You might also like
- What is Jaundice? Causes, Types and DiagnosisDocument29 pagesWhat is Jaundice? Causes, Types and DiagnosisARUSHI ARVINDNo ratings yet
- Everything You Need to Know About JaundiceDocument29 pagesEverything You Need to Know About JaundiceAzizul HalidNo ratings yet
- Practical Guide to Serum Bilirubin LevelsDocument4 pagesPractical Guide to Serum Bilirubin LevelsAli MehmetNo ratings yet
- Estimation of Serum Bilirubin Total Direct 1Document16 pagesEstimation of Serum Bilirubin Total Direct 1Priya singhNo ratings yet
- BilirubinDocument3 pagesBilirubinIkhza LastPandawaNo ratings yet
- JaundiceDocument53 pagesJaundiceAbhishiktaAbhiNo ratings yet
- 8 BilirubinDocument25 pages8 BilirubinTagreed DerarNo ratings yet
- Chem-Dr - Zainab-Bilirubin-Lab 2Document10 pagesChem-Dr - Zainab-Bilirubin-Lab 2gmpcbpzdysNo ratings yet
- RBC Degradation & Causes of JaundiceDocument30 pagesRBC Degradation & Causes of JaundiceSubhi MishraNo ratings yet
- Causes and Classification of JaundiceDocument23 pagesCauses and Classification of JaundicetrcfghNo ratings yet
- Liver PathologyDocument35 pagesLiver Pathologynhgwdwffp2No ratings yet
- Causes of Jaundice: Signs and SymptomsDocument9 pagesCauses of Jaundice: Signs and Symptomspragna novaNo ratings yet
- Jaundice: Signs and SymptomsDocument6 pagesJaundice: Signs and Symptomshero111983No ratings yet
- Metabolism of BilirubinDocument3 pagesMetabolism of BilirubinEris Abdul Aziz100% (1)
- JaundiceDocument4 pagesJaundiceShubhamNo ratings yet
- Bilirubin Levels and JaundiceDocument34 pagesBilirubin Levels and JaundiceKmo mastnNo ratings yet
- ictericia diagnostico ravindran2020Document7 pagesictericia diagnostico ravindran2020Francisco CarpioNo ratings yet
- Bilirubin Metabolism and HyperbilirubinaemiasDocument35 pagesBilirubin Metabolism and HyperbilirubinaemiasEuphrasiaNo ratings yet
- Hemoglobin Catabolism and BilirubinDocument2 pagesHemoglobin Catabolism and BilirubinJacob MasikaNo ratings yet
- Jaundice FinalDocument30 pagesJaundice FinalFrances GrefalNo ratings yet
- Heme DegradationDocument26 pagesHeme DegradationDerick SemNo ratings yet
- Metabolisme Bilirubin Blok 11 2016Document22 pagesMetabolisme Bilirubin Blok 11 2016Astri Hardianti RahimNo ratings yet
- Liver Function Tests (LFTS)Document18 pagesLiver Function Tests (LFTS)farkad rawiNo ratings yet
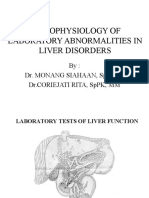
- Pathophysiology of Laboratory Abnormalities in Liver DisordersDocument55 pagesPathophysiology of Laboratory Abnormalities in Liver DisordersYudha fedrian AKNo ratings yet
- Bilirubin Metabolism: Hd. - Msc. (Biochemistry)Document18 pagesBilirubin Metabolism: Hd. - Msc. (Biochemistry)MuhamadMarufNo ratings yet
- 5 - JaundiceDocument16 pages5 - JaundiceHamzehNo ratings yet
- Jaundice: From Wikipedia, The Free EncyclopediaDocument27 pagesJaundice: From Wikipedia, The Free Encyclopediacherryann_calinogNo ratings yet
- BilirubinDocument2 pagesBilirubinZukhruful MuzakkieNo ratings yet
- Assignment 3 BilirubbinDocument5 pagesAssignment 3 Bilirubbinhaseeb ShafaatNo ratings yet
- Jaundice UN 2023 PDFDocument57 pagesJaundice UN 2023 PDFRabiaNo ratings yet
- Uvod:: Total BilirubinDocument5 pagesUvod:: Total BilirubingrgicosNo ratings yet
- Jaundice Symptoms, Causes & Types Explained in 40 CharactersDocument14 pagesJaundice Symptoms, Causes & Types Explained in 40 CharactersAnuradha NanayakkaraNo ratings yet
- Chapter 1 Liver FunctionDocument41 pagesChapter 1 Liver FunctionDaniel HikaNo ratings yet
- Hepatobiliary DiseaseDocument27 pagesHepatobiliary DiseaseGrace NazarenoNo ratings yet
- Liver EnzymesDocument6 pagesLiver EnzymesWande AyodeleNo ratings yet
- HB Degradation and Related ProblemDocument23 pagesHB Degradation and Related ProblemHatim AlnourNo ratings yet
