You might also like
- Parental Consent: Department of EducationDocument13 pagesParental Consent: Department of EducationShure XioNo ratings yet
- Letter of Intent To Transfer: Rinalyn J. JintalanDocument1 pageLetter of Intent To Transfer: Rinalyn J. JintalanRinalynNo ratings yet
- Weekly Accomplishment ReportDocument10 pagesWeekly Accomplishment ReportMa. Victoria LlameraNo ratings yet
- Sample Monthly Technical Assistance Plan For School HeadsDocument5 pagesSample Monthly Technical Assistance Plan For School HeadsJosevi Dela Torre MacasNo ratings yet
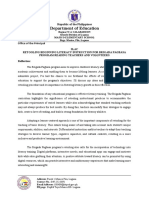
- Retooling Beginning Literacy Instruction For The Brigada Pagbasa Program-ReflectionDocument2 pagesRetooling Beginning Literacy Instruction For The Brigada Pagbasa Program-ReflectionCarmela BancaNo ratings yet
- Department of Education: Republic of The PhilippinesDocument22 pagesDepartment of Education: Republic of The PhilippinesSheryl Cruz EspirituNo ratings yet
- LAC Session Evaluation ToolDocument2 pagesLAC Session Evaluation ToolRhey Jan Hernandez100% (1)
- PLTC and CLTC Matrix and Training StaffDocument11 pagesPLTC and CLTC Matrix and Training StaffAASFI Private SchoolNo ratings yet
- NEAP Provision and Distribution of Communication Package For TeachersDocument9 pagesNEAP Provision and Distribution of Communication Package For TeachersJohn Lester Ysug Alenoid100% (1)
- District Gad Proposal Re - EchoDocument9 pagesDistrict Gad Proposal Re - EchoBeslig EsNo ratings yet
- May Project Proposal For Improvement of Makeshift Classroom and Comfort RoomDocument2 pagesMay Project Proposal For Improvement of Makeshift Classroom and Comfort RoomJoanne Sapla De LeonNo ratings yet
- CLC Classroom Structuring 1Document3 pagesCLC Classroom Structuring 1Al-jun Morilla Labastida100% (1)
- 1ST Certificate of Recognition Coach PosterDocument1 page1ST Certificate of Recognition Coach PosterDux MercadoNo ratings yet
- Home Visitation Form: Certificate of AppearanceDocument1 pageHome Visitation Form: Certificate of AppearanceAmorBabe Tabasa-PescaderoNo ratings yet
- Department of Education: Module 2 Most Essential Learning Competencies (Melcs)Document3 pagesDepartment of Education: Module 2 Most Essential Learning Competencies (Melcs)Natividad San Andres GriarteNo ratings yet
- Set Achievable and Appropriate Learning Outcomes That Aligned With Learning CompetenciesDocument4 pagesSet Achievable and Appropriate Learning Outcomes That Aligned With Learning Competenciesmhlq14100% (1)
- Camp Menu (Food)Document1 pageCamp Menu (Food)riza velascoNo ratings yet
- Department of Education: Schools Division of IsabelaDocument5 pagesDepartment of Education: Schools Division of IsabelaEdwin M. MartinezNo ratings yet
- General Form No 86 Health ExaminationDocument1 pageGeneral Form No 86 Health ExaminationArminda Annabelle Bangks86% (22)
- Letter SGC OrganizationDocument8 pagesLetter SGC OrganizationARGIE DEJECASIONNo ratings yet
- SIP Annex 1A - School-Community Data Template 10302015Document17 pagesSIP Annex 1A - School-Community Data Template 10302015Teody Villegas LimotNo ratings yet
- Activity, Training Design GADDocument3 pagesActivity, Training Design GADEdgar Atinen TagoonNo ratings yet
- Reflection Notes InsetDocument3 pagesReflection Notes InsetMarife A. Orillaneda100% (1)
- AcceptanceDocument3 pagesAcceptanceMaynard PascualNo ratings yet
- Joan Dalumpines Dy: Republic of The Philippines Department of EducationDocument2 pagesJoan Dalumpines Dy: Republic of The Philippines Department of EducationCha AndrianoNo ratings yet
- Mean Percentage Score TemplateDocument7 pagesMean Percentage Score TemplateMylene N. MacedaNo ratings yet
- History of The SchoolDocument4 pagesHistory of The SchoolŇel DanNo ratings yet
- Certification: To Whom It May ConcernDocument5 pagesCertification: To Whom It May ConcernShiarica Mae Atasan - NeriNo ratings yet
- RPMS-Cover PageDocument1 pageRPMS-Cover PageLawrenceAducaNo ratings yet
- Activity Design - EARLY ENROLLMENT SY 2022 2023Document5 pagesActivity Design - EARLY ENROLLMENT SY 2022 2023Carashola Panilagao100% (1)
