You might also like
- מבחן דמה 2021 עם תשובותDocument65 pagesמבחן דמה 2021 עם תשובותYousef TaiserNo ratings yet
- שאלותחזרהלממשלתינוירולוגיהבליתשובות 1Document8 pagesשאלותחזרהלממשלתינוירולוגיהבליתשובות 1blue_blood_boyNo ratings yet
- הרצאה (5) מחלות UMN LMNDocument147 pagesהרצאה (5) מחלות UMN LMNMinikutshupNo ratings yet
- סיכום אלצהיימר ודמנציהDocument2 pagesסיכום אלצהיימר ודמנציהNasser Eddin JamalNo ratings yet
- שיעור 1 - מושגי יסוד בטיפול בכאבDocument4 pagesשיעור 1 - מושגי יסוד בטיפול בכאבItai Izhak100% (1)
- טבלת סיכום מחלות במערכת העצביםDocument7 pagesטבלת סיכום מחלות במערכת העצביםItai IzhakNo ratings yet
- שחזור פנימית א 2021Document14 pagesשחזור פנימית א 2021BluebloodboyNo ratings yet
- Introduction Cva PDFDocument5 pagesIntroduction Cva PDFNasser Eddin JamalNo ratings yet
- סם לכיתה- עותק של הכנה למבחןDocument44 pagesסם לכיתה- עותק של הכנה למבחןNasser Eddin JamalNo ratings yet
- אנמנזה ובדיקה גופניתDocument21 pagesאנמנזה ובדיקה גופניתapi-3705510No ratings yet
- טבלת סיכום מחלות ובדיקות פרובוקטיביותDocument4 pagesטבלת סיכום מחלות ובדיקות פרובוקטיביותNasser Eddin Jamal100% (1)
- ot test gov 15-5-2011.pdf שחזור מבחן ממשלתי למבחן רישוי בריפוי בעיסוקDocument16 pagesot test gov 15-5-2011.pdf שחזור מבחן ממשלתי למבחן רישוי בריפוי בעיסוקYasmen Jbareen100% (1)
- בחינה ממשלתית-שאלות נוירולוגיהDocument5 pagesבחינה ממשלתית-שאלות נוירולוגיהMinikutshupNo ratings yet
- שחזור 2014Document14 pagesשחזור 2014Yasmen Jbareen100% (1)
- שחזור ממשלתי- ספטמבר 2018Document19 pagesשחזור ממשלתי- ספטמבר 2018Dima OradovskyNo ratings yet
- Trauma 2003Document8 pagesTrauma 2003api-3824434No ratings yet
- כוויותDocument21 pagesכוויותאVי100% (1)
- בחינה ממשלתית שחזוריםDocument9 pagesבחינה ממשלתית שחזוריםתמי טרדימן0% (1)
- מבחן הסמכה 2004-1Document22 pagesמבחן הסמכה 2004-1api-3824434100% (1)
- בחינה ממשלתית-שאלות נוירולוגיהDocument5 pagesבחינה ממשלתית-שאלות נוירולוגיהMinikutshupNo ratings yet
- שיחזור קרדיולוגיה 2006Document4 pagesשיחזור קרדיולוגיה 2006api-3824434100% (2)
- שחזור סיעוד במצבי חירום 2020 מעודכןDocument5 pagesשחזור סיעוד במצבי חירום 2020 מעודכןשרה-אלינור וינברגרNo ratings yet
- הפרעות קצב הלבDocument33 pagesהפרעות קצב הלב13e100% (1)
- סיכום מקוצר טיפולים אנטיביוטיים סופיה קלינגDocument14 pagesסיכום מקוצר טיפולים אנטיביוטיים סופיה קלינגMOHAMAD HASSOUNANo ratings yet
- Physical Assesment 2008Document4 pagesPhysical Assesment 2008Anonymous 6iLtIrNo ratings yet
- סיכום שבוע מבוא כירורגיהDocument78 pagesסיכום שבוע מבוא כירורגיהoGamesStudioNo ratings yet
- התמודדות הקשיש והמשפחה, מעבר לבית אבותDocument50 pagesהתמודדות הקשיש והמשפחה, מעבר לבית אבותapi-19729700No ratings yet
- שחזור מבחן ברפואת ילדיםDocument5 pagesשחזור מבחן ברפואת ילדיםElla SharabiNo ratings yet
