You might also like
- Acute Appendicitis ExplainedDocument63 pagesAcute Appendicitis ExplainedIsis Elektra100% (1)
- Gastroenteritis': Dr. Yanga'S Colleges, IncDocument9 pagesGastroenteritis': Dr. Yanga'S Colleges, IncZyren FuentabellaNo ratings yet
- Bronchial Asthma Case PresentationDocument35 pagesBronchial Asthma Case Presentationbear_pandaNo ratings yet
- PEDIATRIC NURSING HandoutDocument17 pagesPEDIATRIC NURSING HandoutJen Ezel100% (1)
- Case Study of Neurological DisordersDocument10 pagesCase Study of Neurological DisordersSkyerexNo ratings yet
- Nursing Case Study: Managing Bleeding Peptic Ulcer DiseaseDocument39 pagesNursing Case Study: Managing Bleeding Peptic Ulcer DiseaseBESA JERIC FLORESNo ratings yet
- Pediatric Nursing GuideDocument17 pagesPediatric Nursing GuideJem TupazNo ratings yet
- Case PneumoniaDocument29 pagesCase Pneumoniahermesdave1100% (2)
- A Case Study Ovarian New Growth (Mucinous Cystadenomacarcinoma)Document20 pagesA Case Study Ovarian New Growth (Mucinous Cystadenomacarcinoma)HappieSayonara Sardoma Minaves100% (1)
- AGE PPT Case Study 2020Document31 pagesAGE PPT Case Study 2020Marco VelaNo ratings yet
- Pediatric Community Acquired Pneumonia (Pecap) : Case StudyDocument32 pagesPediatric Community Acquired Pneumonia (Pecap) : Case StudyR Hornilla ArcegaNo ratings yet
- Case Study HypertensionDocument5 pagesCase Study HypertensionPaul Jolo100% (10)
- Final Case Study PCAPDocument72 pagesFinal Case Study PCAPKelly Tayag100% (1)
- A Case Study Ovarian New Growth (Mucinous Cystadenomacarcinoma)Document21 pagesA Case Study Ovarian New Growth (Mucinous Cystadenomacarcinoma)HappieSayonara Sardoma MinavesNo ratings yet
- PHYSICAL ASSESSMENT CHILDDocument5 pagesPHYSICAL ASSESSMENT CHILDLarr SumalpongNo ratings yet
- Cerebrovascular Accident: "A Case Study Presentation"Document35 pagesCerebrovascular Accident: "A Case Study Presentation"Kristine YoungNo ratings yet
- Physical Assessment Vitals and FindingsDocument16 pagesPhysical Assessment Vitals and FindingsDaryl Jake FornollesNo ratings yet
- Final Case Study Pcapdocx PDF FreeDocument73 pagesFinal Case Study Pcapdocx PDF FreeZerimar Adawe DulnuanNo ratings yet
- Mrs. Carolyn L. Bote: Clinical InstructorDocument36 pagesMrs. Carolyn L. Bote: Clinical InstructorbearosNo ratings yet
- Case Study - PneumoniaDocument14 pagesCase Study - Pneumonianeil garcia89% (36)
- Physical Examination by DRDocument25 pagesPhysical Examination by DRapi-3739910100% (2)
- Physical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingDocument101 pagesPhysical Examination: Binal Joshi Assistant Professor Child Health Nursing Manikaka Topawala Institute of NursingBinal JoshiNo ratings yet
- Final Case Study PCAPDocument71 pagesFinal Case Study PCAPGabriel Lorenz S. ParongNo ratings yet
- Typhoid Fever Case StudyDocument18 pagesTyphoid Fever Case Studyiurae50% (2)
- Case Study: Periorbital Cellulitis To Consider AbcessDocument11 pagesCase Study: Periorbital Cellulitis To Consider AbcessPriscilla ChantalNo ratings yet
- Case Study SSSSDocument37 pagesCase Study SSSSsplakener100% (1)
- Cerebrovascular Accident 14Document33 pagesCerebrovascular Accident 14japheth01No ratings yet
- Cerebrovascular Accident: AMA Computer Learning CenterDocument33 pagesCerebrovascular Accident: AMA Computer Learning Centerhermesdave1100% (1)
- CASE STUDY On A Nodular Nontoxic GoiterDocument60 pagesCASE STUDY On A Nodular Nontoxic GoiterNiko Montesur100% (4)
- Cesarean Section 2ndary To Fetal Distress Case PresentationDocument72 pagesCesarean Section 2ndary To Fetal Distress Case PresentationMhaii Ameril100% (1)
