You might also like
- Arahan Pegawai Pengawal KPM 2011Document23 pagesArahan Pegawai Pengawal KPM 2011Mat Yie Mat NorNo ratings yet
- 2017 Instrumen Pemantauan Perkhidmatan Kawalan KeselamatanDocument4 pages2017 Instrumen Pemantauan Perkhidmatan Kawalan KeselamatanArudin Duali100% (1)
- Senarai Nombor Telefon KecemasanDocument1 pageSenarai Nombor Telefon KecemasanQru Walid E ZuziinshadNo ratings yet
- Pengurusan Risiko Sekolah-Sekolah SelangorDocument178 pagesPengurusan Risiko Sekolah-Sekolah SelangorENCIK MOHD SAHARI SAYUTI BIN ARIFIN (B-PPDGOMBAK)100% (1)
- Borang Maklumat Ko Kurikulum Dan Kad 001Document2 pagesBorang Maklumat Ko Kurikulum Dan Kad 001fardahahmadNo ratings yet
- Kategori 3Document8 pagesKategori 3liewboonchun5258No ratings yet
- Anjakan 5Document2 pagesAnjakan 5Noor Badariah100% (1)
- Borang Senarai Semakan Pengauditan Penguruasan KewanganDocument8 pagesBorang Senarai Semakan Pengauditan Penguruasan KewanganBaharin AzizNo ratings yet
- Borang Laporan Kemajuan Pelajar - PPPDocument3 pagesBorang Laporan Kemajuan Pelajar - PPPPERLIS-CM44 MoeNo ratings yet
- Senarai Semak File Ppki Tahun 2022Document4 pagesSenarai Semak File Ppki Tahun 2022nur atirah100% (1)
- Garis Panduan Interim Versi 2.0Document13 pagesGaris Panduan Interim Versi 2.0Anonymous zDHBZstCNo ratings yet
- Final - Pelan Tindakan NCR Iso 14001 UpmDocument4 pagesFinal - Pelan Tindakan NCR Iso 14001 Upmmr5jalNo ratings yet
- Laporan Biro Kokurikulum 2016Document5 pagesLaporan Biro Kokurikulum 2016casbenxNo ratings yet
- Lampiran B-Borang Permohonan Jawatan Kader PPP KPMDocument3 pagesLampiran B-Borang Permohonan Jawatan Kader PPP KPMAhmad Syahril AyobNo ratings yet
- Borang Instrumen Pemantauan DisiplinDocument5 pagesBorang Instrumen Pemantauan DisiplinfairousismailNo ratings yet
- PiNTAS Dan OPPPM (SLT Dan MLT) SK KOPURONDocument16 pagesPiNTAS Dan OPPPM (SLT Dan MLT) SK KOPURONZulfazly RashidNo ratings yet
- HM01 PengetuaDocument8 pagesHM01 PengetuaAHMAD NZRYSHAH BIN MOHAMED KHALID MoeNo ratings yet
- LNPT SokIIDocument10 pagesLNPT SokIIpaan1187No ratings yet
- Garis Panduan Pengurusan Mesyuarat Dan Penulisan Minit MesyuaratDocument32 pagesGaris Panduan Pengurusan Mesyuarat Dan Penulisan Minit Mesyuaratalagan79No ratings yet
- JPS - SPK-PPDa.02 Instrumen Pemantauan Pengurusan PPDa Di SekolahDocument3 pagesJPS - SPK-PPDa.02 Instrumen Pemantauan Pengurusan PPDa Di Sekolahskbbs2100% (1)
- 02 Dasar Dan Ketetapan KurikulumDocument34 pages02 Dasar Dan Ketetapan KurikulumCikgu AlNo ratings yet
- Garis Panduan Interim Julai 2019 Versi 3.1Document20 pagesGaris Panduan Interim Julai 2019 Versi 3.1شهريلميسلن100% (1)
- Isu ApdmDocument46 pagesIsu ApdmYamunavathy Ponnusamy100% (1)
- Borang Pengesahan Perkhidmatan KBK Bagi Kontrak Yang Berkuat Kuasa Mulai 1 April 2022Document11 pagesBorang Pengesahan Perkhidmatan KBK Bagi Kontrak Yang Berkuat Kuasa Mulai 1 April 2022SJK(C) AI CHUN (SEK-JBC7001)No ratings yet
- CutiDocument199 pagesCutisyahid100% (1)
- Pk12 Pengurusan Kawalan Dokumen Dan Rekod Kualiti 1Document11 pagesPk12 Pengurusan Kawalan Dokumen Dan Rekod Kualiti 1norhanitamohamadNo ratings yet
- Item Penilaian Pibg CemerlangDocument22 pagesItem Penilaian Pibg CemerlangSiti Nur Farihan ShamsuddinNo ratings yet
- Surat Jemputan Jururawat Program TransisiDocument1 pageSurat Jemputan Jururawat Program TransisipakyusNo ratings yet
- Surat Memperkasakan Intervensi Sekolah Feeder - 14.9.2023Document2 pagesSurat Memperkasakan Intervensi Sekolah Feeder - 14.9.2023MOHD SHUKRI SAMSUNo ratings yet
- 2013pengurusan Keselamatan MuridDocument58 pages2013pengurusan Keselamatan MuridLutfi BiharNo ratings yet
- Format Laporan KBK-PKKDocument6 pagesFormat Laporan KBK-PKKShaheer WazirNo ratings yet
- KWS KWK KwaDocument3 pagesKWS KWK Kwapdb1623No ratings yet
- Instrumen Pemantauan 1M 1S JPN JohorDocument5 pagesInstrumen Pemantauan 1M 1S JPN Johormrdan100% (1)