- מבחן אחיות מוסמכות ספטמבר 2012Document4 pagesמבחן אחיות מוסמכות ספטמבר 2012enterpricer100% (1)
- לחץ הדםDocument8 pagesלחץ הדםאVי100% (1)
- המודינמיקה אקדמיה 2008Document47 pagesהמודינמיקה אקדמיה 2008hirschmedNo ratings yet
- Pedyatrya 2005Document6 pagesPedyatrya 2005api-3824434100% (2)
- שחזור בפרמקולוגיה מועד אDocument3 pagesשחזור בפרמקולוגיה מועד אapi-26159412No ratings yet
- הזדקנותDocument25 pagesהזדקנותdd100% (1)
- תרופותDocument23 pagesתרופותIrina Tomshin100% (1)
- תרגול פרמקולוגיה בסיסית פרמקודינמיקה- ג'וניהDocument31 pagesתרגול פרמקולוגיה בסיסית פרמקודינמיקה- ג'וניהapi-3723461100% (1)
- טיפולים אנטיביוטיים-טבלאות סיכום (אילת) PDFDocument21 pagesטיפולים אנטיביוטיים-טבלאות סיכום (אילת) PDFMOHAMAD HASSOUNANo ratings yet
- שיעור מס' 27 - דלקת חריפה של הלבלבDocument8 pagesשיעור מס' 27 - דלקת חריפה של הלבלבrosenk100No ratings yet
- סדנא בחשיבה קלינית 1-ניתוח ארועים בסיעוד - דף הכנה לסטודנט בנושא הפרעות קצב - 485716Document5 pagesסדנא בחשיבה קלינית 1-ניתוח ארועים בסיעוד - דף הכנה לסטודנט בנושא הפרעות קצב - 485716sofNo ratings yet
- סיכומון אקגDocument7 pagesסיכומון אקגslumfi100% (1)
- 4. בדיקה קרדיווסקולרית - 1Document45 pages4. בדיקה קרדיווסקולרית - 1sarkisyanNo ratings yet
- שחזור מבחן מודולה משותפת קורס טיפול נמרץDocument3 pagesשחזור מבחן מודולה משותפת קורס טיפול נמרץaliszlawNo ratings yet
- שחזור 2020 מועד אDocument5 pagesשחזור 2020 מועד אddNo ratings yet
- ניתוחי כיס מרהDocument11 pagesניתוחי כיס מרהEvgeniy Edelman100% (1)
- Neuropathic PainDocument64 pagesNeuropathic Painapi-3723461100% (1)
- פרמקולוגיה תשסהDocument4 pagesפרמקולוגיה תשסהapi-26159412No ratings yet
- Pocket MedicDocument6 pagesPocket Medicreema_bannaNo ratings yet
- מבוגר 1 - סיכום הודיה איתן עטון -אסף הרופאDocument92 pagesמבוגר 1 - סיכום הודיה איתן עטון -אסף הרופאהודיה איתן עטוןNo ratings yet
- - מטלה בתכנית טיפול סיעודיDocument10 pages- מטלה בתכנית טיפול סיעודישרה-אלינור וינברגר100% (1)
- הטיפול הסיעודי בחולה מונשםDocument9 pagesהטיפול הסיעודי בחולה מונשםAnonymous 6iLtIrNo ratings yet
- תרופות אנטי פסיכוטיותDocument147 pagesתרופות אנטי פסיכוטיותראמי חנא100% (2)
- כוויותDocument3 pagesכוויותNasser Eddin JamalNo ratings yet
- חוברת למתמחהDocument18 pagesחוברת למתמחהAnonymous t6lassvLNo ratings yet
- תרגול מבחן שאלות חזרהDocument18 pagesתרגול מבחן שאלות חזרהQadri HaitamNo ratings yet
- צורות מתן תרופה - סיכום - איליDocument3 pagesצורות מתן תרופה - סיכום - איליIlanit Davidi100% (2)
- -אסיל זבידאת-תוכנית טיפולית כירורגיהDocument5 pages-אסיל זבידאת-תוכנית טיפולית כירורגיהפרג ואסיל זבידאת100% (1)
- Epileptic Seizures PredictionDocument13 pagesEpileptic Seizures PredictionMatan DahanNo ratings yet
- זה לא לחץ עצבי... זה דלקת ! NeuritisDocument2 pagesזה לא לחץ עצבי... זה דלקת ! NeuritisItai IzhakNo ratings yet
- 6-נוירו אורטופדיהDocument10 pages6-נוירו אורטופדיהitsik12886No ratings yet