- Reading Derby AccomplishmentDocument28 pagesReading Derby Accomplishmenthoney beeNo ratings yet
- Letter Request For Change Status 1Document1 pageLetter Request For Change Status 1Pamela Camille Plata BretonNo ratings yet
- Summary of IPCRF Rating SY 2022 2023Document1 pageSummary of IPCRF Rating SY 2022 2023ALBERT LEANILLONo ratings yet
- Certification: Republic of The Philippines Department of EducationDocument6 pagesCertification: Republic of The Philippines Department of EducationJeric MaribaoNo ratings yet
- Monitoring On The Status Report Slms Reproduction and DistributionDocument2 pagesMonitoring On The Status Report Slms Reproduction and DistributionAzyl Macaya GalagpatNo ratings yet
- Equivalent Record Form: Republic of The Philippines Department of Education Region Vi - Western Visayas Division of CapizDocument1 pageEquivalent Record Form: Republic of The Philippines Department of Education Region Vi - Western Visayas Division of CapizJL D. Busia100% (1)
- Department of Education: Second Quarter Cards Out Day Narrative ReportDocument3 pagesDepartment of Education: Second Quarter Cards Out Day Narrative ReportHanna Mae Corpuz100% (2)
- DepEd Camsur Unnumbered Memo October 5Document3 pagesDepEd Camsur Unnumbered Memo October 5Gab Rielle FloresNo ratings yet
- Cover Page For PromotionDocument1 pageCover Page For PromotionNathaniel Artajo Galopo100% (1)
- Training Design For CONTEXTUALIZATIONDocument5 pagesTraining Design For CONTEXTUALIZATIONcherry mae joy YbanezNo ratings yet
- Equivalent Record Form: Region Iv-A CalabarzonDocument1 pageEquivalent Record Form: Region Iv-A CalabarzonMj GarciaNo ratings yet
- 4ps Terminal ReportDocument5 pages4ps Terminal ReportNorie JoseNo ratings yet
- Department of Education: Application For LeaveDocument2 pagesDepartment of Education: Application For LeaveDarren Cariño100% (2)
- Consolidated Tbapa Grade 10 Group 6Document5 pagesConsolidated Tbapa Grade 10 Group 6Maria Rose Tariga AquinoNo ratings yet
- Certificate EsatDocument2 pagesCertificate EsatJAIRAH BAUSANo ratings yet
- Embarking On A Journey of Self-AwarenessDocument9 pagesEmbarking On A Journey of Self-Awarenesssalinaya recaro100% (2)
- Arh Activity DesignDocument10 pagesArh Activity Designjefferson faraNo ratings yet
- Certificate of Recognition: Gladys D. CabuscabusDocument2 pagesCertificate of Recognition: Gladys D. CabuscabusJaymar MagtibayNo ratings yet
- Letterhead New Logo Letter Parents Repainting Brigada Eskwela 2018-2019Document1 pageLetterhead New Logo Letter Parents Repainting Brigada Eskwela 2018-2019LORNA RENACIANo ratings yet
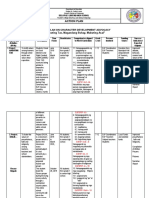
- Action Plan: Action Plan On Character Development Advocacy " Mabuting Tao, Magandang Buhay, Mabuting Asal"Document7 pagesAction Plan: Action Plan On Character Development Advocacy " Mabuting Tao, Magandang Buhay, Mabuting Asal"Lilet PaloNo ratings yet
- Parental Consent: Department of EducationDocument1 pageParental Consent: Department of EducationJhaii Sumi-og BerongesNo ratings yet
- 201 File Cover in LandscapeDocument1 page201 File Cover in LandscapeDhanessa CondesNo ratings yet
- Certificate of GADDocument2 pagesCertificate of GADgemma dalmacioNo ratings yet
- SMEPADocument29 pagesSMEPAHazel Joy Membrado Obongen100% (1)
- Mea Template For Sy 2020-2021Document44 pagesMea Template For Sy 2020-2021Leah Mae PinoteNo ratings yet
- PTA EkDocument1 pagePTA Ekhoney maeNo ratings yet
- Tardiness Monitoring FormDocument3 pagesTardiness Monitoring FormAnonymous 7BpT9OWPNo ratings yet
- Form 211Document1 pageForm 211Kairuz Demson AquilamNo ratings yet
- CS Form No. 211 Revised 2018 Medical Certificate Edited Copy 2Document1 pageCS Form No. 211 Revised 2018 Medical Certificate Edited Copy 2Jesse LeeNo ratings yet
- BitSat-PDR (PDFDrive)Document98 pagesBitSat-PDR (PDFDrive)Shivam MittalNo ratings yet
- WritDocument4 pagesWritKathryn20% (1)
- 2tradeasia Customer Application Information Form - UPDATEDocument10 pages2tradeasia Customer Application Information Form - UPDATEAnna Liza M. GasparNo ratings yet
