You might also like
- Psychiatric Times - Malingering Key Points in Assessment - 2016-04-18Document9 pagesPsychiatric Times - Malingering Key Points in Assessment - 2016-04-18parahNo ratings yet
- 4 Bedroom 2 Storey ResidenceDocument7 pages4 Bedroom 2 Storey ResidenceJoel Victor Amicay100% (3)
- P E R S P E C T I V E: Site Developement Plan Vicinity Map Key MapDocument12 pagesP E R S P E C T I V E: Site Developement Plan Vicinity Map Key Maprolando dionisio100% (1)
- Archi-Struct 2Document14 pagesArchi-Struct 2The crypto GuyNo ratings yet
- SAMPLE Complete Set of Plan - Single - Storey PDFDocument8 pagesSAMPLE Complete Set of Plan - Single - Storey PDFKyla Joy JimenezNo ratings yet
- Final Fence Set PlanDocument2 pagesFinal Fence Set PlanNnelg Nimsaj Aveunalliv100% (1)
- Differentiating Bronchiolitis and PneumoniaDocument17 pagesDifferentiating Bronchiolitis and PneumoniaRizky DarmawanNo ratings yet
- Milliken's Complete Book of Instant Activities - Grade 4: Over 110 Reproducibles for Today's Differentiated ClassroomFrom EverandMilliken's Complete Book of Instant Activities - Grade 4: Over 110 Reproducibles for Today's Differentiated ClassroomNo ratings yet
- Exterior Perspective: ArchitecturalDocument5 pagesExterior Perspective: ArchitecturalChristian ReyesNo ratings yet
- Land Use & Zoning: Line & GradeDocument19 pagesLand Use & Zoning: Line & GradeVicson RiveraNo ratings yet
- Activity Intolerance Related To ImmobilizationDocument3 pagesActivity Intolerance Related To ImmobilizationAgronaSlaughterNo ratings yet
- Typical Plan For Construction of 2 STOREY Regular Workshop, 4 CLASSROOM SHSDocument37 pagesTypical Plan For Construction of 2 STOREY Regular Workshop, 4 CLASSROOM SHSFernandez DanielNo ratings yet
- Final Physical ExaminationDocument3 pagesFinal Physical Examinationapi-620159117No ratings yet
- PneumothoraxDocument6 pagesPneumothoraxNader Smadi100% (1)
- Philippine school building plans and specificationsDocument90 pagesPhilippine school building plans and specificationsArch EnemyNo ratings yet
- The Respiratory SystemDocument117 pagesThe Respiratory SystemPark chin-haeNo ratings yet
- 2 Storey 6 Classroom BuildingDocument15 pages2 Storey 6 Classroom BuildingDhan VincentNo ratings yet
- Stair Foundation Detail at Beam: Rosario L. RostataDocument1 pageStair Foundation Detail at Beam: Rosario L. RostataJesusAntonioJugosNo ratings yet
- Chest X-RayDocument101 pagesChest X-RayYuke04No ratings yet
- Building Permit RecommendationDocument14 pagesBuilding Permit RecommendationAlexander Osmeña IINo ratings yet
- Test Bank For Clinical Application of Mechanical Ventilation 4th Edition Chang Isbn 10 1111539588 Isbn 13 9781111539580Document6 pagesTest Bank For Clinical Application of Mechanical Ventilation 4th Edition Chang Isbn 10 1111539588 Isbn 13 9781111539580swungnauticalden100% (1)
- Science 9 DLL Session 1Document5 pagesScience 9 DLL Session 1NikkieIrisAlbañoNovesNo ratings yet
- Intubation Set Equipment & FunctionsDocument4 pagesIntubation Set Equipment & FunctionsJrBong Semanero100% (1)
- MECONIUM Aspiration SyndromeDocument37 pagesMECONIUM Aspiration SyndromekamalaNo ratings yet
- PDF 2Document1 pagePDF 2Lintank AbdillahNo ratings yet
- Coca-Cola Mop - Installation of New Comressort - AsbuiltDocument5 pagesCoca-Cola Mop - Installation of New Comressort - AsbuiltJareem PeesNo ratings yet
- Site development plan for Republic of the PhilippinesDocument1 pageSite development plan for Republic of the PhilippinesVon Philip DecenaNo ratings yet
- Jl. TamblongDocument1 pageJl. TamblongImamHerriansyahNo ratings yet
- Water Tank Sanitary Plumbing PlanDocument1 pageWater Tank Sanitary Plumbing PlanPhineas FlynnNo ratings yet
- Typical Plan For Construction of 2 STOREY Regular Workshop 4 CLASSROOM SHS - ResizedDocument37 pagesTypical Plan For Construction of 2 STOREY Regular Workshop 4 CLASSROOM SHS - ResizedAshley Van Goele BalubarNo ratings yet
