You might also like
- C. Explain The Principles of Drug AdministrationsDocument6 pagesC. Explain The Principles of Drug AdministrationsAubrey Nicole MacapagalNo ratings yet
- Suppositories: Presented byDocument21 pagesSuppositories: Presented byVanessa PatraoNo ratings yet
- Tutorial One: Routes of Drugs Administration&Dosage FormsDocument53 pagesTutorial One: Routes of Drugs Administration&Dosage FormsNarcissusNo ratings yet
- NCM103 SL - MedsDocument200 pagesNCM103 SL - MedsZen Gesner Kenneth G. EganaNo ratings yet
- MEDICATION ADMINISTRATION Reviewer AbreganaMarnitoDocument7 pagesMEDICATION ADMINISTRATION Reviewer AbreganaMarnitoBlaise Anne InocNo ratings yet
- Administering Medications and IV FluidsDocument41 pagesAdministering Medications and IV FluidsJada RichardsNo ratings yet
- Lecture On Drug AdministrationDocument140 pagesLecture On Drug AdministrationAngelinaNo ratings yet
- Medication AdministrationDocument27 pagesMedication AdministrationCrystal MaidenNo ratings yet
- Know Your Medicine UPH654: Nur Sabiha MD HussinDocument176 pagesKnow Your Medicine UPH654: Nur Sabiha MD HussinSyafiyatulMunawarahNo ratings yet
- Scope of Discussion: Prefinal Oral MedicationDocument4 pagesScope of Discussion: Prefinal Oral MedicationQueenie Kaye FrontalNo ratings yet
- Pharmacology 1Document7 pagesPharmacology 1Cleo PizarrasNo ratings yet
- Pharma - Midterm-Part 1Document17 pagesPharma - Midterm-Part 1Kaela ChoiNo ratings yet
- 4.1 - Doge and Doges FormsDocument28 pages4.1 - Doge and Doges FormsNo IdeaNo ratings yet
- Compare Liquid Dosage Form and Solid Dosage Form Base On Their Advantages and DisadvantagesDocument4 pagesCompare Liquid Dosage Form and Solid Dosage Form Base On Their Advantages and Disadvantagessybyl formenteraNo ratings yet
- 2 Forms &routes of Drug AdminDocument38 pages2 Forms &routes of Drug AdminNathaniel PulidoNo ratings yet
- Introduction Dosage Forms and Routes of Drug AdministrationDocument64 pagesIntroduction Dosage Forms and Routes of Drug AdministrationNaolNo ratings yet
- Introduction To Pharmaceutical Dosage FormDocument42 pagesIntroduction To Pharmaceutical Dosage FormSubha ShankareeNo ratings yet
- Funda PharmaDocument9 pagesFunda PharmaShiangNo ratings yet
- Dosage FormDocument7 pagesDosage FormKawtar MenjraNo ratings yet
- Sublingual Tablet Tapentadol HCL 2Document80 pagesSublingual Tablet Tapentadol HCL 2Maharshi PandyaNo ratings yet
- Pharmaceutical Dosage FormsDocument77 pagesPharmaceutical Dosage Formsester juanitaNo ratings yet
- Medications: By: Mrs. Mae G. Mallorca, R.N., M.A.N Ms. Jo Maree Pearl J. Oyco, R.NDocument66 pagesMedications: By: Mrs. Mae G. Mallorca, R.N., M.A.N Ms. Jo Maree Pearl J. Oyco, R.NGia Espinosa OcbeñaNo ratings yet
- Types of Drug Preparation (Credit To The Rightful Owner)Document1 pageTypes of Drug Preparation (Credit To The Rightful Owner)Keren Grace EspirituNo ratings yet
- Drug Administration: Wella Grace A. Go, RN, RMDocument78 pagesDrug Administration: Wella Grace A. Go, RN, RMPaulineNo ratings yet
- Finals Reviewer Funda SkillsDocument9 pagesFinals Reviewer Funda SkillsTricia Maxine DomingoNo ratings yet
- Hard Copy Sublingual FinalDocument7 pagesHard Copy Sublingual FinalRaya Ibarra LumogdangNo ratings yet
- FINALS MEDS - Part1Document58 pagesFINALS MEDS - Part1Ma. Isabel A. EnriquezNo ratings yet
