You might also like
- American Red CrossDocument484 pagesAmerican Red CrossAngelika LowderNo ratings yet
- ASCP ExamDocument10 pagesASCP Examnoone100% (3)
- Surgery OsceDocument69 pagesSurgery OsceRebecca BrandonNo ratings yet
- Fraud Investigation and Medical Audit ManualDocument68 pagesFraud Investigation and Medical Audit Manualneetu singhNo ratings yet
- Skeletal Muscle Tissue & Muscle OrganizationDocument90 pagesSkeletal Muscle Tissue & Muscle Organizationtiiandi100% (3)
- Cognitive Remediation Therapy For Anorexia Nervosa Kate TchanturaDocument156 pagesCognitive Remediation Therapy For Anorexia Nervosa Kate TchanturaIndriNo ratings yet
- The Full Gaps DietDocument9 pagesThe Full Gaps Dietalina4891100% (1)
- Assisting in Nasogastric Tube Insertion 1 1Document14 pagesAssisting in Nasogastric Tube Insertion 1 1Princess Faniega SugatonNo ratings yet
- Common Respiratory InterventionsDocument10 pagesCommon Respiratory InterventionsAngel Joy CatalanNo ratings yet
- Line and TubesDocument18 pagesLine and Tubespaulzilicous.artNo ratings yet
- Assisting in Nasogastric Tube InsertionDocument11 pagesAssisting in Nasogastric Tube InsertionJan Federick BantayNo ratings yet
- NG Tube IntubationDocument40 pagesNG Tube IntubationVed BratNo ratings yet
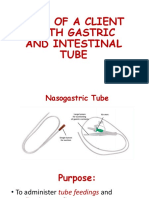
- Objectives: at The End of The Discussion The Students Will Be Able ToDocument6 pagesObjectives: at The End of The Discussion The Students Will Be Able ToMichael Angelo SeñaNo ratings yet
- .archNG - Parenteral NutritionDocument77 pages.archNG - Parenteral NutritionBidhya GuptaNo ratings yet
- Drains Tubes CathetersDocument56 pagesDrains Tubes CathetersFrancess Dane CobradoNo ratings yet
- Tracheostomy Care SkillsDocument8 pagesTracheostomy Care Skillshoangt2002No ratings yet
- Blakemore TubingDocument3 pagesBlakemore Tubingl_m_pacheco100% (1)
- NGT Insertion 2022Document41 pagesNGT Insertion 2022Krishna Faith P. DelaraNo ratings yet
- Fundamental Nsg-IiDocument46 pagesFundamental Nsg-IiabiyotNo ratings yet
- Gastric LavageDocument13 pagesGastric Lavagetibinj67No ratings yet
- The Respiratory SystemDocument40 pagesThe Respiratory SystemAdriana ChasiguanoNo ratings yet
- NG Tube InsertionDocument37 pagesNG Tube InsertionSarah BirechNo ratings yet
- Nasogastric Tube NGT 1215082454278959 8Document107 pagesNasogastric Tube NGT 1215082454278959 8Raquel M. MendozaNo ratings yet
- NG Tube Lictures 2023Document22 pagesNG Tube Lictures 2023ALi NursingNo ratings yet
- NGTDocument36 pagesNGTAstrid Bernadette Ulina PurbaNo ratings yet
- ENEMADocument53 pagesENEMAJocel Mae OrtegaNo ratings yet
- Day 5 Lecture - GI and NutritionDocument65 pagesDay 5 Lecture - GI and NutritionRemej SilutgamNo ratings yet
- Administering An EnemaDocument13 pagesAdministering An EnemaNai DhavalNo ratings yet
- TRACHEOSTOMTPRESENTATIONDocument37 pagesTRACHEOSTOMTPRESENTATIONStar AcademyNo ratings yet
- EnemaDocument48 pagesEnemaPrajna TiwariNo ratings yet
- Enema 5Document22 pagesEnema 5meseretNo ratings yet
- NGT Insertion: Group 2 Guerrero, Gumatay, Lim, Lopez, Mallabo, Miñano, Nario, Olores, Paaño, Pajutan, Paz, PerezDocument19 pagesNGT Insertion: Group 2 Guerrero, Gumatay, Lim, Lopez, Mallabo, Miñano, Nario, Olores, Paaño, Pajutan, Paz, PerezHarlyn MagsinoNo ratings yet
- NGT Feeding and Meds Administration Via NGTDocument25 pagesNGT Feeding and Meds Administration Via NGTPaul Michael BaguhinNo ratings yet
- Gastrostomy Feeding ProcedureDocument5 pagesGastrostomy Feeding ProcedureRohini RaiNo ratings yet