- Typical Plan For Construction of 2 STOREY Regular Workshop, 4 CLASSROOM SHSDocument37 pagesTypical Plan For Construction of 2 STOREY Regular Workshop, 4 CLASSROOM SHSJmransNo ratings yet
- Building plan reinforcement detailsDocument1 pageBuilding plan reinforcement detailsJesusAntonioJugosNo ratings yet
- Perspective View: Roller Guide DetailsDocument1 pagePerspective View: Roller Guide DetailsPhineas FlynnNo ratings yet
- Hall-Plan-2024-2Document1 pageHall-Plan-2024-2苏先生No ratings yet
- Concrete Beam Design and Reinforcement DetailsDocument1 pageConcrete Beam Design and Reinforcement DetailsAndre Joseph OrtizNo ratings yet
- CucuDocument1 pageCucuJuan Carlos Marquez RodenasNo ratings yet
- Two Storey Residential House PDF 5 PDF FreeDocument9 pagesTwo Storey Residential House PDF 5 PDF FreeRiowin GamboaNo ratings yet
- Perspective A: KarevDocument1 pagePerspective A: KarevJohn Paul GutierrezNo ratings yet
- Construction Drawings 2Document21 pagesConstruction Drawings 2engr.jerico.abaoNo ratings yet
- E W S N: Not To Scale A-1Document1 pageE W S N: Not To Scale A-1zab04148114No ratings yet
- S1 Matting S2 Matting Wall Matting: Sorsogon City Bulk Water Supply As-Built Plan For Water Treatment PlantDocument1 pageS1 Matting S2 Matting Wall Matting: Sorsogon City Bulk Water Supply As-Built Plan For Water Treatment PlantAlphaMae DitanNo ratings yet
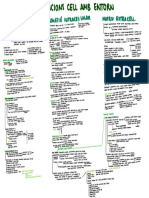
- Relacions Cell Amb EntornDocument1 pageRelacions Cell Amb Entornqueralt.collado.carcelNo ratings yet
- NayaDocument13 pagesNayaMikhail LeeNo ratings yet
- A1 PDFDocument1 pageA1 PDFOculus ConstructoresNo ratings yet
- Globalization and Inclusive Growth in AKI Report: DLSU-WB Project Advocates Public Service MonitoringDocument2 pagesGlobalization and Inclusive Growth in AKI Report: DLSU-WB Project Advocates Public Service MonitoringAve Gaile PerazNo ratings yet
- Second Floor Plan: Architect BuilderDocument1 pageSecond Floor Plan: Architect BuilderGore AtienzaNo ratings yet
- Stair Railing and Granite Treads PDFDocument1 pageStair Railing and Granite Treads PDFbobosNo ratings yet
- Site Vicinity Map Site Development Plan Perspective - UP BaguioDocument13 pagesSite Vicinity Map Site Development Plan Perspective - UP BaguioErjie GerasmioNo ratings yet
- Complete Construction DrawingDocument9 pagesComplete Construction DrawingJerwin TarucNo ratings yet
- Plano ASPRODocument1 pagePlano ASPROMiguel Angel Cardozo MolinaNo ratings yet
- Line Pipe TCUDocument1 pageLine Pipe TCUI Made Candra IrawanNo ratings yet
- Jefferson County Sample Ballot 2022 General ElectionDocument1 pageJefferson County Sample Ballot 2022 General ElectionCBS 4250% (2)
- ../render Photo and Videos/render New - JPG: PerspectiveDocument1 page../render Photo and Videos/render New - JPG: Perspectivemj sabioNo ratings yet
- Department of Public Works and Highways Architectural: City / District / MunicipalityDocument1 pageDepartment of Public Works and Highways Architectural: City / District / MunicipalityStephen A. CuizonNo ratings yet
- S Ecti On Thru 'B-B': Roof P L A NDocument1 pageS Ecti On Thru 'B-B': Roof P L A NAntonio CunananNo ratings yet
- Vellore DivisionDocument1 pageVellore DivisionDilesh KumarNo ratings yet
- COVER SHEET ArchlDocument1 pageCOVER SHEET ArchlShayna Rei MirañaNo ratings yet
- 6904132-ELE (1) 11-06 LRDocument8 pages6904132-ELE (1) 11-06 LRЭрнест БекировNo ratings yet
- Villa C Hanin Town (2068)Document17 pagesVilla C Hanin Town (2068)urquicoreinelNo ratings yet
- PrampDocument6 pagesPrampMihai Ionut TanaseNo ratings yet
- JABINES - PDF 1 1Document1 pageJABINES - PDF 1 1ice iceNo ratings yet
- Ar Gabaldon Annex A 1Document19 pagesAr Gabaldon Annex A 17yd54s95z7No ratings yet
- S-2-1, BasementDocument1 pageS-2-1, BasementKenneth Bryan VillagonezaNo ratings yet
- 4Th Floor 5Th Floor: Meditation CentreDocument1 page4Th Floor 5Th Floor: Meditation CentreRekha TanpureNo ratings yet
- Architectural plans for proposed clinicDocument1 pageArchitectural plans for proposed clinicAnjo Semania100% (1)