- Dosage FormsDocument21 pagesDosage Formsyashaswim4No ratings yet
- Dosage FormsDocument27 pagesDosage FormsAhmed YTNo ratings yet
- Dosage Forms & RoutesDocument119 pagesDosage Forms & RoutesLowellaJulioNo ratings yet
- Basic Pharmacology NotesDocument83 pagesBasic Pharmacology NotesSanujNo ratings yet
- Pharmacokinetics and PharmacodynamicsDocument8 pagesPharmacokinetics and PharmacodynamicsAnonymous vKjGGgNo ratings yet
- What Is PharmacologyDocument59 pagesWhat Is PharmacologyNuha AgabnaNo ratings yet
- G4 Lecture NotesDocument13 pagesG4 Lecture NotesSehun OohNo ratings yet
- Nursing Pharmacology HandoutsDocument10 pagesNursing Pharmacology HandoutsMICHAELA TIMBOLNo ratings yet
- GLOSSARY of Terms With Specific Meanings For Pharmacists v9 2020Document5 pagesGLOSSARY of Terms With Specific Meanings For Pharmacists v9 2020beto betoyaNo ratings yet
- 7 MedicationsDocument83 pages7 MedicationsTuTitNo ratings yet
- Types of Dispensed PreparationsDocument67 pagesTypes of Dispensed Preparationsneha_dand15910% (1)
- Types of Dosage FormsDocument92 pagesTypes of Dosage Formsneha_dand1591No ratings yet
- UntitledDocument16 pagesUntitledIssac GeorgeNo ratings yet
- SuppositoriesDocument21 pagesSuppositoriesMyzhel InumerableNo ratings yet
- Buotan Si June Buotan Jud Si JuneDocument13 pagesBuotan Si June Buotan Jud Si JuneMajestic RavenNo ratings yet
- Drugs: Group: 1Document19 pagesDrugs: Group: 1Syifa AidilaNo ratings yet
- Dosage FormsDocument12 pagesDosage FormsBrix GallardoNo ratings yet
- Pharmacology 0615 PDFDocument89 pagesPharmacology 0615 PDFWRONGHEARNo ratings yet
- MEDICATIONDocument19 pagesMEDICATIONBeverly DatuNo ratings yet
- 2020 Easy Guide To Homeopathy - Single MedicinesDocument16 pages2020 Easy Guide To Homeopathy - Single MedicinesRitik KumarNo ratings yet
- Session 3 MEDICATION ADMINISTRATION (Summarized)Document10 pagesSession 3 MEDICATION ADMINISTRATION (Summarized)AlexandreaNo ratings yet
- Disperse SystemsDocument16 pagesDisperse SystemsMiguel MonsaludNo ratings yet
- NotesDocument7 pagesNotesBlessed Glaiza MarianoNo ratings yet
- Lecture 2Document40 pagesLecture 2Untouchable Monster 2No ratings yet
- Pharmacology Kechn Notes 2 1Document85 pagesPharmacology Kechn Notes 2 1mbaidavidmutuku1No ratings yet
- Understanding Drugs and Medicines 1Document31 pagesUnderstanding Drugs and Medicines 1radly.lopez09No ratings yet
- GENERAL PHARMACOLOGY (Absorption) - 1Document48 pagesGENERAL PHARMACOLOGY (Absorption) - 1samrawitmekonnen16No ratings yet
- Jurnal ResmiDocument6 pagesJurnal Resminurul100% (1)
- The Nature of Drug and Drug AbusedDocument18 pagesThe Nature of Drug and Drug AbusedINTERO, GERALD JANE S.No ratings yet
- Dosage Forms PC IDocument29 pagesDosage Forms PC Ianeri desaiNo ratings yet
- Community Pharmacy Intern Exercises5-9Document6 pagesCommunity Pharmacy Intern Exercises5-9Joslin RozNo ratings yet
- What Is MedicationDocument1 pageWhat Is Medication1BSN04 DE GUZMAN, LEMARRY JOYCE V.No ratings yet
- 27 Ovarian Cystectomy Consent FormDocument3 pages27 Ovarian Cystectomy Consent FormsekyNo ratings yet
- Hearing ImpairmentDocument20 pagesHearing ImpairmentAlexandra Villaflor HernandezNo ratings yet
- Writing Task Set 1Document62 pagesWriting Task Set 1RoneyNo ratings yet
- Final Ovarian Cancer Meigs Pathophysio PDFDocument3 pagesFinal Ovarian Cancer Meigs Pathophysio PDFCathy Santos100% (1)
