You might also like
- Medical Speech Language Pathology Across The Care Continuum An Introduction 1st Edition Alex Johnson Barbara Jacobson Megan Schliep Bridget PerryDocument45 pagesMedical Speech Language Pathology Across The Care Continuum An Introduction 1st Edition Alex Johnson Barbara Jacobson Megan Schliep Bridget Perryelizabeth.rouse409100% (2)
- Treatment of Skin Disease Comprehensive Therapeutic Strategies 6Th Edition Mark G Lebwohl 2 All ChapterDocument67 pagesTreatment of Skin Disease Comprehensive Therapeutic Strategies 6Th Edition Mark G Lebwohl 2 All Chapterfelipe.canada376100% (4)
- Abnormal Psychology - Clinical Persps. On Psych. Disorders, 6th Ed. - R. Halgin, Et. Al., (McGraw-Hill, 2010 WW-10-15Document6 pagesAbnormal Psychology - Clinical Persps. On Psych. Disorders, 6th Ed. - R. Halgin, Et. Al., (McGraw-Hill, 2010 WW-10-15bella swanNo ratings yet
- Family Life Cycle PDFDocument2 pagesFamily Life Cycle PDFDon'tAsK TheStupidOnes100% (1)
- Eustress Distress WorksheeDocument2 pagesEustress Distress WorksheeJoe LevinneNo ratings yet
- Biopsychosocial ModelDocument3 pagesBiopsychosocial ModelMaheen HamidNo ratings yet
- Issues in Family ManagementDocument21 pagesIssues in Family ManagementujaiNo ratings yet
- Psycho Social Factors in CancerDocument1 pagePsycho Social Factors in CancerPallabi ChatterjeeNo ratings yet
- Family ADocument2 pagesFamily AIzy FrancoNo ratings yet
- Therapuetic Intervention Referral FormDocument3 pagesTherapuetic Intervention Referral Formswinky kalraNo ratings yet
- Community Medicine Tranx (Family Life Cycle)Document4 pagesCommunity Medicine Tranx (Family Life Cycle)Kaye NeeNo ratings yet
- HEADSSDocument1 pageHEADSSBandya SahooNo ratings yet
- Tss Infographic 7 2015Document1 pageTss Infographic 7 2015api-356243627No ratings yet
- Perdev Activity 1 3Document1 pagePerdev Activity 1 3Prences Jhewen AlbisNo ratings yet
- Updated Intake Packet 2020Document21 pagesUpdated Intake Packet 2020Allison GomoNo ratings yet
- Report TypingDocument3 pagesReport TypingAansa AkramNo ratings yet
- Fish Bone 1Document1 pageFish Bone 1حسناء محمدNo ratings yet
- Risk and Protective Factors For DisordersDocument1 pageRisk and Protective Factors For Disordersapi-461452779No ratings yet
- Republic of The Philippines Department of Education Region Iv-A Calabarzon Division of Rizal Ampid National High SchoolDocument5 pagesRepublic of The Philippines Department of Education Region Iv-A Calabarzon Division of Rizal Ampid National High SchoolJoan E ArcebidoNo ratings yet
- Life Events ScaleDocument3 pagesLife Events ScaleDawn FarmNo ratings yet
- Why Do We Change Mind MapDocument1 pageWhy Do We Change Mind Mapapi-543374660No ratings yet
- SSP Profile SheetDocument1 pageSSP Profile SheetDwayne Bob LerionNo ratings yet
- Root CausesDocument25 pagesRoot CausesextraordinyariNo ratings yet
- Attachment K Clinical Interview and AssessmentDocument13 pagesAttachment K Clinical Interview and AssessmentMitesh HarmalkarNo ratings yet
- Table 5-4 - Issues Covered During The Family InterviewDocument2 pagesTable 5-4 - Issues Covered During The Family InterviewDragutin PetrićNo ratings yet
- Children, Families and Poverty: Ross A. Thompson, PH.DDocument9 pagesChildren, Families and Poverty: Ross A. Thompson, PH.DSagarNo ratings yet
- Root Cause Analysis ENROLMENT RATE SAMPLEDocument1 pageRoot Cause Analysis ENROLMENT RATE SAMPLEJon Graniada100% (1)