- Beam DetailDocument1 pageBeam DetailkbgainsanNo ratings yet
- Building Plans and DrawingsDocument1 pageBuilding Plans and DrawingsJem CapistranoNo ratings yet
- Site Plans ComparisonDocument1 pageSite Plans ComparisonDaniel CryerNo ratings yet
- Architectural Compressed FileDocument4 pagesArchitectural Compressed FileMark jason FuertesNo ratings yet
- (1) LUVAR BTECH-STRUCTURAL-ModelDocument1 page(1) LUVAR BTECH-STRUCTURAL-Modelreynesmarygen9No ratings yet
- Granite Floor 12"x12" 24"x24" (Size To Be Confirmed After Approval of Sample)Document1 pageGranite Floor 12"x12" 24"x24" (Size To Be Confirmed After Approval of Sample)Azkagul 28No ratings yet
- Kesehatan Dan Hak Asasi ManusiaDocument26 pagesKesehatan Dan Hak Asasi ManusiaIndah LusiadiNo ratings yet
- Acute Decompensated Heart Failure: Inpatient ManagementDocument72 pagesAcute Decompensated Heart Failure: Inpatient ManagementparahNo ratings yet
- Malingering Diagnosis Difficult But ImportantDocument6 pagesMalingering Diagnosis Difficult But ImportantparahNo ratings yet
- 8Document7 pages8parahNo ratings yet
- Accuracy of Emphysema Quantification Performed With Reduced Numbers of CT SectionsDocument7 pagesAccuracy of Emphysema Quantification Performed With Reduced Numbers of CT SectionsparahNo ratings yet
- Pi Is 1556086416317786Document2 pagesPi Is 1556086416317786parahNo ratings yet
- PullmoDocument2 pagesPullmoparahNo ratings yet
- Ajr 163 5 7976869Document9 pagesAjr 163 5 7976869parahNo ratings yet
- Otitis MediaDocument6 pagesOtitis MediaririNo ratings yet
- Infantile Lobar Emphysema : OF TWO Cases WithDocument4 pagesInfantile Lobar Emphysema : OF TWO Cases WithparahNo ratings yet
- Pulmonary Emphysema: EpidemiologyDocument4 pagesPulmonary Emphysema: EpidemiologyAnonymous 835s2sxNo ratings yet
- Katalog Astograf PDFDocument2 pagesKatalog Astograf PDFandi lenyNo ratings yet
- Chest and Lungs - Supplementary Handout - Laboratory SessionDocument7 pagesChest and Lungs - Supplementary Handout - Laboratory SessionPaul AculladorNo ratings yet
- Ventilation Techniques Chris ThompsonDocument3 pagesVentilation Techniques Chris Thompsonfalcone87No ratings yet
- Msds Reagen Koh 10%Document6 pagesMsds Reagen Koh 10%Rumah Sakit Bhakti Asih BrebesNo ratings yet
- Introduction To Fitness TrainingDocument25 pagesIntroduction To Fitness TrainingShailendra Singh ChouhanNo ratings yet
- Management of Patient-Ventilator AsynchronyDocument8 pagesManagement of Patient-Ventilator Asynchronyema moralesNo ratings yet
- Cricothyroidotomy and Needle CricothyrotomyDocument10 pagesCricothyroidotomy and Needle CricothyrotomykityamuwesiNo ratings yet
- Lesson Plan BiologyDocument8 pagesLesson Plan BiologyNarasimha SastryNo ratings yet
- Chronic Bronchitis GuideDocument5 pagesChronic Bronchitis GuideJemalyn M. Saludar100% (2)
- 7 - Gas Exchange in HumansDocument7 pages7 - Gas Exchange in HumansTSE UEN SHAN s20181137No ratings yet
- Organs of the Respiratory System FunctionsDocument3 pagesOrgans of the Respiratory System FunctionsEmmeth ArdienteNo ratings yet
- NAME: Nor Fauziatun BT Mohd Fauzi CLASS: 4 Ar-Razi IC NUMBER: 940407-02-5534 Teacher'S NameDocument19 pagesNAME: Nor Fauziatun BT Mohd Fauzi CLASS: 4 Ar-Razi IC NUMBER: 940407-02-5534 Teacher'S NamefauziatunNo ratings yet
- NON-INVASIVE VENTILATION GUIDEDocument1 pageNON-INVASIVE VENTILATION GUIDENicholas HelmstetterNo ratings yet
- Scan 17-Nov-2021Document6 pagesScan 17-Nov-2021Savita AgrawalNo ratings yet
- PTBDocument71 pagesPTBAnonymous 9fLDcZrNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- Explaination: Let'S TalkDocument6 pagesExplaination: Let'S TalkSatriya WibowoNo ratings yet
- Monitoring AnestesiDocument1 pageMonitoring AnestesidianiNo ratings yet
- Physiologic Changes PregnancyDocument53 pagesPhysiologic Changes PregnancyDeedong Zydee100% (1)
- Respiratory SystemDocument57 pagesRespiratory SystemAngelica RevilNo ratings yet