- Cerebrovascular Accident: "A Case Study Presentation"Document38 pagesCerebrovascular Accident: "A Case Study Presentation"Kristine YoungNo ratings yet
- Phinma Cagayan de Oro CollegeDocument14 pagesPhinma Cagayan de Oro CollegeYasmin MagsaysayNo ratings yet
- 2nd PartDocument20 pages2nd PartChristine PicardalNo ratings yet
- Repeat Case Breech 1Document73 pagesRepeat Case Breech 1Francis MendozaNo ratings yet
- Bronchial Asthma Case StudyDocument16 pagesBronchial Asthma Case StudyMOLINA, TANJA JAYNENo ratings yet
- A Case Study ON Pneumonia: Panpacific University North PhilippinesDocument13 pagesA Case Study ON Pneumonia: Panpacific University North PhilippinesAbdalrahman AhmedNo ratings yet
- Case PresentationDocument50 pagesCase Presentationapi-19762967No ratings yet
- Acute Renal FailureDocument16 pagesAcute Renal Failuresantosh kumarNo ratings yet
- Pa NephroticDocument7 pagesPa NephroticPaola CamainNo ratings yet
- Dengue Fever Case StudyDocument24 pagesDengue Fever Case Studymaemaeyee95% (22)
- Case Presentation in Geriatric Ward "Cancer of The Larynx"Document130 pagesCase Presentation in Geriatric Ward "Cancer of The Larynx"Christina GutierrezNo ratings yet
- A Case Study: AnemiaDocument25 pagesA Case Study: AnemiaDiana Marie Magango FranciaNo ratings yet
- Postpartal Perineal Pain Case StudyDocument64 pagesPostpartal Perineal Pain Case Studymharz_astilloNo ratings yet
- Thu, February 12, 2009 2:16:53 PM Ito N Ung 4mat ... : Physical Assessment General Survey: Appearance and Mental StatusDocument10 pagesThu, February 12, 2009 2:16:53 PM Ito N Ung 4mat ... : Physical Assessment General Survey: Appearance and Mental StatusTheresa de JesusNo ratings yet
- Case Study On Meninomyocele (Repaired) PDocument29 pagesCase Study On Meninomyocele (Repaired) Pcharanjit kaur100% (1)
- Case Study Acute Urinary RetentionDocument10 pagesCase Study Acute Urinary RetentionYasmin MagsaysayNo ratings yet
- In Partial Fulfillment of The Final Requirements in Advanced Health Assessment MSN 205Document13 pagesIn Partial Fulfillment of The Final Requirements in Advanced Health Assessment MSN 205Gummie Akalal SugalaNo ratings yet
- NCM101 Collection of Objective Data (Validation of Data)Document50 pagesNCM101 Collection of Objective Data (Validation of Data)Roland100% (1)
- Sections of Health History: ExaminationDocument4 pagesSections of Health History: ExaminationMhelrose JornalesNo ratings yet
- NCM101J - Nursing Health Assessment - Week 3Document31 pagesNCM101J - Nursing Health Assessment - Week 3Jenny Ruth TubanNo ratings yet
- The Basics: A Comprehensive Outline of Nursing School ContentFrom EverandThe Basics: A Comprehensive Outline of Nursing School ContentRating: 5 out of 5 stars5/5 (3)
- Restore Hearing Naturally: How to Use Your Inner Resources to Bring Back Full HearingFrom EverandRestore Hearing Naturally: How to Use Your Inner Resources to Bring Back Full HearingNo ratings yet
- Is Your Pet Safe?: Morgellon's Disease-A New Parasitic Disease May Be Transmitted by PetsFrom EverandIs Your Pet Safe?: Morgellon's Disease-A New Parasitic Disease May Be Transmitted by PetsNo ratings yet
- Unlocking the Ancient Secrets to Healing: Why Science is Looking to the Past for the Future of MedicineFrom EverandUnlocking the Ancient Secrets to Healing: Why Science is Looking to the Past for the Future of MedicineRating: 5 out of 5 stars5/5 (2)
