You might also like
- Concept Map On Acute PainDocument1 pageConcept Map On Acute PainKatherine Conlu Bengan0% (1)
- ABPS Exam Study GuideDocument37 pagesABPS Exam Study Guidepodjones100% (2)
- Palm Fisting, Thrombophlebitis, IV Cannulated Patient, VIP Score (Visual Infusion Phlebitis)Document8 pagesPalm Fisting, Thrombophlebitis, IV Cannulated Patient, VIP Score (Visual Infusion Phlebitis)Manashi SenguptaNo ratings yet
- Biomedical ResearchDocument8 pagesBiomedical ResearchTarek TarekNo ratings yet
- Observations: Disease DistributionDocument31 pagesObservations: Disease DistributionSarika RanaNo ratings yet
- Chapter-Iv Analysis and Interpretation in Quantitative Research Studies, Numerical Data Must Be Organized in AnDocument22 pagesChapter-Iv Analysis and Interpretation in Quantitative Research Studies, Numerical Data Must Be Organized in AnSonali DavidsonNo ratings yet
- Observations and Results: Table No. 1 Shows Percent Wise Distribution of Subjects in Control and Study GroupDocument34 pagesObservations and Results: Table No. 1 Shows Percent Wise Distribution of Subjects in Control and Study Groupmuqadar khanNo ratings yet
- Haematologica 2020 105:e349Document6 pagesHaematologica 2020 105:e349Mario SutantoNo ratings yet
- Pembrolizumab Plus Axitinib Versus Sunitinib For Advanced Renal-Cell Carcinoma (Keynote-426 Trial)Document6 pagesPembrolizumab Plus Axitinib Versus Sunitinib For Advanced Renal-Cell Carcinoma (Keynote-426 Trial)Manoj YadavNo ratings yet
- 10 1001@jamapediatrics 2020 0878 PDFDocument3 pages10 1001@jamapediatrics 2020 0878 PDFPaulNaranjoNo ratings yet
- JC Oncology55211005Document32 pagesJC Oncology55211005Neenuch ManeenuchNo ratings yet
- Serological Survey of Toxoplasma Gondii Infection Among Urban (Manila) and Suburban (Dasmariñas, Cavite) Residents, PhilippinesDocument8 pagesSerological Survey of Toxoplasma Gondii Infection Among Urban (Manila) and Suburban (Dasmariñas, Cavite) Residents, PhilippinesJohn Mark AndanNo ratings yet
- FTPDocument5 pagesFTPHaya RihanNo ratings yet
- Effect of Prepregnancy Body Mass Index and Gestational Weight Gain On Obstetric and Neonatal Outcomes - A Pilot StudyDocument5 pagesEffect of Prepregnancy Body Mass Index and Gestational Weight Gain On Obstetric and Neonatal Outcomes - A Pilot StudyJubair NewazNo ratings yet
- Pelvic Inflammatory DiseaseDocument48 pagesPelvic Inflammatory DiseaseAnonymouscatNo ratings yet
- Klasifikasi Usia Hipertensi CrosstabulationDocument12 pagesKlasifikasi Usia Hipertensi CrosstabulationRasyiqah Fitriyah RasyiNo ratings yet
- Serological Survey of Toxoplasma Gondii Infection Amoug Urban (Manila) and Suburban (Dasmarinas, Cavite) Residents, PhilippinesDocument9 pagesSerological Survey of Toxoplasma Gondii Infection Amoug Urban (Manila) and Suburban (Dasmarinas, Cavite) Residents, PhilippinesJohn Mark AndanNo ratings yet
- 1 - Up To 3 Year Follow Up of Patients W Vaginal Relax SindDocument6 pages1 - Up To 3 Year Follow Up of Patients W Vaginal Relax SindGustavo DolinskyNo ratings yet
- Effect of Sodium PAG2 TRADUCIDODocument2 pagesEffect of Sodium PAG2 TRADUCIDOJohanna Belen PaezNo ratings yet
- 1989-The Relationship Between Anemia in PregnancyDocument9 pages1989-The Relationship Between Anemia in Pregnancydw21541No ratings yet
- Article1385135472 - Rezaie Et AlDocument5 pagesArticle1385135472 - Rezaie Et AlimeldafitriNo ratings yet
