagesCardiologyslidescrilala23No ratings yet
- Heart Failure2Document39 pagesHeart Failure2Giselle Chloe Baluya icoNo ratings yet
- Primary Trauma Care: Sirkulasi C CirculationDocument36 pagesPrimary Trauma Care: Sirkulasi C CirculationAnisa RachmawatiNo ratings yet
- Cardiology 2: OutlineDocument5 pagesCardiology 2: Outlinevinnie0905No ratings yet
- Exam 1reference SheetDocument2 pagesExam 1reference SheetAndrea Norton100% (1)
- Heart FailureDocument42 pagesHeart FailureAdine Jeminah LimonNo ratings yet
- Pathway Gagal JantungDocument1 pagePathway Gagal Jantungmarlinapsik14No ratings yet
- ShockDocument30 pagesShockLập Trương Minh QuốcNo ratings yet
- Blood Pressure Regulation Hypertension AtfDocument4 pagesBlood Pressure Regulation Hypertension AtfMariaNo ratings yet
- 8 Venous ReturnDocument19 pages8 Venous ReturnDmNo ratings yet
- Mekanisme Dari Blood Pressure Regulation 1. Hemodynamic Factors (CO, TPR, Etc)Document9 pagesMekanisme Dari Blood Pressure Regulation 1. Hemodynamic Factors (CO, TPR, Etc)Caroline AgathaNo ratings yet
- 27 Cardio SpoDocument114 pages27 Cardio SpovinanoermayaniNo ratings yet
- Regulation of Blood Pressure - 2Document38 pagesRegulation of Blood Pressure - 2vikrant gholapNo ratings yet
- 14 Heart Cardio Edit NOquesDocument44 pages14 Heart Cardio Edit NOquesugjdk djfgNo ratings yet
- Cardiovascular SystemDocument11 pagesCardiovascular SystemJanet Floreno VillasanaNo ratings yet
- Cardiogenic Shock: DR Putra Hendra SPPD UnibaDocument30 pagesCardiogenic Shock: DR Putra Hendra SPPD UnibaDian PuspaNo ratings yet
- Blood PressureDocument64 pagesBlood PressureSrishti GoenkaNo ratings yet
- Inotropes and Vasopressors: Definition RecapDocument2 pagesInotropes and Vasopressors: Definition RecapThistell ThistleNo ratings yet
- Manajemen Cairan Pada Shock Hemoraghic & HipovolemikDocument57 pagesManajemen Cairan Pada Shock Hemoraghic & HipovolemikImron RosyadiNo ratings yet
- Hytension For 16 Years Men (64 Years Old) Cigarette Smoking (32 Pack Years) Alcoholic Drinker For 32 Years Fond of Eating Fatty Foods Physical Inability Sodium Intake HereditaryDocument3 pagesHytension For 16 Years Men (64 Years Old) Cigarette Smoking (32 Pack Years) Alcoholic Drinker For 32 Years Fond of Eating Fatty Foods Physical Inability Sodium Intake HereditaryJohn Paulo CatacutanNo ratings yet
- ShockDocument39 pagesShockCut Ristina OlviaNo ratings yet
- FA 2020 - Cardio Sterling Curve PDFDocument15 pagesFA 2020 - Cardio Sterling Curve PDFDrbee10No ratings yet
- Pemeriksaan Fisik KardiovaskularDocument46 pagesPemeriksaan Fisik KardiovaskularyuliaNo ratings yet
- Cardiac Output: Presented by N.Perumal Bot 4 TH YearDocument21 pagesCardiac Output: Presented by N.Perumal Bot 4 TH YearNithya SekarNo ratings yet
- CAD NCP Decreased Cardiac OutputDocument3 pagesCAD NCP Decreased Cardiac OutputLeizel Apolonio100% (3)
- CVS Drugs NewDocument46 pagesCVS Drugs NewreemonsantoNo ratings yet
- PhysiologyDocument10 pagesPhysiologyAmyrah MagajiNo ratings yet
- Cardio-Vascular ExaminationDocument43 pagesCardio-Vascular ExaminationDimas FrasesaNo ratings yet
- Shock: Agus Setiyana, M.D. Cardiac Anesthetist Acls Provider Fccs Provider Atls ProviderDocument39 pagesShock: Agus Setiyana, M.D. Cardiac Anesthetist Acls Provider Fccs Provider Atls ProvidersheiraNo ratings yet
- Cardio N41Document13 pagesCardio N41ashafernandesssNo ratings yet
- Principles of HemodynamicDocument48 pagesPrinciples of HemodynamicdevdsantoshNo ratings yet
- Coronary Circulation: Two Coronary Arteries (RT & LT) Arises From The Root of Aorta Supply Blood To MyocardiumDocument43 pagesCoronary Circulation: Two Coronary Arteries (RT & LT) Arises From The Root of Aorta Supply Blood To MyocardiumPhysiology by Dr RaghuveerNo ratings yet
- Crat - Cardio PulmoDocument11 pagesCrat - Cardio PulmoJULIANE MAE BALANGNo ratings yet
- Pharmacology: Cardiovascular SystemDocument314 pagesPharmacology: Cardiovascular SystemSharifa DarayanNo ratings yet
- Inadequate Reperfusion Therapy: Myocardial InfarctionDocument4 pagesInadequate Reperfusion Therapy: Myocardial InfarctionPäw YusophNo ratings yet
- CCC Nurs 235 - Pediatric & Maternity NursingFinal Study GuideDocument13 pagesCCC Nurs 235 - Pediatric & Maternity NursingFinal Study GuideHeidi HeffelfingerNo ratings yet