- Tinnitus Stop!: The Complete Guide On Ringing In The Ears, Natural Tinnitus Remedies, And A Holistic System For Permanent Tinnitus ReliefFrom EverandTinnitus Stop!: The Complete Guide On Ringing In The Ears, Natural Tinnitus Remedies, And A Holistic System For Permanent Tinnitus ReliefRating: 5 out of 5 stars5/5 (1)
- The Other Side of the Valley: Healing Through Altered States of ConsciousnessFrom EverandThe Other Side of the Valley: Healing Through Altered States of ConsciousnessNo ratings yet
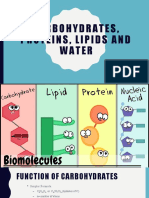
- Lesson 2 - Water, CarbohydratesDocument22 pagesLesson 2 - Water, CarbohydratesDon'tAsK TheStupidOnesNo ratings yet
- For Portfolio LS1 EnglishDocument5 pagesFor Portfolio LS1 EnglishDon'tAsK TheStupidOnesNo ratings yet
- For Portfolio LS2 ScienceDocument7 pagesFor Portfolio LS2 ScienceDon'tAsK TheStupidOnesNo ratings yet
- For Portfolio LS6 Digital CitizenshipDocument4 pagesFor Portfolio LS6 Digital CitizenshipDon'tAsK TheStupidOnesNo ratings yet
- For Portfolio LS3 Mathematical and Problem Solving SkillsDocument8 pagesFor Portfolio LS3 Mathematical and Problem Solving SkillsDon'tAsK TheStupidOnesNo ratings yet
- Biology BasicsDocument5 pagesBiology BasicsDon'tAsK TheStupidOnesNo ratings yet
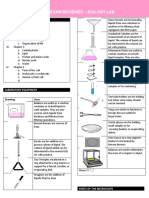
- Prelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Document7 pagesPrelim Exam Reviewer - Biology Lab: by Team Meow Meow (Halimeow and 3 Headed Creature)Don'tAsK TheStupidOnesNo ratings yet
- Welcome General Chemistry For Engineering and TechnologistDocument9 pagesWelcome General Chemistry For Engineering and TechnologistDon'tAsK TheStupidOnesNo ratings yet
- Principles of Biology I Lab ManualDocument75 pagesPrinciples of Biology I Lab ManualDon'tAsK TheStupidOnesNo ratings yet
- Cross WordDocument1 pageCross WordDon'tAsK TheStupidOnesNo ratings yet
- Crystal Structure Quiz: Name: - DateDocument1 pageCrystal Structure Quiz: Name: - DateDon'tAsK TheStupidOnesNo ratings yet
- Crystal Structure Quiz: Name: - DateDocument1 pageCrystal Structure Quiz: Name: - DateDon'tAsK TheStupidOnesNo ratings yet
- Quiz 1-ChemDocument2 pagesQuiz 1-ChemDon'tAsK TheStupidOnesNo ratings yet
- Quiz 2 - ChemDocument3 pagesQuiz 2 - ChemDon'tAsK TheStupidOnesNo ratings yet
- Pathophysiology of TuberculosisDocument1 pagePathophysiology of TuberculosisDon'tAsK TheStupidOnesNo ratings yet
- Family Life Cycle StagesDocument2 pagesFamily Life Cycle StagesDon'tAsK TheStupidOnes100% (1)
- Global Warming: Public Health Impacts and SolutionsDocument45 pagesGlobal Warming: Public Health Impacts and SolutionsDon'tAsK TheStupidOnesNo ratings yet
- EF2017 FinalDigital PDFDocument20 pagesEF2017 FinalDigital PDFHieuNo ratings yet
- Gibbs WorksheetDocument4 pagesGibbs WorksheetDon'tAsK TheStupidOnesNo ratings yet
- Internal energy problems solutionsDocument3 pagesInternal energy problems solutionsDon'tAsK TheStupidOnesNo ratings yet
- KEY Nuclear EquationsDocument3 pagesKEY Nuclear EquationsDon'tAsK TheStupidOnesNo ratings yet
- Hess's Law Problems SolvedDocument2 pagesHess's Law Problems SolvedTjrjfjdjNo ratings yet
- Bomb Calorimetry Practice ProblemsDocument2 pagesBomb Calorimetry Practice ProblemsDon'tAsK TheStupidOnesNo ratings yet
- Calorimetry Problems KeyDocument2 pagesCalorimetry Problems KeyDon'tAsK TheStupidOnesNo ratings yet
- Comparison Between Piezoelectric and Magnetic PDFDocument6 pagesComparison Between Piezoelectric and Magnetic PDFDon'tAsK TheStupidOnesNo ratings yet
- IntrodutionDocument21 pagesIntrodutionDon'tAsK TheStupidOnesNo ratings yet
- Specific Heat ProblemsDocument4 pagesSpecific Heat ProblemskhenNo ratings yet