- The Impact of Economic HardshipDocument37 pagesThe Impact of Economic HardshipGabrielLopezNo ratings yet
- Psychiatry EoY History SampleDocument11 pagesPsychiatry EoY History SampleNicholasNo ratings yet
- Root Cause Dropped Out 2022Document1 pageRoot Cause Dropped Out 2022Janice G. FelipeNo ratings yet
- Preschool - Registration Form - 2020-21Document4 pagesPreschool - Registration Form - 2020-21Wrightsville FirstNo ratings yet
- 106 Bullying SurveyDocument3 pages106 Bullying SurveyMangsuan mungcheshamNo ratings yet
- Motivation of Fraudster (Kelompok 5)Document11 pagesMotivation of Fraudster (Kelompok 5)Syarifah Alda AzlikaNo ratings yet
- Stress Scale ReflectionDocument2 pagesStress Scale ReflectionSHIELA SAMANTHA SANTOSNo ratings yet
- Individualized Education ProgramDocument14 pagesIndividualized Education ProgramKeven James PaclejanNo ratings yet
- DCPS Referral Form Student Mental HealthDocument1 pageDCPS Referral Form Student Mental HealthsherryNo ratings yet
- Lesson 4Document12 pagesLesson 4Bethany PalinoNo ratings yet
- Adventist University of The Philippines: Family Assessment GuideDocument11 pagesAdventist University of The Philippines: Family Assessment GuideMarvel JazzrealNo ratings yet
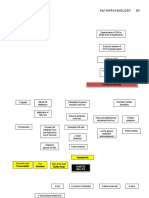
- PATHOPHYSIOLOGYDocument1 pagePATHOPHYSIOLOGYJhexy Rhay BayagenNo ratings yet
- Factors - Financial Problems: Poverty - Domestic Violence - History of Child Abuse - Form of Punishment or Disciplinary ActionDocument2 pagesFactors - Financial Problems: Poverty - Domestic Violence - History of Child Abuse - Form of Punishment or Disciplinary ActionIda HaidarNo ratings yet
- Toolkit For Carers: The Caring Role in Eating DisordersDocument10 pagesToolkit For Carers: The Caring Role in Eating DisordersGNo ratings yet
- Beed 2a - Group 4 - WorkplaceDocument17 pagesBeed 2a - Group 4 - WorkplaceParsley Thyme Painaga HipolitoNo ratings yet
- Problem and Objective Tree, RBMDocument12 pagesProblem and Objective Tree, RBMrolando.pabioNo ratings yet
- Pediatrics: Counselling of Parents With Hearing Impaired ChildrenDocument12 pagesPediatrics: Counselling of Parents With Hearing Impaired ChildrenHubs RamosNo ratings yet
- Preparing Chapter 8Document35 pagesPreparing Chapter 8Hawraa ShaalanNo ratings yet
- Revision Maps: Unit 1: Defining The Family (Pages 61-66)Document8 pagesRevision Maps: Unit 1: Defining The Family (Pages 61-66)Jul 480weshNo ratings yet
- Stressful Family or Friend SituationsDocument2 pagesStressful Family or Friend SituationsCinthia Hoyos jiménezNo ratings yet
- Unit 6 Daniela Barrientos Assignment 3Document11 pagesUnit 6 Daniela Barrientos Assignment 3api-585580789No ratings yet
- What Is PovertyDocument18 pagesWhat Is PovertySaurabh SumanNo ratings yet
- Case Formulation - Adult Clinical PsychologyDocument1 pageCase Formulation - Adult Clinical Psychologygfatima.pcpsychologistNo ratings yet
- Ashy#Document4 pagesAshy#ashley mapfumoNo ratings yet
- English Homework Week 31Document2 pagesEnglish Homework Week 31Ivan PilaresNo ratings yet
- Adolescent S and Well-Being: Stress, Depression, Weight Issues, and Body PositivityDocument2 pagesAdolescent S and Well-Being: Stress, Depression, Weight Issues, and Body PositivitygalelavNo ratings yet
- Case Analysis DelaoDocument6 pagesCase Analysis DelaoKenn Carlo DelaoNo ratings yet