- Cardiac Output, Blood Flow, and Blood PressureDocument69 pagesCardiac Output, Blood Flow, and Blood PressureUzma KhanNo ratings yet
- Lecture Notes On CardiologyDocument31 pagesLecture Notes On CardiologyambiskuysNo ratings yet
- Cardiovascular System - Blood Vessels and CirculationDocument56 pagesCardiovascular System - Blood Vessels and CirculationJohn Carlo Cabueñas RagmaNo ratings yet
- Antianginal Drugs: Classes Therapeutic Uses MOA Adverse EffectsDocument3 pagesAntianginal Drugs: Classes Therapeutic Uses MOA Adverse EffectsNadhirah ZulkifliNo ratings yet
- MD-8 Regulation of Cardiovascular FunctionssDocument22 pagesMD-8 Regulation of Cardiovascular FunctionssvincenzoNo ratings yet
- CirculationDocument18 pagesCirculationasimm9hamedNo ratings yet
- Physio-DES-6 (Cardiac)Document56 pagesPhysio-DES-6 (Cardiac)Joseph Kim100% (1)
- Perfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationFrom EverandPerfusion for Congenital Heart Surgery: Notes on Cardiopulmonary Bypass for a Complex Patient PopulationRating: 5 out of 5 stars5/5 (2)
- Muhajir DiasporaDocument10 pagesMuhajir DiasporaneoindusNo ratings yet
- Martial Arts Jutekwon Ecuador PDFDocument34 pagesMartial Arts Jutekwon Ecuador PDFJHON FERNANDO ESPIN CUEVANo ratings yet
- Linguistic and Cultural Competence Will Be The Mark of The Well-Educated Citizen of The 21 CenturyDocument27 pagesLinguistic and Cultural Competence Will Be The Mark of The Well-Educated Citizen of The 21 CenturyJhay Mhar ANo ratings yet
- Classical PhilosophyDocument20 pagesClassical PhilosophyxogenNo ratings yet
- Fengshui in The BedroomDocument3 pagesFengshui in The BedroomJaralex SedlexNo ratings yet
- Dark PactDocument5 pagesDark PactSilvino González MoralesNo ratings yet
- Chapter 2Document99 pagesChapter 2Anish KumarNo ratings yet
- PENGARUH EKSTRAK DAUN KELOR (Moringa Oleifera L.) Terhadap Kualitas YoghurtDocument8 pagesPENGARUH EKSTRAK DAUN KELOR (Moringa Oleifera L.) Terhadap Kualitas YoghurtChaaNo ratings yet
- List of Laboratory ActivitiesDocument2 pagesList of Laboratory ActivitiesRuvy Jean Codilla-FerrerNo ratings yet
- DLL g6 q3 Week 5 All SubjectsDocument61 pagesDLL g6 q3 Week 5 All SubjectsRolando AtaNo ratings yet
- Project Example A1-1130H-1400W Air Handling Unit With PHE - (2.2m3/s) 2.20 m3/sDocument12 pagesProject Example A1-1130H-1400W Air Handling Unit With PHE - (2.2m3/s) 2.20 m3/samirin_king100% (1)
- Abhishek DubeyDocument89 pagesAbhishek DubeyVeekeshGuptaNo ratings yet
- A1a Introduction Defining GlobalizationDocument38 pagesA1a Introduction Defining GlobalizationMarco Tagun Laqueo0% (1)
- Heung 2012Document11 pagesHeung 2012Luis Jhonny Dávila ValderaNo ratings yet
- Emotion Regulation and Intellectual DisabilityDocument7 pagesEmotion Regulation and Intellectual DisabilityAntónio MartinsNo ratings yet
- MR Hiram BDocument3 pagesMR Hiram BPaul SegoviaNo ratings yet
- Voluntary Actions and Social MovementsDocument20 pagesVoluntary Actions and Social MovementsgmNo ratings yet
- Aniket Nagapure: Work Experience SkillsDocument1 pageAniket Nagapure: Work Experience Skillsaniket nagapureNo ratings yet
- 5 Compeitior 2021Document22 pages5 Compeitior 2021杜昕No ratings yet
- Evaluación Diagnóstica 4º InglésDocument9 pagesEvaluación Diagnóstica 4º InglésSharon Carola Ruiz GarciaNo ratings yet
- Dell EMC Unity: Unisphere OverviewDocument41 pagesDell EMC Unity: Unisphere OverviewJim SmithNo ratings yet
- 10 - The Farm Business SurveyDocument48 pages10 - The Farm Business SurveySeyha L. AgriFoodNo ratings yet
- Safe Back Exercises: The Extensors. Craig LiebensonDocument1 pageSafe Back Exercises: The Extensors. Craig LiebensonrojexeNo ratings yet
- Dornier DO 328 100 TDocument6 pagesDornier DO 328 100 TDANIEL ENRIQUE ALDANA LOPERANo ratings yet
- Monkayo East District Enrolment Report For The Month of SeptemberDocument3 pagesMonkayo East District Enrolment Report For The Month of SeptemberMary Ann AysonNo ratings yet
- Littlejohn v. Patrick B Harris Psychiatric Hospital - Document No. 12Document7 pagesLittlejohn v. Patrick B Harris Psychiatric Hospital - Document No. 12Justia.comNo ratings yet