- Module 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Document18 pagesModule 3 Nursing Skills Procedure On GI, Endo-Metab Concept (A)Nashebah A. BatuganNo ratings yet
- Chest Tube, Urinary Catheter, Ryles Tube InsertionDocument60 pagesChest Tube, Urinary Catheter, Ryles Tube InsertionMohd Johari Mohd ShafuwanNo ratings yet
- Tracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HDocument74 pagesTracheostomy Care: Presented by Sital B. Sharma M SC Nursing Student College of Nursing. N.B.M.C.HShetal Sharma100% (1)
- Care in Palliative Care Care in Palliative CareDocument12 pagesCare in Palliative Care Care in Palliative CareminaranabhatNo ratings yet
- NG and Foley Cath M2 2009Document54 pagesNG and Foley Cath M2 2009aditi268100% (1)
- Promoting Nutrition (Enteral Nutrition)Document51 pagesPromoting Nutrition (Enteral Nutrition)Yayin Pestaño100% (1)
- NCM 109 Rle Retdems Rational MidtermsDocument35 pagesNCM 109 Rle Retdems Rational MidtermsemilynbernatNo ratings yet
- Oro & Nasopharyngeal SuctioningDocument16 pagesOro & Nasopharyngeal SuctioningHERLIN HOBAYANNo ratings yet
- Gastric LavageDocument11 pagesGastric LavageJay Villasoto100% (3)
- Providing Special CareDocument23 pagesProviding Special CareJan LagriaNo ratings yet
- Urinary-Catheterization (1)Document31 pagesUrinary-Catheterization (1)hazel jamisNo ratings yet
- NGT FeedingDocument19 pagesNGT FeedingzhaimeangirlNo ratings yet
- Nursing Procedures 2003Document11 pagesNursing Procedures 2003jackson2494100% (1)
- Nyoman Purwadi: Divisi Gastro-Hepatology Sanglah HospitalDocument17 pagesNyoman Purwadi: Divisi Gastro-Hepatology Sanglah HospitalMuhammad RamadhanNo ratings yet
- DRAINS.-WPS OfficeDocument14 pagesDRAINS.-WPS OfficeIsaac ayobamiNo ratings yet
- Nasogastric Tube (Ryle)Document1 pageNasogastric Tube (Ryle)AAGKhatriNo ratings yet
- FundamentalsDocument34 pagesFundamentalsColleen CalditoNo ratings yet
- Nasogastric TubeDocument25 pagesNasogastric Tubekayse abtidoonNo ratings yet
- Care of Clients With Chest TubeDocument55 pagesCare of Clients With Chest TubeMarc Andreo MalalaNo ratings yet
- Care of Patient With: Chest DrainageDocument29 pagesCare of Patient With: Chest DrainageMSc. PreviousNo ratings yet
- 3 Gastrointestinal IntubationsDocument19 pages3 Gastrointestinal IntubationsmegbriansularteNo ratings yet
- Medicine InstrumentsDocument89 pagesMedicine Instrumentsvinaynagar1994No ratings yet
- Tracheostomy SlidesDocument24 pagesTracheostomy SlidesMohammed AdamNo ratings yet
- Airway Management For ParamedicsDocument53 pagesAirway Management For ParamedicsNataliya PiletskaNo ratings yet
- Fundamentals of NursingDocument42 pagesFundamentals of NursingFrancis James RigodonNo ratings yet
- Nasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdDocument32 pagesNasogastric Intubation: DR - Efman.E.U.Manawan Mkes.,Spb-KbdBilly PeterNo ratings yet
- NGT Feeding Discussion InotDocument2 pagesNGT Feeding Discussion InotRhenelyn Delos ReyesNo ratings yet
- احمد كريمDocument12 pagesاحمد كريمMr. abbas fahim hamidNo ratings yet
- Objectives: Intestinal Tube InsertionDocument28 pagesObjectives: Intestinal Tube Insertion2013SecBNo ratings yet
- Inserting A Nasogastric TubeDocument5 pagesInserting A Nasogastric TubeWendy EscalanteNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Week 9Document3 pagesWeek 9api-530814583No ratings yet
- Week 10Document3 pagesWeek 10api-530814583No ratings yet
- Week 8Document3 pagesWeek 8api-530814583No ratings yet
- Week 5Document3 pagesWeek 5api-530814583No ratings yet
- Week 7Document3 pagesWeek 7api-530814583No ratings yet
