You might also like
- ARTICLES A An The ZeroDocument12 pagesARTICLES A An The ZeroIvana LalicNo ratings yet
- 439 3 Electrophysiology & ECG BasicsDocument34 pages439 3 Electrophysiology & ECG BasicsjpoutreNo ratings yet
- Informacion GE Pick-Up TraserosDocument26 pagesInformacion GE Pick-Up Traserosemilio cortes100% (1)
- OPeration & Maintenance ManualDocument23 pagesOPeration & Maintenance ManualMohammed Esheaba100% (1)
- Basic Cephalometrics: Mark H. Taylor, D.D.S., F.A.C.DDocument32 pagesBasic Cephalometrics: Mark H. Taylor, D.D.S., F.A.C.DSelimir ProdanovicNo ratings yet
- Concordia Ch. - Synchronous Machines - Theory and Performance PDFDocument229 pagesConcordia Ch. - Synchronous Machines - Theory and Performance PDFRafael Alves100% (5)
- VERY IMP 2nd Mate Fun 1Document90 pagesVERY IMP 2nd Mate Fun 1Jayesh Solaskar100% (2)
- Environment and MarketDocument33 pagesEnvironment and MarketAnthonyNo ratings yet
- L R L R: SSEP Lower 2 Chanel SSEP Upper 4 ChanelDocument20 pagesL R L R: SSEP Lower 2 Chanel SSEP Upper 4 ChanelAndreas Arie WidiadiaksaNo ratings yet
- EIGA StandardsDocument4 pagesEIGA StandardsGnaniar IlangoNo ratings yet
- VlsiDocument1 pageVlsiYo Yo AnandNo ratings yet
- Vlsi SyllDocument2 pagesVlsi SyllYo Yo AnandNo ratings yet
- Scoring PSGDocument23 pagesScoring PSGMilky UniqueNo ratings yet
- M.o.sii - 17 Manual by SirDocument69 pagesM.o.sii - 17 Manual by SirMr. Danish SaeedNo ratings yet
- Hello Sunshine InstructionsDocument1 pageHello Sunshine InstructionsTricia Lynn Marshall JonesNo ratings yet
- Sistem UrinariaDocument8 pagesSistem UrinariaNofita AizzaNo ratings yet
- UTERUSDocument6 pagesUTERUSsneha ravichandranNo ratings yet
- Catalogo Eber 2018Document34 pagesCatalogo Eber 2018api-415596402No ratings yet
- CTTB Ques AfrDocument147 pagesCTTB Ques AfrKamrul Islam1996No ratings yet
- Sleep Stages and Basic Sleep Monitoring: Chapter PointsDocument11 pagesSleep Stages and Basic Sleep Monitoring: Chapter PointsnatalieNo ratings yet
- DESIGN OF VOLTAge AbstractDocument1 pageDESIGN OF VOLTAge AbstractnandeeshNo ratings yet
- Premiere WOKDocument2 pagesPremiere WOKEni AndrianiNo ratings yet
- Football Coaching Strategies 16Document4 pagesFootball Coaching Strategies 16derte linoNo ratings yet
- 4331-9642248 Certif TermoAnemometerDocument1 page4331-9642248 Certif TermoAnemometerjocalaNo ratings yet
- Shweta MaviDocument81 pagesShweta MaviAman SinghNo ratings yet
- Lecturelbp AngelatulaarforpresentationrecDocument80 pagesLecturelbp Angelatulaarforpresentationrecamelia rahayuNo ratings yet
- 5 Orbit For Dental Students 2Document18 pages5 Orbit For Dental Students 2Mohamad TallNo ratings yet
- PowerpointDocument44 pagesPowerpointmina bacayNo ratings yet
- C6 Upper Primary - Reproduction of AnimalsDocument9 pagesC6 Upper Primary - Reproduction of AnimalsHwee Hong AngNo ratings yet
- Guide Dilution EoaDocument1 pageGuide Dilution EoaMaja Bogicevic GavrilovicNo ratings yet
- Part1 PediaDocument12 pagesPart1 Pediavim rvNo ratings yet
- Tugas Bahasa Inggris - Ristika SuryaniDocument2 pagesTugas Bahasa Inggris - Ristika SuryaniEti JulianiNo ratings yet
- Klebsiell A Oxytoca: B L Se + B L SeDocument3 pagesKlebsiell A Oxytoca: B L Se + B L SeOussama KhelladiNo ratings yet