- Liver Function Mazen 1Document24 pagesLiver Function Mazen 1Ahmed GaberNo ratings yet
- The Biochemistry of Jaundice ExplainedDocument29 pagesThe Biochemistry of Jaundice ExplainedeminemizenNo ratings yet
- Bilirubin Group2Document53 pagesBilirubin Group2ChiNo ratings yet
- HB Degradation: D.Hythem SaeedDocument34 pagesHB Degradation: D.Hythem Saeedsamar yousif mohamed100% (1)
- Jaundice 03Document24 pagesJaundice 03kuldeep sainiNo ratings yet
- Kuliah Bill Gite Harly 2013Document41 pagesKuliah Bill Gite Harly 2013DaniaPutriNo ratings yet
- Tests for Liver Function: Serum BilirubinDocument4 pagesTests for Liver Function: Serum BilirubinHiba EmadNo ratings yet
- BilirubinDocument6 pagesBilirubinwandebesNo ratings yet
- JAUNDICE pptm-1Document29 pagesJAUNDICE pptm-1jismi vallachiraNo ratings yet
- cc2 Lectures AllDocument256 pagescc2 Lectures AllJayson Dagohoy SudioNo ratings yet
- 212 Spring 2005 Heme DegradationDocument17 pages212 Spring 2005 Heme Degradationcockatoo_whiteNo ratings yet
- Jaundice Syndrome: Liver Chemistry Panelserum Total and Fractioned Direct Bilirubin Should Be Obtained. in CholestasisDocument4 pagesJaundice Syndrome: Liver Chemistry Panelserum Total and Fractioned Direct Bilirubin Should Be Obtained. in CholestasisManusheeNo ratings yet
- Liver Function Test (TSB)Document25 pagesLiver Function Test (TSB)shafyd ramdanNo ratings yet
- Liver Panel: EM 6203 Dr. K. AikenheadDocument24 pagesLiver Panel: EM 6203 Dr. K. AikenheadCrystal Lynn Keener SciariniNo ratings yet
- Heme Metabolism and Bilirubin ProcessingDocument1 pageHeme Metabolism and Bilirubin ProcessingmargeNo ratings yet
- Which of The Two Is More Liver Specific and Increases More During Liver DiseaseDocument8 pagesWhich of The Two Is More Liver Specific and Increases More During Liver DiseaseMariel AbatayoNo ratings yet
- JaundiceDocument4 pagesJaundiceAbo Omar Ahmed100% (1)
- Biochemistry of Jaundice Group 2 FinalDocument44 pagesBiochemistry of Jaundice Group 2 FinalShanna SolideoNo ratings yet
- Jaundice: DR: Ramy A. SamyDocument42 pagesJaundice: DR: Ramy A. Samyoscar3spurgeonNo ratings yet
- Jaundice Diagnosis and ClassificationDocument29 pagesJaundice Diagnosis and ClassificationShravan SharmaNo ratings yet
- BIOCHEM Jaundice FinalDocument54 pagesBIOCHEM Jaundice FinalJohnRobynDiezNo ratings yet
- JaundiceDocument19 pagesJaundiceketsela12No ratings yet
- Jaundice, (Hyperbilirubinemia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandJaundice, (Hyperbilirubinemia) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
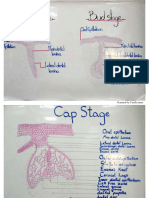
- Drawings - First term (صور الكلية)Document16 pagesDrawings - First term (صور الكلية)Kamal AhmedNo ratings yet
- 03 - Mechanical PrinciplesDocument50 pages03 - Mechanical PrinciplesKamal AhmedNo ratings yet
- Drawings - Second TermDocument19 pagesDrawings - Second TermKamal AhmedNo ratings yet
- 1 HepatitisDocument62 pages1 HepatitisKamal AhmedNo ratings yet
- 6 JaundiceDocument36 pages6 JaundiceKamal AhmedNo ratings yet
- 1 Terminology ShamsDocument248 pages1 Terminology ShamsKamal AhmedNo ratings yet
- Resin Composite 2Document47 pagesResin Composite 2Kamal AhmedNo ratings yet
- 3 Liver CirrhosisDocument50 pages3 Liver CirrhosisKamal AhmedNo ratings yet
- 3 Finish LineDocument81 pages3 Finish LineKamal AhmedNo ratings yet
- 7 Porcelin Construction ShamsDocument73 pages7 Porcelin Construction ShamsKamal AhmedNo ratings yet
- Aerobic Respiration 1 QPDocument13 pagesAerobic Respiration 1 QPKHANSANo ratings yet
- Why cells remain small: Surface area to volume ratioDocument3 pagesWhy cells remain small: Surface area to volume ratioMay TreeNo ratings yet
- Postions Movement Bones JointsDocument8 pagesPostions Movement Bones JointsNini BakradzeNo ratings yet