- Lack of Parental Guidance: Engage inDocument5 pagesLack of Parental Guidance: Engage inMhygz Perez IINo ratings yet
- Client InformationDocument2 pagesClient Informationapi-395461859No ratings yet
- Building Your Resilience Workbooks (Fillable)Document15 pagesBuilding Your Resilience Workbooks (Fillable)Nicole JohnsonNo ratings yet
- Week 31Document1 pageWeek 31ana gabrielaNo ratings yet
- Mch. Rasul K. Gani 6Document4 pagesMch. Rasul K. Gani 6Mariam “Yham” BocaNo ratings yet
- Household: Reasons For Increase in One-Person Households: Segregated Conjugal RolesDocument2 pagesHousehold: Reasons For Increase in One-Person Households: Segregated Conjugal RolesIram GulfarazNo ratings yet
- Common Reactions To StressDocument1 pageCommon Reactions To StresssamuelNo ratings yet
- Coping Mechanism StressorsDocument2 pagesCoping Mechanism Stressorsjohn TabonNo ratings yet
- The Overwhelmed Parent: Tips for developing successful elementary school students, from a teacher's perspectiveFrom EverandThe Overwhelmed Parent: Tips for developing successful elementary school students, from a teacher's perspectiveNo ratings yet
- Generalizability Theory: An Introduction With Application To Simulation EvaluationDocument10 pagesGeneralizability Theory: An Introduction With Application To Simulation Evaluationbella swanNo ratings yet
- Kesiapsiagaan Anak Dalam Menghadapi Bencana: Studi Di Kabupaten SlemanDocument9 pagesKesiapsiagaan Anak Dalam Menghadapi Bencana: Studi Di Kabupaten Slemanbella swanNo ratings yet
- Generalizability Theory: January 2015Document21 pagesGeneralizability Theory: January 2015bella swanNo ratings yet
- Materi Group InfluenceDocument29 pagesMateri Group Influencebella swanNo ratings yet
- Peter Dickinson: Return To The CaseDocument5 pagesPeter Dickinson: Return To The Casebella swanNo ratings yet
- Abnormal Psychology 5th Ed by Gerald C Davidson-177-216Document40 pagesAbnormal Psychology 5th Ed by Gerald C Davidson-177-216bella swanNo ratings yet
- Online Learning Center: Student Resources About The BookDocument5 pagesOnline Learning Center: Student Resources About The Bookbella swanNo ratings yet
- Chapter 3 Job AnalysisDocument25 pagesChapter 3 Job Analysisbella swan100% (1)
- Rebec Ca Hasbrouck: Return To The CaseDocument5 pagesRebec Ca Hasbrouck: Return To The Casebella swanNo ratings yet
- Personal Adjustment and Mental Health-Pages-443-521-11-19Document9 pagesPersonal Adjustment and Mental Health-Pages-443-521-11-19bella swanNo ratings yet
- Psychological Causes: What Is Abnormal Behavior?Document5 pagesPsychological Causes: What Is Abnormal Behavior?bella swanNo ratings yet
- Chapter 13 Conflict and Peacemaking-36-39Document4 pagesChapter 13 Conflict and Peacemaking-36-39bella swanNo ratings yet
- RagozineDocument28 pagesRagozineMoisés MedinaNo ratings yet
- Veggie Restaurant Company Profile by SlidesgoDocument45 pagesVeggie Restaurant Company Profile by Slidesgobella swanNo ratings yet
- en The Relationship of Conformity and MemorDocument9 pagesen The Relationship of Conformity and Memorbella swanNo ratings yet
- Trivia Night by SlidesgoDocument51 pagesTrivia Night by Slidesgobella swanNo ratings yet
- Gender Differences in Personality Traits Across CuDocument11 pagesGender Differences in Personality Traits Across Cubella swanNo ratings yet
- Exercises in Plant Disease Epidemiology PDFDocument2 pagesExercises in Plant Disease Epidemiology PDFSherri50% (2)