- Paeds Case Write Up 1Document29 pagesPaeds Case Write Up 1Charlotte Ee33% (3)
- Singh Et Al-2013-Cochrane Database of Systematic ReviewsDocument73 pagesSingh Et Al-2013-Cochrane Database of Systematic Reviewspermenkes no 75 tahun 2014No ratings yet
- Disclosure: Interpreting Hematology Scatter-PlotsDocument29 pagesDisclosure: Interpreting Hematology Scatter-PlotsLaboratorium Ansari SalehNo ratings yet
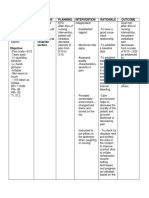
- NCP and Drug Study For Ob WardDocument7 pagesNCP and Drug Study For Ob WardAce Fabrigas100% (1)
- Health. Basic in First AidDocument16 pagesHealth. Basic in First AidAndrew ZafraNo ratings yet
- Herpetic StomatitisDocument21 pagesHerpetic StomatitisZulfahmi RizkiNo ratings yet
- Pathophysiology Cardiac ArrestDocument1 pagePathophysiology Cardiac ArrestPATHOSHOPPE100% (2)
- Reproductive Health Notes For NEET Download PDF - pdf-24Document4 pagesReproductive Health Notes For NEET Download PDF - pdf-24Sonty100% (1)
- FSRH Guideline Emergency Contraception 17mar2017 2Document65 pagesFSRH Guideline Emergency Contraception 17mar2017 2blopper123100% (1)
- Outside The Box - Rethinking ADD - ADHD in Children and Adults - A Practical Guide IDocument338 pagesOutside The Box - Rethinking ADD - ADHD in Children and Adults - A Practical Guide ICarlos Hernan Castañeda Ruiz100% (4)
- Persepsi Konsumen Dalam Menentukan Keputusan Pembelian Produk Minuman Dengan Klaim Kurang GulaDocument8 pagesPersepsi Konsumen Dalam Menentukan Keputusan Pembelian Produk Minuman Dengan Klaim Kurang GulaMuhammadSandyNo ratings yet
- Analysis of Veterinary Service Delivery in Uganda An Application of The Process Net-Map ToolDocument25 pagesAnalysis of Veterinary Service Delivery in Uganda An Application of The Process Net-Map ToolKYALIGONZA GEOFREYNo ratings yet
- GSK DOJ AgreementsDocument722 pagesGSK DOJ Agreements4207west59thNo ratings yet
- Superspeciality Admissions CourseDocument1 pageSuperspeciality Admissions Coursekiran kumarNo ratings yet
- Better Outcomes Lower Costs FSG&GIH Spring 2012Document18 pagesBetter Outcomes Lower Costs FSG&GIH Spring 2012iggybauNo ratings yet
- Overdenture VVDocument37 pagesOverdenture VVVikas Aggarwal50% (2)
- Lorna Pint AsDocument5 pagesLorna Pint Ascharlyn amadoNo ratings yet
- Bleeding in Early PregnancyDocument25 pagesBleeding in Early PregnancyAnnapurna DangetiNo ratings yet
- Intravenous Dexamethasone As An Analgesic: A Literature ReviewDocument6 pagesIntravenous Dexamethasone As An Analgesic: A Literature ReviewTri Utami JasmanNo ratings yet
- Tuberculosis LaryngitisDocument15 pagesTuberculosis Laryngitisrizgah jawasNo ratings yet
- Colorado COVID-19 Public Health Order April 15, 2021Document7 pagesColorado COVID-19 Public Health Order April 15, 2021Michael_Roberts2019No ratings yet
- Trend 10 DiseaseDocument8 pagesTrend 10 Diseasehanung satrioNo ratings yet
- Opioides y ArtroplastiaDocument10 pagesOpioides y ArtroplastiaCirugia HEAVNo ratings yet
- Practice: Failures in Implant DentistryDocument7 pagesPractice: Failures in Implant DentistryhmsatNo ratings yet
- ISK Pada Anak (Ade Sinta)Document10 pagesISK Pada Anak (Ade Sinta)Ades SundayNo ratings yet
- Health Information System SecondaryDocument6 pagesHealth Information System SecondaryAlondra Aran0% (1)