You might also like
- Appex Corporation: Organizational Behaviour - Ii Group Case Write-Up 1Document6 pagesAppex Corporation: Organizational Behaviour - Ii Group Case Write-Up 1Pooja Yadav100% (1)
- Dark Side LeadershipDocument20 pagesDark Side Leadershipphanquipk100% (1)
- Labman - Transes PDFDocument7 pagesLabman - Transes PDFJasmine BunaoNo ratings yet
- PALMER (NLM) Enhancement Notes Nov 2020Document21 pagesPALMER (NLM) Enhancement Notes Nov 2020Basema HashhashNo ratings yet
- PPL Session 6Document25 pagesPPL Session 6thakranisparshNo ratings yet
- Laboratory Management MIDTERMSDocument4 pagesLaboratory Management MIDTERMSHera PrettyNo ratings yet
- FPI Ilaro - Managing For Results - 02102021 - UpdateDocument80 pagesFPI Ilaro - Managing For Results - 02102021 - UpdateKayode AdebiyiNo ratings yet
- Strategic Planning ADocument26 pagesStrategic Planning AmelissaNo ratings yet
- Ca2 Pre Lim NotesDocument39 pagesCa2 Pre Lim NotesDoll HwasaNo ratings yet
- A Research Based Assignment Mba-134 Understanding Business: Tulika Singh Registration Number 1927347 Mba DDocument5 pagesA Research Based Assignment Mba-134 Understanding Business: Tulika Singh Registration Number 1927347 Mba DTulika singhNo ratings yet
- Cia 1 Ub PDFDocument5 pagesCia 1 Ub PDFTULIKA SINGH 1927347No ratings yet
- Stratmg PDFDocument61 pagesStratmg PDFMARIELLE MANDACNo ratings yet
- BigstuL21LeadI New 2Document24 pagesBigstuL21LeadI New 2privynoble.05No ratings yet
- ABM083 MidDocument5 pagesABM083 Midespinoangel935No ratings yet
- SALM130 - CHPT 6Document46 pagesSALM130 - CHPT 6maphumulogwiriNo ratings yet
- Three Determinants of Behavior in An Organization: - Individuals - Groups - StructureDocument25 pagesThree Determinants of Behavior in An Organization: - Individuals - Groups - StructureHumayun ArshadNo ratings yet
- Leadership and ManagementDocument23 pagesLeadership and ManagementShimz kenNo ratings yet
- Life Cycle of An OrganizationDocument1 pageLife Cycle of An Organizationkelvin pogiNo ratings yet
- Executive Leadership and Physician Well-BeingDocument1 pageExecutive Leadership and Physician Well-BeingNatalia VillamizarNo ratings yet
- Getting More Effective: Branch Managers As ExecutivesDocument38 pagesGetting More Effective: Branch Managers As ExecutivesLubna SiddiqiNo ratings yet
- Nursing ProcessDocument23 pagesNursing Processjulesubayubay5428100% (6)
- Strategic Planning ModelDocument53 pagesStrategic Planning ModelSui Yuxuan100% (1)
- Lesson 11 - LeadershipDocument15 pagesLesson 11 - Leadershipram tibayNo ratings yet
- Module 1 Introduction To Leadership - FINALDocument32 pagesModule 1 Introduction To Leadership - FINALarbyjamesNo ratings yet
- IIAC-IMDS 2021 - 21st Century Economy and Business - Managing For Results - Final 240321 - 16.43Document90 pagesIIAC-IMDS 2021 - 21st Century Economy and Business - Managing For Results - Final 240321 - 16.43Kayode AdebiyiNo ratings yet
- Planning Functions & Pples of MgmtStudyNote6QUIZ IIDocument27 pagesPlanning Functions & Pples of MgmtStudyNote6QUIZ IIvenkataramanan_thiru100% (1)
- Health Management 2Document5 pagesHealth Management 2Carmela LadoresNo ratings yet
- Introduction Leadership and Management in NursingDocument32 pagesIntroduction Leadership and Management in NursingFida Mindia Farotama AmaliaNo ratings yet
- Unit StaffingDocument25 pagesUnit StaffingChetan PathakNo ratings yet
- Bullet SlidesDocument2 pagesBullet Slidesnitin21822No ratings yet