- محمود وجدهمحمود وجدهDocument15 pagesمحمود وجدهمحمود وجدهmahmmoudeltaweelNo ratings yet
- Seizures and Angelman Syndrome Thiele Study ResultsDocument11 pagesSeizures and Angelman Syndrome Thiele Study Resultsbaba ababNo ratings yet
- Effect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialDocument24 pagesEffect of Ibuprofen Vs Acetaminophen On Postpartum Hypertension in Preeclampsia With Severe Features: A Double-Masked, Randomized Controlled TrialRiyan W. PratamaNo ratings yet
- Observation and ResultDocument42 pagesObservation and ResultPatrick JohnsonNo ratings yet
- Pain Managementin Medical WardsDocument8 pagesPain Managementin Medical WardsALYSSA MARIE MATANo ratings yet
- Paper18 25Document8 pagesPaper18 25Rachmat HidayatNo ratings yet
- Prevalence of Premenstrual Syndrome (PMS) Among Adolescent GirlsDocument4 pagesPrevalence of Premenstrual Syndrome (PMS) Among Adolescent Girlsfitriani fitriNo ratings yet
- Results DCI PareadosDocument5 pagesResults DCI PareadosAlfonsoSánchezNo ratings yet
- The Prognostic PotensialDocument10 pagesThe Prognostic PotensialPremiumstock90No ratings yet
- NIHMS1053940 Supplement 1Document6 pagesNIHMS1053940 Supplement 1Sara VillaNo ratings yet
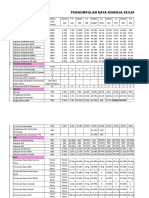
- Pengumpulan Data Kinerja Secara Periodik Tahun 2018Document6 pagesPengumpulan Data Kinerja Secara Periodik Tahun 2018rusdiyantiNo ratings yet
- Marine Drugs: The Potential of Neoagaro-Oligosaccharides As A Treatment of Type II Diabetes in MiceDocument17 pagesMarine Drugs: The Potential of Neoagaro-Oligosaccharides As A Treatment of Type II Diabetes in MiceSiapa HayoNo ratings yet
- Powerloom EmployersDocument44 pagesPowerloom Employerschandru ajiNo ratings yet
- Section - A Frequency and Percentage Distribution of Samples On Demographic Variables: Table: 1Document4 pagesSection - A Frequency and Percentage Distribution of Samples On Demographic Variables: Table: 1iCAN ComputersNo ratings yet
- 15 JMSCRDocument5 pages15 JMSCRVani Junior LoverzNo ratings yet
- A Cross Sectional Study of Metabolic Changes in Acanthosis Nigricans in AdolescentsDocument18 pagesA Cross Sectional Study of Metabolic Changes in Acanthosis Nigricans in AdolescentsIndhu GreenNo ratings yet
- BAB IV Translate ArifDocument11 pagesBAB IV Translate ArifDoc Arif AkhmadNo ratings yet
- Original Paper: Acid Peel in The Treatment of MelasmaDocument4 pagesOriginal Paper: Acid Peel in The Treatment of MelasmaEricka LemaNo ratings yet
- Sindrome MetabolicoDocument2 pagesSindrome MetabolicoDra Florencia BiroNo ratings yet
- Profile Frequency %: ResidencyDocument10 pagesProfile Frequency %: ResidencyMy Brain FartsNo ratings yet
- Table 1.: Assessment of ResponseDocument1 pageTable 1.: Assessment of ResponsejoycechicagoNo ratings yet
- Pergamon 0005-7967 (94) 00070-0: (Received 29 June 1994)Document5 pagesPergamon 0005-7967 (94) 00070-0: (Received 29 June 1994)Aggelou MayaNo ratings yet
- Results: Laksmi PW, Ainun N, Setyohadi B, Setiati S, Ariane A, Tirtarahardja GDocument1 pageResults: Laksmi PW, Ainun N, Setyohadi B, Setiati S, Ariane A, Tirtarahardja GNurAinunNo ratings yet
- CCO 2017 NASH Quiz Anstee DownloadableDocument42 pagesCCO 2017 NASH Quiz Anstee DownloadablePD18No ratings yet
- Annie Anderson Obesity The Elephant in The RoomDocument18 pagesAnnie Anderson Obesity The Elephant in The RoomVignesh JayaNo ratings yet