- Community Health Nursing Review (Edited)Document407 pagesCommunity Health Nursing Review (Edited)api-2658787991% (35)
- Nursing Review BulletsDocument125 pagesNursing Review BulletsROBERT C. REÑA, BSN, RN, MAN (ue)96% (46)
- Community Health Nursing: I - Definition of TermsDocument25 pagesCommunity Health Nursing: I - Definition of TermsRichard Ines Valino97% (29)
- Operative SurgeryDocument119 pagesOperative SurgerySubhrajyoti Banerjee100% (2)
- Bone Surface MarkingsDocument2 pagesBone Surface MarkingsNurul Afiqah Fattin AmatNo ratings yet
- Urinary Elimination: Lesson 5eDocument33 pagesUrinary Elimination: Lesson 5eMikhaela Andree MarianoNo ratings yet
- Harrison's Endocrinology 4th Ed (2017) (PDF)Document610 pagesHarrison's Endocrinology 4th Ed (2017) (PDF)Sergiu97% (30)
- Rolf HingesDocument8 pagesRolf Hingeswalterego58100% (3)
- Embryology of Respiratory System NotesDocument3 pagesEmbryology of Respiratory System NotesJulienne Sanchez-SalazarNo ratings yet
- Dr. A. Samy TAG Surgical Approaches - 1Document7 pagesDr. A. Samy TAG Surgical Approaches - 1gehadbeddaNo ratings yet
- Steps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-StepDocument9 pagesSteps in The Synthesis and Secretion of Thyroid Hormone: Process Diagrams Step-by-Steprambabs369No ratings yet
- Space Regainer 2Document12 pagesSpace Regainer 2rahmadhanidianNo ratings yet
- Manual Nervous SystemDocument6 pagesManual Nervous SystemVynz Morales CosepNo ratings yet
- CVSDocument58 pagesCVSDoina SvetNo ratings yet
- 11.3 Neurons - Biology LibreTextsDocument3 pages11.3 Neurons - Biology LibreTextsDandy MarayagNo ratings yet
- Lower Limbs MCQs Section 1 TitleDocument148 pagesLower Limbs MCQs Section 1 TitleCaim ZNo ratings yet
- Clinical Voice 28 PaginasDocument28 pagesClinical Voice 28 PaginasCarlos CarrascoNo ratings yet
- Derived Position - IDocument30 pagesDerived Position - IPONMATHI P FACULTY OF PHYSIOTHERAPYNo ratings yet
- Inner Smile and Six Healing Sounds PracticeDocument12 pagesInner Smile and Six Healing Sounds Practiceghulam ali100% (1)
- ANATOMY AND PHYSIOLOGY (Muscular System)Document2 pagesANATOMY AND PHYSIOLOGY (Muscular System)Gwyn Louise CarolinoNo ratings yet
- 4sb Reflex InfographicDocument1 page4sb Reflex Infographicvombyandi100% (1)
- Chapter 8Document60 pagesChapter 8enewaw sabawNo ratings yet
- Cat Dissection GuideDocument46 pagesCat Dissection GuideShelomi GerdanNo ratings yet
- Urinary SystemDocument27 pagesUrinary SystemNicole LamNo ratings yet
- Circulatory System PPT 1Document47 pagesCirculatory System PPT 1Czarae VillanuevaNo ratings yet
- Headgear and Its MechanicsDocument10 pagesHeadgear and Its MechanicsDharaniNo ratings yet
- Endocrine GlandsDocument9 pagesEndocrine Glandstadashii100% (1)
- Thyrotoxicosis: Giridhar MF 9 TermDocument19 pagesThyrotoxicosis: Giridhar MF 9 TermGiridhar MFNo ratings yet
- Neck Training For Wrestlers-ClientDocument104 pagesNeck Training For Wrestlers-ClientIvan Medić100% (2)
- Physical Education's Health BenefitsDocument67 pagesPhysical Education's Health BenefitsAlejandro Francisco Jr.No ratings yet
- Ischemic Stroke Pathophysiology and Principles of Localization (1) G PDFDocument16 pagesIschemic Stroke Pathophysiology and Principles of Localization (1) G PDFGina Ayudia PutriNo ratings yet
- L3Rds: Jhigo Pascual I-19: Video AudioDocument4 pagesL3Rds: Jhigo Pascual I-19: Video AudioJhigo Villar Franco PascualNo ratings yet
- Muscles of The EyeDocument3 pagesMuscles of The EyeAnna GarbiNo ratings yet