- Kertas Kerja WAWASAN DESADocument8 pagesKertas Kerja WAWASAN DESAYoyoball BallNo ratings yet
- Panduan Penyediaan Fail Rekod Pensyarah: Politeknik MukahDocument32 pagesPanduan Penyediaan Fail Rekod Pensyarah: Politeknik MukahHeidi KingNo ratings yet
- Borang Keberhasil 2020Document3 pagesBorang Keberhasil 2020Siti Rodiah Abdul AzizNo ratings yet
- Tugasan Individu Wajib Modul 2 (Esei) LatestDocument15 pagesTugasan Individu Wajib Modul 2 (Esei) LatestJennifer JohnsonNo ratings yet
- Borang Pemantauan KK (Baru)Document12 pagesBorang Pemantauan KK (Baru)Zuraidah Binti Ahmat100% (1)
- Carta Alir Kes Tatatertib BiasaDocument2 pagesCarta Alir Kes Tatatertib BiasaGURU BESAR SJK(C) CHUEN MINNo ratings yet
- Borang Data Murid Ponteng Sekolah RendahDocument1 pageBorang Data Murid Ponteng Sekolah RendahTing Suk HeeNo ratings yet
- Slide Ippi 30 Jun 2022 - EditedDocument39 pagesSlide Ippi 30 Jun 2022 - Editedbala jayaNo ratings yet
- Senarai Semak Tuntutan Pelarasan Bantuan Persekolahan 2021Document1 pageSenarai Semak Tuntutan Pelarasan Bantuan Persekolahan 2021NORAZIAN ARIPNo ratings yet
- PGB Garis Panduan Undangan Orang Kenamaan Dan Ahli Politik 1Document19 pagesPGB Garis Panduan Undangan Orang Kenamaan Dan Ahli Politik 1Abdul Hadi TurmidiNo ratings yet
- Penubuhan Dan Pengurusan Kelab, Persatuan, Ub BeruniformDocument60 pagesPenubuhan Dan Pengurusan Kelab, Persatuan, Ub BeruniformStanley Stewart Peter100% (1)
- 1 Penerimaan Wang Sekolah 08Document41 pages1 Penerimaan Wang Sekolah 08tiiannNo ratings yet
- Carta Fungsi Sekolah KPMDocument2 pagesCarta Fungsi Sekolah KPMMiraa IxoraaNo ratings yet
- Borang Pengisytiharan Kesihatan MuridDocument1 pageBorang Pengisytiharan Kesihatan MuridJeNo ratings yet
- Borang Isytihar KesihatanDocument2 pagesBorang Isytihar KesihatanRyan KubalNo ratings yet
- Borang Akuan KesihatanDocument2 pagesBorang Akuan KesihatanharisfaizalNo ratings yet
- Borang Isytihar KesihatanDocument1 pageBorang Isytihar KesihatanFitri RazakNo ratings yet
- Borang Saringan V3Document1 pageBorang Saringan V3Assraff ReaduanNo ratings yet
- Borang - SKCPM 2021 - Pelajar Dan IbubapaDocument3 pagesBorang - SKCPM 2021 - Pelajar Dan IbubapaafnijeNo ratings yet
- Borang Deklarasi Kesihatan MuridDocument1 pageBorang Deklarasi Kesihatan MuridRAMLAH BINTI MOHAMED JAMLI PPDSNo ratings yet
- Borang Deklarasi Kesihatan Asrama 2021Document1 pageBorang Deklarasi Kesihatan Asrama 2021Aiman IrfanNo ratings yet
- 04 Borang Akuan Pengisytiharan Kesihatan MuridDocument1 page04 Borang Akuan Pengisytiharan Kesihatan MuridSabree SeninNo ratings yet
- LAMPIRAN 5 - Isytihar Kesihatan Pekerja - Guru & PPMDocument1 pageLAMPIRAN 5 - Isytihar Kesihatan Pekerja - Guru & PPMM Badrul HisamNo ratings yet
- Rekod Kesihatan PDFDocument4 pagesRekod Kesihatan PDFRuzaifah ZyNo ratings yet
- Rekod KesihatanDocument4 pagesRekod KesihatanHadiah HazemiNo ratings yet
- Borang Istihar Kesihatan MBKDocument3 pagesBorang Istihar Kesihatan MBKfridlyNo ratings yet
- 3 Borang Pengesahan Kesihatan MFLSDocument1 page3 Borang Pengesahan Kesihatan MFLStenang10No ratings yet
- Amali Solat BerjemaahDocument13 pagesAmali Solat BerjemaahnursyahzananiNo ratings yet
- Pengesahan Lapor Diri PelajarDocument1 pagePengesahan Lapor Diri PelajarnursyahzananiNo ratings yet
- 7-Borang Pendaftaran Barangan Elektrik (Usas)Document1 page7-Borang Pendaftaran Barangan Elektrik (Usas)nursyahzananiNo ratings yet
- Hiasan Landskap Kos RendahDocument5 pagesHiasan Landskap Kos RendahnursyahzananiNo ratings yet
- 9-Borang Keahlian Perpustakaan (2) (USAS) PDFDocument1 page9-Borang Keahlian Perpustakaan (2) (USAS) PDFnursyahzanani100% (2)
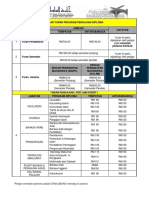
- 3-KADAR YURAN DAN BAYARAN YURAN JOMPAY (Diploma)Document2 pages3-KADAR YURAN DAN BAYARAN YURAN JOMPAY (Diploma)nursyahzananiNo ratings yet
- 6-Borang Permohonan Kediaman PelajarDocument2 pages6-Borang Permohonan Kediaman PelajarnursyahzananiNo ratings yet