- Subgroup 3Document12 pagesSubgroup 3John Mervin OliverosNo ratings yet
- Amr Ppra Bethesda 2017 (DR Hari)Document29 pagesAmr Ppra Bethesda 2017 (DR Hari)Maya DamanikNo ratings yet
- Correlation Between Estrogen Receptor and Programmed Death Ligand-1 in Type I Endometrial Cancer - ScienceDirectDocument1 pageCorrelation Between Estrogen Receptor and Programmed Death Ligand-1 in Type I Endometrial Cancer - ScienceDirectTeguh RahardjoNo ratings yet
- Pengumpulan Data Kinerja Secara Periodik Tahun 2018Document6 pagesPengumpulan Data Kinerja Secara Periodik Tahun 2018rusdiyantiNo ratings yet
- Jco.2022.40.16 Suppl.9520Document1 pageJco.2022.40.16 Suppl.9520Beto MálagaNo ratings yet
- ResultsDocument13 pagesResultsAgnes MilomNo ratings yet
- Yurashevich 2020Document6 pagesYurashevich 2020Miftah Furqon AuliaNo ratings yet
- Body Composition and Leptin/Ghrelin Levels During Lenvatinib For Thyroid CancerDocument10 pagesBody Composition and Leptin/Ghrelin Levels During Lenvatinib For Thyroid CancerwafasahilahNo ratings yet
- Emerging InfectionDocument49 pagesEmerging InfectionTaufan LutfiNo ratings yet
- Revision Report FinalDocument6 pagesRevision Report FinalAnderson FellypNo ratings yet
- Thinness Gene Jo PoultonDocument18 pagesThinness Gene Jo PoultonHarline Jalire ValdiviaNo ratings yet
- Observations: Incidence of Age GroupDocument44 pagesObservations: Incidence of Age GroupKrishnaNo ratings yet
- Admin, ExampleDocument12 pagesAdmin, ExampleSilvio Cesar ViegasNo ratings yet
- Null 1Document45 pagesNull 1Ahmed samyNo ratings yet
- T1 T2 and T3 DRDocument4 pagesT1 T2 and T3 DRclaireclaireann69No ratings yet
- Gene RegulationDocument49 pagesGene RegulationNaina KalraNo ratings yet
- Toxic Diatoms & DinoflagellatesDocument28 pagesToxic Diatoms & DinoflagellatesNaina KalraNo ratings yet
- Bacterial Genetics PresentationDocument56 pagesBacterial Genetics PresentationNaina KalraNo ratings yet
- Prokaryotic TranslationDocument22 pagesProkaryotic TranslationNaina KalraNo ratings yet
- MicroorgansimsDocument2 pagesMicroorgansimsNaina KalraNo ratings yet
- Cholelithiasis POSTER (MAHEEN)Document1 pageCholelithiasis POSTER (MAHEEN)Naina KalraNo ratings yet
- COVID-19 (Precautions & PPEs)Document54 pagesCOVID-19 (Precautions & PPEs)Naina KalraNo ratings yet
- Deptmbp 7:30a 8:00a 8:30a 9:00a 9:30a 10:00a 10:30a 11:00a 11:30a 12:00p 12:30p 1:00p 1:30p 2:00p 2:30p 3:00p 3:30p 4:00p 4:30p 5:00p MonDocument3 pagesDeptmbp 7:30a 8:00a 8:30a 9:00a 9:30a 10:00a 10:30a 11:00a 11:30a 12:00p 12:30p 1:00p 1:30p 2:00p 2:30p 3:00p 3:30p 4:00p 4:30p 5:00p MonNaina KalraNo ratings yet
- Anesthesia 3Document97 pagesAnesthesia 3Ahmed Salah HadaraNo ratings yet
- Pondichery DoctorsDocument2 pagesPondichery Doctorspriya selvaraj50% (2)
- Nota Takafulink New Plan (Nota) SoftDocument7 pagesNota Takafulink New Plan (Nota) SoftShahrir RayNo ratings yet
- Đề Thi Thử THPT 2021 - Tiếng Anh - GV Vũ Thị Mai Phương - Đề 14 - Có Lời GiảiDocument16 pagesĐề Thi Thử THPT 2021 - Tiếng Anh - GV Vũ Thị Mai Phương - Đề 14 - Có Lời GiảiHanh YenNo ratings yet
- Tension Pneumothorax: Pediatric Respirology DivisionDocument20 pagesTension Pneumothorax: Pediatric Respirology DivisionAan AlawiyahNo ratings yet
- Anaesthesia Critical Care & Pain MedicineDocument26 pagesAnaesthesia Critical Care & Pain MedicineasiyazaidiaNo ratings yet