- שליטה שרירת רביע תחתון (מצב תאימות)Document38 pagesשליטה שרירת רביע תחתון (מצב תאימות)MinikutshupNo ratings yet
- ניתוח הליכה פברואר 2011Document99 pagesניתוח הליכה פברואר 2011Minikutshup100% (1)
- מחקר רפואי וסטטיסטיקהDocument175 pagesמחקר רפואי וסטטיסטיקהMinikutshupNo ratings yet
- הערכה וטיפול נוירולוגיDocument94 pagesהערכה וטיפול נוירולוגיMinikutshup100% (1)
- Clinical NeurodynamicsDocument24 pagesClinical NeurodynamicsMinikutshupNo ratings yet
- בדיקות וניתוחים קרדיווסקולריותDocument143 pagesבדיקות וניתוחים קרדיווסקולריותMinikutshupNo ratings yet
- ספירומטריהDocument24 pagesספירומטריהMinikutshupNo ratings yet
- אנטומיה קרדיוווסרקולריתDocument123 pagesאנטומיה קרדיוווסרקולריתMinikutshupNo ratings yet
- Knee JointDocument56 pagesKnee JointMinikutshupNo ratings yet
- מחקר רפואי וסטטיסטיקהDocument178 pagesמחקר רפואי וסטטיסטיקהMinikutshupNo ratings yet
- מאזו חומצה ובסיסDocument27 pagesמאזו חומצה ובסיסMinikutshupNo ratings yet
- מחלות לב, כלי דם וריאות 24022011Document108 pagesמחלות לב, כלי דם וריאות 24022011MinikutshupNo ratings yet
- אנטומיה של מערכת הנשימה פברואר 2011Document46 pagesאנטומיה של מערכת הנשימה פברואר 2011MinikutshupNo ratings yet
- הנשמה מיכנית- אינדיקציות וסוגיםDocument78 pagesהנשמה מיכנית- אינדיקציות וסוגיםMinikutshup100% (1)
- אינדיקציות, קונטראינדיקציות, השפעות משניות, סיבוכיםDocument144 pagesאינדיקציות, קונטראינדיקציות, השפעות משניות, סיבוכיםMinikutshup100% (1)
- אינדיקציות, קונטראינדיקציות, השפעות משניות, סיבוכיםDocument144 pagesאינדיקציות, קונטראינדיקציות, השפעות משניות, סיבוכיםMinikutshup100% (1)
- תרמו&אלקטרותרפיהDocument120 pagesתרמו&אלקטרותרפיהMinikutshupNo ratings yet
- אנטומיה קרדיוווסרקולריתDocument123 pagesאנטומיה קרדיוווסרקולריתMinikutshupNo ratings yet
- שברים בקרסולDocument12 pagesשברים בקרסולMinikutshupNo ratings yet
- שברים בגפה עליונהDocument59 pagesשברים בגפה עליונהMinikutshup100% (1)
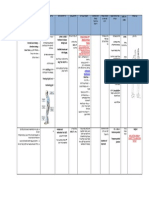
- טבלת+שבריDocument6 pagesטבלת+שבריMinikutshupNo ratings yet
- ניתוח הליכה פברואר 2011Document99 pagesניתוח הליכה פברואר 2011Minikutshup100% (1)
- אורטופדיה א - שברים באגןDocument18 pagesאורטופדיה א - שברים באגןMinikutshup100% (1)
- מפרק הירךDocument10 pagesמפרק הירךMinikutshupNo ratings yet
- אורתופדיה א - הקדמהDocument42 pagesאורתופדיה א - הקדמהMinikutshupNo ratings yet
- סיכום נחשDocument8 pagesסיכום נחשMinikutshupNo ratings yet
- טבלת+שברי 2Document5 pagesטבלת+שברי 2MinikutshupNo ratings yet
- אורטופדיה ב דסלוקציה בכתףDocument31 pagesאורטופדיה ב דסלוקציה בכתףMinikutshupNo ratings yet
- אורטופדיה א - דסלוקציות של הירךDocument67 pagesאורטופדיה א - דסלוקציות של הירךMinikutshupNo ratings yet
- אורטופדיה א - דסלוקציות של הירךDocument67 pagesאורטופדיה א - דסלוקציות של הירךMinikutshupNo ratings yet