- Quantum Comms For ADGS GabeLDocument22 pagesQuantum Comms For ADGS GabeLOmaisNo ratings yet
- Horario de GradosDocument5 pagesHorario de GradosefrainNo ratings yet
- Transpetrosal ApproachDocument6 pagesTranspetrosal ApproachspiritNo ratings yet
- Igaatus A Sonemete Set Ob Tunning Fosk 1 KQ Hung: Czpeinnt IDocument2 pagesIgaatus A Sonemete Set Ob Tunning Fosk 1 KQ Hung: Czpeinnt IMrX GamingNo ratings yet
- Toyota Generic 3 - WPS OfficeDocument2 pagesToyota Generic 3 - WPS OfficeShoaib AhsanNo ratings yet
- Met Hod: Ful L Yaut Omat Edonest Epdi R Ectchemi L Umi Nescent I MmunoassayDocument3 pagesMet Hod: Ful L Yaut Omat Edonest Epdi R Ectchemi L Umi Nescent I MmunoassayAnupam Saraf IINo ratings yet
- Roads 14 May 2019Document1 pageRoads 14 May 2019tapiwanaishe maunduNo ratings yet
- Philips Low Volt PAR Lamps Bulletin 9-92Document4 pagesPhilips Low Volt PAR Lamps Bulletin 9-92Alan MastersNo ratings yet
- MCQsDocument64 pagesMCQsHussnain AslamNo ratings yet
- Maju 4Document1 pageMaju 4Ardina Nur PramudhitaNo ratings yet
- OCT OPTOM DR Sudha Cugati 2Document76 pagesOCT OPTOM DR Sudha Cugati 2Dung Duong TrungNo ratings yet
- Arrays 2 Aug22Document15 pagesArrays 2 Aug22Sachin ManeNo ratings yet
- CBCS - ISEM - Electrical - LabDocument29 pagesCBCS - ISEM - Electrical - LabManjot SinghNo ratings yet
- Rashid 240228 200709Document9 pagesRashid 240228 200709sneha singhNo ratings yet
- Some OF: Instructor Anatomy, University Miclbigan. F R o M The Anatomical Laboratory The Johns Hoplcins UniversityDocument80 pagesSome OF: Instructor Anatomy, University Miclbigan. F R o M The Anatomical Laboratory The Johns Hoplcins Universityevangelista daviNo ratings yet
- 2003 ÀåÀ È PDFDocument33 pages2003 ÀåÀ È PDFCon Chồn Phép ThuậtNo ratings yet
- Group 06 Lab 04Document6 pagesGroup 06 Lab 04ZabeehullahmiakhailNo ratings yet
- The Velas M EtaverseDocument9 pagesThe Velas M EtaverseFrancisco MartinezNo ratings yet
- CS 341p Crop ProtectionDocument36 pagesCS 341p Crop Protectiongiftmuyuni2020No ratings yet
- Mo in PGP-GP 1Document39 pagesMo in PGP-GP 1BINDU ENo ratings yet
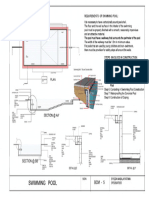
- SWI MMI NG Pool: SI GNDocument1 pageSWI MMI NG Pool: SI GNlerasat267No ratings yet
- DND Story Mode Character Sheet SpellsDocument1 pageDND Story Mode Character Sheet SpellsDaniel Hidalgo VerzobiasNo ratings yet
- C6 Lower Primary - 3 States of MatterDocument9 pagesC6 Lower Primary - 3 States of MatterHwee Hong AngNo ratings yet
- Semest Er - 3ecesyl L Abus (Analogelectroni CS)Document2 pagesSemest Er - 3ecesyl L Abus (Analogelectroni CS)Anurag ThakurNo ratings yet
- Mri Spine by DR ShamolDocument309 pagesMri Spine by DR Shamolالقارئ محمد سيد عباس mohamed sayed abassNo ratings yet
- Epesiment No: NationDocument11 pagesEpesiment No: NationBhanu MacharlaNo ratings yet
- WBC CountDocument5 pagesWBC CountJanhavi DeshmukhNo ratings yet
- Cartography 1 CAT SET 1Document2 pagesCartography 1 CAT SET 1MikNo ratings yet
- Sci Additional NotesDocument16 pagesSci Additional NotesdescalzotahNo ratings yet
- BIOLOGY Q1 Mod5Document12 pagesBIOLOGY Q1 Mod5Karen Mae CastilloNo ratings yet
- 5th To 8trh Sem ECE SyllabusDocument45 pages5th To 8trh Sem ECE Syllabusapi-3856240100% (2)