- Anaesthetic Concerns: Supraclavicular Block Was The Chosen Anaesthetic PlanDocument1 pageAnaesthetic Concerns: Supraclavicular Block Was The Chosen Anaesthetic PlanGokul RamNo ratings yet
- Versana-Balance V2 Transducer-Guide v3Document4 pagesVersana-Balance V2 Transducer-Guide v3azambinhassan26No ratings yet
- List of Medical Institutions Available For Foreign Language(s)Document24 pagesList of Medical Institutions Available For Foreign Language(s)leithNo ratings yet
- A True Complete Diphalliahas Proven To Be A More Complex Case of Caudal Duplication SyndromeDocument4 pagesA True Complete Diphalliahas Proven To Be A More Complex Case of Caudal Duplication SyndromeLuminita PopaNo ratings yet
- Philhealth: Coverage and ExclusionsDocument15 pagesPhilhealth: Coverage and ExclusionsJoher MendezNo ratings yet
- List of Nursing BooksDocument11 pagesList of Nursing BooksChakrapani Chaturvedi100% (1)
- Warming Up: 1. Discuss in Your Class: (Write Your Own Answers. Points Only Given For Reference)Document8 pagesWarming Up: 1. Discuss in Your Class: (Write Your Own Answers. Points Only Given For Reference)FOXTROTNo ratings yet
- Surgical Site Infections (SSI) : Dr. Mahmud Ul Alam Mondal (Saikat)Document42 pagesSurgical Site Infections (SSI) : Dr. Mahmud Ul Alam Mondal (Saikat)মাহমুদ সৈকতNo ratings yet
- Rectal CarcinomaDocument7 pagesRectal CarcinomaEbrahim Adel Ali AhmedNo ratings yet
- Clinical Experience With Surgical Debridement and Simultaneous Meshed Skin Grafts in Treating Biofilm-Associated Infection: An Exploratory Retrospective Pilot StudyDocument9 pagesClinical Experience With Surgical Debridement and Simultaneous Meshed Skin Grafts in Treating Biofilm-Associated Infection: An Exploratory Retrospective Pilot StudyAsmat BurhanNo ratings yet
- Work of The Cardiovascular Surgical InstrumentationDocument1 pageWork of The Cardiovascular Surgical Instrumentationapi-613248156No ratings yet
- Castration of Calves: Castration: Gettings The Best Results For Farm and Calf What Techniques Are Available?Document5 pagesCastration of Calves: Castration: Gettings The Best Results For Farm and Calf What Techniques Are Available?WAQAS SHAHIDNo ratings yet
- Influence of Chlorhexidine Rinsing On The Healing of Oral Mucosa and Osseous LesionsDocument15 pagesInfluence of Chlorhexidine Rinsing On The Healing of Oral Mucosa and Osseous LesionsAna Maria Montoya GomezNo ratings yet
- Cleft Palate (DeGuzman)Document16 pagesCleft Palate (DeGuzman)JhayneNo ratings yet
- Telescopes TontarraDocument20 pagesTelescopes Tontarrag5quadNo ratings yet
- Hospital DetailsDocument34 pagesHospital Detailsmolus030No ratings yet
- DePuy ASR Hip Recall Revision SurgeryDocument2 pagesDePuy ASR Hip Recall Revision SurgerydepuyhiprecallNo ratings yet
- Apf Clinic Aftercare InstructionsDocument4 pagesApf Clinic Aftercare InstructionsapNo ratings yet
- Medical Tourism in India Strengths and WeaknessesDocument4 pagesMedical Tourism in India Strengths and Weaknessesjimmy3229No ratings yet
- DR - KumarSonal No CVDocument3 pagesDR - KumarSonal No CVashish bondiaNo ratings yet
- Trans Women's Safer Sex GuideDocument36 pagesTrans Women's Safer Sex GuideHenry JohnNo ratings yet
- Pathologic Complete ResponseDocument5 pagesPathologic Complete ResponseNoe PaezNo ratings yet