- Human Anatomy and PhysiologyDocument4 pagesHuman Anatomy and PhysiologyClarish Ann CaranzoNo ratings yet
- Special Stains and Its Applications in HistopathologyDocument18 pagesSpecial Stains and Its Applications in HistopathologyIJAR JOURNAL100% (2)
- Physiology RAASDocument3 pagesPhysiology RAASAulia Mahya FaradisaNo ratings yet
- Introduction To Biochemistry - Activity 2Document1 pageIntroduction To Biochemistry - Activity 2Lanette Liana A. LocaylocayNo ratings yet
- Torehj 6 1 PDFDocument20 pagesTorehj 6 1 PDFSaifuddin HaswareNo ratings yet
- Alternative Item Formats: Sample QuestionsDocument33 pagesAlternative Item Formats: Sample QuestionsCristianFranceschi100% (2)
- 9th Biology - Chapter 1 The Fundamental Unit of LifeDocument38 pages9th Biology - Chapter 1 The Fundamental Unit of LifeAbhaya RanjanNo ratings yet
- NSSCH Specimen Bio Apr2006Document54 pagesNSSCH Specimen Bio Apr2006AngelNo ratings yet
- Module 11, Chapter 27:: University of Cebu-BaniladDocument10 pagesModule 11, Chapter 27:: University of Cebu-BaniladSuzanne Kyla CabuenasNo ratings yet
- Editing File: Recognizing Major Renal Glomerular SyndromesDocument22 pagesEditing File: Recognizing Major Renal Glomerular SyndromesmariapaulaguerrerocNo ratings yet
- II) Coagulase Test: ProcedureDocument4 pagesII) Coagulase Test: ProcedureMd Ahsanul HaqueNo ratings yet
- Local Media3530622189352282331Document26 pagesLocal Media3530622189352282331Novie Carla GayosaNo ratings yet
- YCT Anatomy of Flowering Plants NEET Questions PracticeDocument36 pagesYCT Anatomy of Flowering Plants NEET Questions PracticepreitaphilenaNo ratings yet
- Types of Placenta ClassificationDocument16 pagesTypes of Placenta Classificationmuqadar khanNo ratings yet
- Anatomy of The Female Reproductive SystemDocument63 pagesAnatomy of The Female Reproductive SystemMahmoud Abu Al AmrainNo ratings yet
- Cambridge International General Certificate of Secondary EducationDocument16 pagesCambridge International General Certificate of Secondary EducationMohammad Shahidullah ChowdhuryNo ratings yet
- Shivering and Neuraxial AnesthesiaDocument12 pagesShivering and Neuraxial AnesthesiaKarla Albert ReyesNo ratings yet
- Laboratory Activity No. 10: Frog Circulatory and Excretory SystemDocument5 pagesLaboratory Activity No. 10: Frog Circulatory and Excretory SystemMaricris GuillermoNo ratings yet
- Biokemistri Volume 32, Number 1Document95 pagesBiokemistri Volume 32, Number 1Clement BewajiNo ratings yet
- VETRO DESIGN SRL Medical CatalogDocument104 pagesVETRO DESIGN SRL Medical CatalogCristiDanNo ratings yet
- External Anatomy of Toad: Stephen C. Capilitan, MSTDocument24 pagesExternal Anatomy of Toad: Stephen C. Capilitan, MSTSofia RatuisteNo ratings yet
- Importance of CBC in disease diagnosisDocument21 pagesImportance of CBC in disease diagnosisDr Millon RoutNo ratings yet
- Experiment and Activity CellDocument4 pagesExperiment and Activity CellPang ChixxNo ratings yet
- Simple Epithelium-Found in Areas That Require Stratified Epithelium - More Than One Layer of CellsDocument4 pagesSimple Epithelium-Found in Areas That Require Stratified Epithelium - More Than One Layer of CellsDimple Lexiry Gloria100% (1)
- Department of Education: Individual Output On Unpacked MelcsDocument1 pageDepartment of Education: Individual Output On Unpacked MelcsBalagtas VinaNo ratings yet
- Herpetology: An Introductory Biology of Amphibians and ReptilesDocument4 pagesHerpetology: An Introductory Biology of Amphibians and ReptilesChristine BantilingNo ratings yet
- Roitt'S Essential Immunology 12Th Edition (All Mcqs With Answers)Document100 pagesRoitt'S Essential Immunology 12Th Edition (All Mcqs With Answers)Kiran Krupa100% (6)