- Week 4Document3 pagesWeek 4api-530814583No ratings yet
- Week 2Document3 pagesWeek 2api-530814583No ratings yet
- Extra WeekDocument3 pagesExtra Weekapi-530814583No ratings yet
- Week 3Document2 pagesWeek 3api-530814583No ratings yet
- Week 1Document1 pageWeek 1api-530814583No ratings yet
- Remediation 480Document2 pagesRemediation 480api-530814583No ratings yet
- Effectiveness of Using Contraceptives of The TeenagersDocument9 pagesEffectiveness of Using Contraceptives of The TeenagersQUEDDENG, CLYDE WALTER D.No ratings yet
- 10 Commandments of ConsultationDocument4 pages10 Commandments of ConsultationZlatan KurjakovicNo ratings yet
- Rustom A. Velila BSED 3204Document4 pagesRustom A. Velila BSED 3204Ella CustodioNo ratings yet
- Medical Surgical Nursing MCQsDocument4 pagesMedical Surgical Nursing MCQssivakamasundari pichaipillai90% (10)
- Consti and Juris Cases Compilation 3Document169 pagesConsti and Juris Cases Compilation 3MG DangtayanNo ratings yet
- Go Go Go First Vita PlusDocument6 pagesGo Go Go First Vita PlusArnulfo Yu LanibaNo ratings yet
- Anemia of Chronic DiseaseDocument20 pagesAnemia of Chronic DiseaseAryeswaraNo ratings yet
- PHARMA 06. Introduction To Autonomic PharmacologyDocument6 pagesPHARMA 06. Introduction To Autonomic PharmacologyCindy Mae MacamayNo ratings yet
- Fundamentals of Molecular Virology 2Nd Edition Acheson Test Bank Full Chapter PDFDocument29 pagesFundamentals of Molecular Virology 2Nd Edition Acheson Test Bank Full Chapter PDFdanielaidan4rf7100% (10)
- 23 Levin Et Al-1977-Journal of Oral Pathology & MedicineDocument10 pages23 Levin Et Al-1977-Journal of Oral Pathology & Medicineshir keshalesNo ratings yet
- FormaldehydeDocument14 pagesFormaldehydeSalman AshrafNo ratings yet
- Peran Keluarga Pada Kepatuhan Minum Obat Penderita TB Di Kawedanan Pedan KlatenDocument10 pagesPeran Keluarga Pada Kepatuhan Minum Obat Penderita TB Di Kawedanan Pedan KlatenDede Yusuf HatamiNo ratings yet
- Antimicrobial AssayDocument14 pagesAntimicrobial AssayArvin GerlabanNo ratings yet
- Psychological Support For People Living With HIV: Report: July 2010Document28 pagesPsychological Support For People Living With HIV: Report: July 2010Ikponmwosa EseosaNo ratings yet
- Ass 1Document14 pagesAss 1Kenneth WongNo ratings yet
- BELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Document69 pagesBELIZARIO VY Et Al Medical Parasitology in The Philippines 3e 158 226Sharon Agor100% (1)
- Dog Incontinence - An Incontinent Dog Dry and Treat Urine ScaldDocument28 pagesDog Incontinence - An Incontinent Dog Dry and Treat Urine ScaldJerome SiegelNo ratings yet
- Introduction To Preventive and Community MedicineDocument2 pagesIntroduction To Preventive and Community MedicineMonsour SalazarNo ratings yet
- DRUG STUDY Ft. RanitidineDocument4 pagesDRUG STUDY Ft. RanitidinePao LaurenteNo ratings yet
- Aesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinDocument7 pagesAesthetic Durable Forehead Contouring in Asians With Fat Grafting and Botulinum ToxinAnonymous LnWIBo1GNo ratings yet
- Mock Exam (November 2018) Biology Paper 2: HKDSE BIOLOGY-Concepts and ApplicationsDocument10 pagesMock Exam (November 2018) Biology Paper 2: HKDSE BIOLOGY-Concepts and ApplicationsStevenson DavidNo ratings yet
- دورة هامة في التحاليل الطبية PDFDocument308 pagesدورة هامة في التحاليل الطبية PDFkigm mkjNo ratings yet
- Q1 Sci9 Mod7Document18 pagesQ1 Sci9 Mod7Regine Rafer EscalanteNo ratings yet
- Chapter 7 CELL STRUCTURE AND FUNCTION PDFDocument16 pagesChapter 7 CELL STRUCTURE AND FUNCTION PDFAngelene PelayoNo ratings yet