- Types of Hazards and Food SafetyDocument5 pagesTypes of Hazards and Food SafetyAarajita ParinNo ratings yet
- 1166 Stomach Dr.-RaviDocument38 pages1166 Stomach Dr.-RaviKubra ĖdrisNo ratings yet
- AneurysmDocument7 pagesAneurysmLillabinNo ratings yet
- Candidiasis: Armie Jade S. Gante, RNDocument18 pagesCandidiasis: Armie Jade S. Gante, RNAnnapurna DangetiNo ratings yet
- Acute Prescribing - Challenges and Solutions - Ajit KulkarniDocument51 pagesAcute Prescribing - Challenges and Solutions - Ajit KulkarniAgha QaimiNo ratings yet
- Case Study On Biopsychosocial ApproachDocument19 pagesCase Study On Biopsychosocial ApproachCindy Mae MacamayNo ratings yet
- Listening 7Document2 pagesListening 7Bá Phúc PhạmNo ratings yet
- Medicine: Sudden Deaths From Positional AsphyxiaDocument5 pagesMedicine: Sudden Deaths From Positional AsphyxiaVanessa Veronica Irenea PatiNo ratings yet
- Healing Exercises For Internal Organs Help Your Body Quickly Recover From Cardiovascular, Gastrointestinal, Pulmonary, Urinary and Other Diseases by Greenberg, SamuelDocument123 pagesHealing Exercises For Internal Organs Help Your Body Quickly Recover From Cardiovascular, Gastrointestinal, Pulmonary, Urinary and Other Diseases by Greenberg, SamuelcvcrebeloNo ratings yet
- Pathophysiology Cushing S SyndromeDocument4 pagesPathophysiology Cushing S SyndromeMaria Luisa VillalunaNo ratings yet
- NCM 109 MCN Semifinals Gestational ConditionsDocument6 pagesNCM 109 MCN Semifinals Gestational ConditionsQUEZON, BRITNEY KIM E.No ratings yet
- Pharma 4 QDocument1 pagePharma 4 QMARIA PAULINA AMANTENo ratings yet
- Revision Notes Class 8 Science Chapter 2 - Micro-Organisms: Friend and FoeDocument7 pagesRevision Notes Class 8 Science Chapter 2 - Micro-Organisms: Friend and FoeArpit SharmaNo ratings yet
- Mov22. Hyperkinetic Disorders 3 (Tics, Myoclonus, Other)Document6 pagesMov22. Hyperkinetic Disorders 3 (Tics, Myoclonus, Other)Monica J Ortiz PereiraNo ratings yet
- Test Bank For Abnormal Psychology 7th Edition Thomas F OltmannsDocument38 pagesTest Bank For Abnormal Psychology 7th Edition Thomas F Oltmannscourtneyparkermdknscmrepzq100% (37)
- Soal Uts BHS Inggris KeperawatanDocument3 pagesSoal Uts BHS Inggris KeperawatanFriska SimbolonNo ratings yet
- Toxicology Tables PDFDocument23 pagesToxicology Tables PDFIssam HadiNo ratings yet
- SHC Asplenia Vaccine Guide 11-8-18 RevisionDocument4 pagesSHC Asplenia Vaccine Guide 11-8-18 RevisionEl LenNo ratings yet
- SchizophreniaDocument26 pagesSchizophreniapranesh premkumarNo ratings yet
- Genereal Examination-Anukul SurgeryDocument4 pagesGenereal Examination-Anukul SurgeryTRASH MAILNo ratings yet
- Meconium AspirationDocument7 pagesMeconium AspirationDelphy VargheseNo ratings yet
- Physiology of Pain: DR M Madhavi LathaDocument23 pagesPhysiology of Pain: DR M Madhavi Lathanico diangeloNo ratings yet
- Toxins: Use of Botulinum Toxin in Orofacial Clinical PracticeDocument16 pagesToxins: Use of Botulinum Toxin in Orofacial Clinical PracticeAfiliado LendárioNo ratings yet
- Prescurtari WhonetDocument6 pagesPrescurtari WhonetSimona TalpesNo ratings yet
- Leavell and ClarkDocument3 pagesLeavell and Clarkfildzahdiniatikahs100% (2)
- Case Presentation On AnemiaDocument27 pagesCase Presentation On AnemiaBhumi ChouhanNo ratings yet
- MS TopUp HandoutDocument4 pagesMS TopUp HandoutSTEFFI GABRIELLE GOLEZNo ratings yet