- Impact of Urbanisation and Encroachment in Wetlands, A Case Study of Ganga Riparian Wetlands, Patna Impacts of Urbanization and Encroachment in Urban Wetlands, A Case Study of Gang..Document8 pagesImpact of Urbanisation and Encroachment in Wetlands, A Case Study of Ganga Riparian Wetlands, Patna Impacts of Urbanization and Encroachment in Urban Wetlands, A Case Study of Gang..Abdul QuadirNo ratings yet
- 12bf3577-2461-De1migration and Development: Future Directions For Research and Policy1-Bd80-001cc477ec70Document390 pages12bf3577-2461-De1migration and Development: Future Directions For Research and Policy1-Bd80-001cc477ec70Yasir AbdalmonimNo ratings yet
- DuPont AnalysisDocument14 pagesDuPont AnalysisManika AggarwalNo ratings yet
- Stoicism Is A School of PhilosophyDocument3 pagesStoicism Is A School of PhilosophyNahdatul FikraNo ratings yet
- Battle Companies 2016 1 PDFDocument117 pagesBattle Companies 2016 1 PDFMarcus BallNo ratings yet
- SAP Community Network Forums - Physical Inventory WM ..Document2 pagesSAP Community Network Forums - Physical Inventory WM ..Kosaraju SandeepNo ratings yet
- What Are The Important Stipulations in Magna Carta For Teachers and The Code of Ethics For Professional Teachers?Document1 pageWhat Are The Important Stipulations in Magna Carta For Teachers and The Code of Ethics For Professional Teachers?Junnel CasanovaNo ratings yet
- 098 - Essay Bhs - Inggris - Ahmad Mughni Al MubarokDocument5 pages098 - Essay Bhs - Inggris - Ahmad Mughni Al MubarokAhmad Mughni Al MubarokNo ratings yet
- Joy Global Inc: FORM 10-QDocument44 pagesJoy Global Inc: FORM 10-QfiahstoneNo ratings yet
- Mrugala Fabrice - Celtic GodsDocument13 pagesMrugala Fabrice - Celtic GodsElithemessieNo ratings yet
- Pan Files Library REC Peak Energy 72 Series Rev. ADocument4 pagesPan Files Library REC Peak Energy 72 Series Rev. AankitNo ratings yet
- Rededication Ceremonies For LeadersDocument4 pagesRededication Ceremonies For LeadersFritchie GinoNo ratings yet
- YM Website - User Manual: BookingDocument19 pagesYM Website - User Manual: Bookingwinda hervianaNo ratings yet
- British American Tobacco Bangladesh Company LTD Vs Begum Shamsun NaharDocument5 pagesBritish American Tobacco Bangladesh Company LTD Vs Begum Shamsun NaharFahim Shahriar MozumderNo ratings yet
- Detailed Lesson Plan - Teaching English in Elem - Grades - Gabat Clara ADocument8 pagesDetailed Lesson Plan - Teaching English in Elem - Grades - Gabat Clara AClara GabatNo ratings yet
- SAP Financial Accounting Configuration Steps - SAP Training TutorialsDocument45 pagesSAP Financial Accounting Configuration Steps - SAP Training TutorialsNaveen KumarNo ratings yet
- Summary of The Madrid Agreement Concerning The International Registration of Marks (1891) and The Protocol Relating To That Agreement (1989)Document5 pagesSummary of The Madrid Agreement Concerning The International Registration of Marks (1891) and The Protocol Relating To That Agreement (1989)Gilbert John LacorteNo ratings yet
- Consti Law Cases Chapters 1 To 3Document6 pagesConsti Law Cases Chapters 1 To 3Gervilyn Macarubbo Dotollo-SorianoNo ratings yet
- Challenge 7.1Document5 pagesChallenge 7.1JamRickNo ratings yet
- Assignment 1 Cittizenship & DiversityDocument2 pagesAssignment 1 Cittizenship & Diversitynickoh28No ratings yet
- Development and Development ParadigmsDocument49 pagesDevelopment and Development ParadigmsroblagrNo ratings yet
- Consolidated Civil Law QQR 1 PDFDocument33 pagesConsolidated Civil Law QQR 1 PDFMarcelino CasilNo ratings yet
- Repaso Unit 3 Travelling and HolidaysDocument3 pagesRepaso Unit 3 Travelling and HolidaysluciaNo ratings yet
- Education-Watch-Report - 2002Document84 pagesEducation-Watch-Report - 2002api-19623971No ratings yet
- Project IndustrialDocument16 pagesProject IndustrialMonic BasconNo ratings yet
- Trademark Law in India With Special Reference To Passing Off and Infringement of TrademarksDocument30 pagesTrademark Law in India With Special Reference To Passing Off and Infringement of TrademarksKUNAL1221No ratings yet
- Practice Test 1 PDFDocument22 pagesPractice Test 1 PDFvasean329No ratings yet