- LP VI Bi Lab ManualDocument28 pagesLP VI Bi Lab Manualgpay94348No ratings yet
- Navigating The Challenges and Unlocking The Potential: An Exploration of Small Scale and Cottage Industries in KalimpongDocument38 pagesNavigating The Challenges and Unlocking The Potential: An Exploration of Small Scale and Cottage Industries in KalimpongInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Info Sphere Information Analyzer - Methodology and Best PracticesDocument127 pagesInfo Sphere Information Analyzer - Methodology and Best PracticesRoshava KratunaNo ratings yet
- Finished Goods Inventories XX Work in Progress XX To Record The Completed JobDocument6 pagesFinished Goods Inventories XX Work in Progress XX To Record The Completed JobClarissa TeodoroNo ratings yet
- Spanish 1 Unidad 3 Etapa 2Document36 pagesSpanish 1 Unidad 3 Etapa 2api-293988969No ratings yet
- Superior Vena Cava Flow 2020Document6 pagesSuperior Vena Cava Flow 2020Betül DUMANNo ratings yet
- June 2018 QP Unified Physics A Level OCR PhysicsDocument20 pagesJune 2018 QP Unified Physics A Level OCR PhysicsJude PereraNo ratings yet
- Colour Television Chassis: Block Diagram, Testpoints, I C and Supply Voltage OverviewDocument72 pagesColour Television Chassis: Block Diagram, Testpoints, I C and Supply Voltage OverviewadrianATL20No ratings yet
- D33116505 - Muh Halilul Rohman - TGS Matek 4Document12 pagesD33116505 - Muh Halilul Rohman - TGS Matek 4muh halilul rohmanNo ratings yet
- Komatsu Wa95 3 Operation Maintenance ManualDocument10 pagesKomatsu Wa95 3 Operation Maintenance Manualrhonda100% (25)
- CV Lacp IfccDocument4 pagesCV Lacp Ifcclubna aloshibiNo ratings yet
- Sylvania Lc370ss9 LCD TV SMDocument61 pagesSylvania Lc370ss9 LCD TV SMstechs02100% (1)
- BS Iso 05667-6-2014Document40 pagesBS Iso 05667-6-2014mohamed senoussi100% (1)
- AwsrgmstDocument996 pagesAwsrgmstKanha MishraNo ratings yet
- S Setting Value, C Check Value) OT Outside Tolerance (X Is Set)Document5 pagesS Setting Value, C Check Value) OT Outside Tolerance (X Is Set)carlos puertoNo ratings yet
- TSG Roles and ResponsibilitiesDocument10 pagesTSG Roles and ResponsibilitiesdinesharikaNo ratings yet
- Forensic 1 Fifty Definition of Terms To Be ReciteDocument3 pagesForensic 1 Fifty Definition of Terms To Be Recitemarkroviclarito100% (1)
- M53 Lec4.4 Area and ArclengthDocument141 pagesM53 Lec4.4 Area and Arclengthcriscab12345100% (1)
- A First Look at Browser-Based CryptojackingDocument10 pagesA First Look at Browser-Based CryptojackingTá CheioNo ratings yet
- 3.4ii. BoK 11 - 001 Collection Pavement Structural Parameters Part II - VERY GOODDocument65 pages3.4ii. BoK 11 - 001 Collection Pavement Structural Parameters Part II - VERY GOODSpiros Licoudis100% (1)
- I. Safe and Quality Nursing CareDocument12 pagesI. Safe and Quality Nursing CareJoanne Sosa تNo ratings yet
- Noel Angelo M. Pineda: Personal DataDocument2 pagesNoel Angelo M. Pineda: Personal DataNoel AngeloNo ratings yet
- KidsBox PreA1 Starters Practice TestDocument14 pagesKidsBox PreA1 Starters Practice TestMonika GodlewskaNo ratings yet
- Microeconomics Fifteenth Canadian Edition Campbell R Mcconnell Full ChapterDocument53 pagesMicroeconomics Fifteenth Canadian Edition Campbell R Mcconnell Full Chapterjacqueline.newman665100% (2)