- Lec01 Lab-Management TransesDocument4 pagesLec01 Lab-Management TransesHANNAH N. RULIDANo ratings yet
- Rangkuman Chapter 19Document25 pagesRangkuman Chapter 19Fourenty KusumaNo ratings yet
- Leadership MBA.Document25 pagesLeadership MBA.AkshitaNo ratings yet
- BS4S19 Tutorial-Workshop 7Document30 pagesBS4S19 Tutorial-Workshop 7Chathurika KariyawasamNo ratings yet
- Managing People in Organization: Approaches To Leadership and Emotional Intelligence Stig ChristensenDocument28 pagesManaging People in Organization: Approaches To Leadership and Emotional Intelligence Stig ChristensenLe YM100% (1)
- PSF Leadership WorkshopDocument65 pagesPSF Leadership WorkshophakakNo ratings yet
- Human Resources& Job DesignDocument34 pagesHuman Resources& Job Designjohanna shaanyenengeNo ratings yet
- Leadership and ManagementDocument160 pagesLeadership and Management00060651No ratings yet
- Overview of Leadership: - Leadership Is Defined AsDocument32 pagesOverview of Leadership: - Leadership Is Defined Aswelcome2jungleNo ratings yet
- Lec 3 Leading Technical People PDFDocument44 pagesLec 3 Leading Technical People PDFAsad KhokharNo ratings yet
- What Is LeadershipDocument41 pagesWhat Is LeadershipFaraz Mansoor100% (2)
- 2023 M&C Collated Sessions Post Quiz 1Document35 pages2023 M&C Collated Sessions Post Quiz 1Siddharth PandeyNo ratings yet
- MGMT OB Leadership Lecture-2024 - Semester 2Document90 pagesMGMT OB Leadership Lecture-2024 - Semester 2ShareceNo ratings yet
- 1 Introduction To Management Copy 2Document21 pages1 Introduction To Management Copy 2Angelica Camille B. AbaoNo ratings yet
- HRM Session 1Document32 pagesHRM Session 1Yash NagarNo ratings yet
- Leadership: © 2015 Cengage LearningDocument45 pagesLeadership: © 2015 Cengage LearningHanah Camille GarabilloNo ratings yet
- Introduction To Management & Managing PeopleDocument95 pagesIntroduction To Management & Managing Peoplehillary opilloNo ratings yet
- Ob 27Document58 pagesOb 27Lakshmi NarayanNo ratings yet
- MPA Class Report Skills of An OD Practitioner FinalDocument55 pagesMPA Class Report Skills of An OD Practitioner FinaltonshieNo ratings yet
- Module 7Document9 pagesModule 7Jandrei Ezekiel LausNo ratings yet
- 3 W3 Organization Behavior1 2Document21 pages3 W3 Organization Behavior1 292vsmzv6t2No ratings yet
- Tlo 5 LeadingDocument43 pagesTlo 5 LeadingGerry Jimenez Sao-anNo ratings yet
- Motivation ProcessDocument7 pagesMotivation ProcessAmit729No ratings yet
- Professional Development CMDocument10 pagesProfessional Development CMapi-707173744No ratings yet
- UGM-Kompetensi Perawat Manajer IndonesiaDocument36 pagesUGM-Kompetensi Perawat Manajer IndonesiaNoval BastianNo ratings yet
- Leadership & Leadership Styles: BSS666: LECT 4Document72 pagesLeadership & Leadership Styles: BSS666: LECT 4Ahmad Muzakkir Ahmad FauziNo ratings yet
- Management Science: Unit-I Introduction To ManagementDocument27 pagesManagement Science: Unit-I Introduction To ManagementMamilla Naveen Kumar ReddyNo ratings yet
- Uncommonly Observant Leadership; Overcoming 'Management by Ignorance'From EverandUncommonly Observant Leadership; Overcoming 'Management by Ignorance'No ratings yet
- Git OnlineDocument82 pagesGit OnlineCarl JustineNo ratings yet
- Endo Modified PDFDocument35 pagesEndo Modified PDFCarl JustineNo ratings yet
- Note Jul 1, 2023Document45 pagesNote Jul 1, 2023Carl JustineNo ratings yet
- Fdar FormatDocument1 pageFdar FormatCarl JustineNo ratings yet
- Palmr Day 1 Atty. CapiliDocument12 pagesPalmr Day 1 Atty. CapiliCarl Justine100% (1)
- Chapter 7 - Forecasting HR SupplyDocument27 pagesChapter 7 - Forecasting HR SupplyAnish PenujuruNo ratings yet
- Human Resource PlanningDocument20 pagesHuman Resource PlanningKevin Fisher67% (3)
- Tutorial 4Document2 pagesTutorial 4syafiqahzinNo ratings yet
- Recruitment Agency in Pakistan For Saudi ArabiaDocument2 pagesRecruitment Agency in Pakistan For Saudi ArabiaTeleportManpower Consulting100% (1)
- Penilaian Akhir Semester 5 (A5) Tahun Pelajaran 2022-2023Document40 pagesPenilaian Akhir Semester 5 (A5) Tahun Pelajaran 2022-2023Karina RafaNo ratings yet
- Matrix OrganizationDocument1 pageMatrix OrganizationrizqiaisyahNo ratings yet
- Activity Template - Risk Management PlanDocument3 pagesActivity Template - Risk Management PlanshiteNo ratings yet
- Plan Financial Management Approaches - Task 1Document12 pagesPlan Financial Management Approaches - Task 1Tee Li MinNo ratings yet
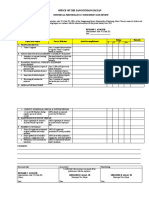
- Office of The Sangguniang Bayan: Individual Performance Commitment and ReviewDocument2 pagesOffice of The Sangguniang Bayan: Individual Performance Commitment and ReviewRichard C. Amoguis83% (6)
- Share Zimbabwejobs MONDAY - tuesDAYDocument64 pagesShare Zimbabwejobs MONDAY - tuesDAYOspen Noah SitholeNo ratings yet
- Module 4 To Module 6 POMDocument105 pagesModule 4 To Module 6 POMARYA JAIN 21111511No ratings yet
- Workplace Violence and Intervention 2011Document78 pagesWorkplace Violence and Intervention 2011izzyWanHalen100% (1)
- Lecture 8Document32 pagesLecture 8Tan Chee SengNo ratings yet
- Human Resource Management 512Document5 pagesHuman Resource Management 512NoxoloNo ratings yet
- Front Office VsDocument2 pagesFront Office VsJai De LeonNo ratings yet
- WWW - Kznhealth.gov - Za: Private Bag X9051, Pietermaritzburg, 3200 Human Resource Management ServicesDocument4 pagesWWW - Kznhealth.gov - Za: Private Bag X9051, Pietermaritzburg, 3200 Human Resource Management ServicesferhthyhrvdcecdcdcNo ratings yet
- Performance Evaluation of NestleDocument4 pagesPerformance Evaluation of NestleMomal Khawaja100% (2)
- Ambreen Hussain - NamazDocument5 pagesAmbreen Hussain - NamazAmbreen HussainNo ratings yet
- Managing: Work Flows and Conducting Job AnalysisDocument24 pagesManaging: Work Flows and Conducting Job AnalysisMelody Refaat AbdallaNo ratings yet
- Assignment 1 HRMDocument8 pagesAssignment 1 HRMnikita bajpaiNo ratings yet
- Project Work 01Document23 pagesProject Work 01Mr. JahirNo ratings yet
- OAM 680 - Spring 2024 - SyllabusDocument15 pagesOAM 680 - Spring 2024 - SyllabusVishal KhemaniNo ratings yet
- Organizational Behavior AnswersDocument35 pagesOrganizational Behavior AnswersGilbert BohiyanNo ratings yet
- Business FunctionsDocument12 pagesBusiness FunctionsKartelo 4132No ratings yet
- Ost Final Report BDocument36 pagesOst Final Report BPRANNAO RB 2127524No ratings yet
- 2 Project-Report-On-Recruitment-And-SelectionDocument79 pages2 Project-Report-On-Recruitment-And-SelectionMansoor khan100% (4)
- DR Case AnalysisDocument5 pagesDR Case AnalysisVaroon RNo ratings yet
- Advertisement For Fixed Term Engagement (FTE) - Unfilled VacancyDocument8 pagesAdvertisement For Fixed Term Engagement (FTE) - Unfilled VacancyQBIT bitNo ratings yet
- Role of Human Resource Management in Mergers and AcquisitionsDocument9 pagesRole of Human Resource Management in Mergers and AcquisitionsSHRUTI PILLAINo ratings yet
- CVSU SPMS Manual Revision 1 Final SignedDocument64 pagesCVSU SPMS Manual Revision 1 Final SignedXMARNo ratings yet