You might also like
- DKA DrawioDocument2 pagesDKA DrawioSOPHIA LOISE TEJANO FULACHENo ratings yet
- Concept Map MarwahDocument5 pagesConcept Map MarwahAsniah Hadjiadatu AbdullahNo ratings yet
- Schematic Pathophy DkaDocument2 pagesSchematic Pathophy DkaMaria Francheska OsiNo ratings yet
- AlgoDocument1 pageAlgoErrold Joseph LahaganNo ratings yet
- Legend: - Precipitating Factors - Flow - Medical Diagnosis - Nursing Diagnosis - Lab Results - MedicationsDocument1 pageLegend: - Precipitating Factors - Flow - Medical Diagnosis - Nursing Diagnosis - Lab Results - MedicationsEricka GenoveNo ratings yet
- Hormone NotesDocument8 pagesHormone Noteslaeticia schmiesNo ratings yet
- Drug StudyDocument18 pagesDrug StudyJinky Nacar DomingoNo ratings yet
- Pathophysiology of Diabetes Mellitus Type IIDocument14 pagesPathophysiology of Diabetes Mellitus Type IIElay PedrosoNo ratings yet
- Disease Patho Manifestations Assessment Labs Other Notes DKA Used To Suppress Ketogenesis, Gluconeogenesis NOT Just To Lower BGDocument1 pageDisease Patho Manifestations Assessment Labs Other Notes DKA Used To Suppress Ketogenesis, Gluconeogenesis NOT Just To Lower BGSara SabraNo ratings yet
- Concept Map AtekharlssDocument3 pagesConcept Map AtekharlssAsniah Hadjiadatu AbdullahNo ratings yet
- DKA Current Practices in Africa 02 - 02 - 2022-1Document30 pagesDKA Current Practices in Africa 02 - 02 - 2022-1Raphael SeretiNo ratings yet
- Patho 1Document1 pagePatho 1ricciNo ratings yet
- Diabetic Ketoacidosis Protocol PICU Oct 2010 2Document9 pagesDiabetic Ketoacidosis Protocol PICU Oct 2010 2Vidini Kusuma AjiNo ratings yet
- Endocrine DisordersDocument2 pagesEndocrine DisordersRalph Elvin MacanlalayNo ratings yet
- HomeostasisDocument34 pagesHomeostasisAwaid AsimNo ratings yet
- Anatomy of The Pancreas: Regulate Blood Glucose - The Fuel ThatDocument2 pagesAnatomy of The Pancreas: Regulate Blood Glucose - The Fuel ThatSkyerex100% (1)
- Pathophysiology CKD - DrawioDocument54 pagesPathophysiology CKD - DrawioGwyneth CiriloNo ratings yet
- Drug StudyDocument8 pagesDrug StudyjovanneyNo ratings yet
- Patient Based Patho GDMDocument1 pagePatient Based Patho GDMMarc SorianoNo ratings yet
- Metabolisme Karbohidrat Dan Integrasinya DG Regulasi HormonalDocument21 pagesMetabolisme Karbohidrat Dan Integrasinya DG Regulasi HormonalMahendra Yudha NNo ratings yet
- Insulin Mechanism of Action and Nursing ResponsibilitiesDocument7 pagesInsulin Mechanism of Action and Nursing ResponsibilitiesGrape JuiceNo ratings yet
- Diabetic Ketoacidosis Written ReportDocument19 pagesDiabetic Ketoacidosis Written ReportEros Victorino100% (2)
- Biochemical Changes of Diabetes MellitusDocument4 pagesBiochemical Changes of Diabetes MellitusGerardLum100% (3)
- Assessment Using Functional Health Patterns: AppendixDocument16 pagesAssessment Using Functional Health Patterns: AppendixNalzaro Emyril89% (19)
- Gonzales, Elyhna Bsn2d Drugstudy Unit8Document3 pagesGonzales, Elyhna Bsn2d Drugstudy Unit8Elyhna GonzalesNo ratings yet
- DM Type 2 Pa Tho PhysiologyDocument4 pagesDM Type 2 Pa Tho PhysiologyEllen Grace Cañarejo BaroyNo ratings yet
- Insulin Drug Nursing ResponsibilitiesDocument2 pagesInsulin Drug Nursing ResponsibilitiesSophia MarieNo ratings yet
- Drug Study Insulin LisproDocument2 pagesDrug Study Insulin LisproEzron Kendrick Duran100% (1)
- PathophysiologyDocument1 pagePathophysiologyVanessa SumalbagNo ratings yet
- Diabetic KetoacidosisDocument37 pagesDiabetic KetoacidosisjjNo ratings yet
- Glucagon and Its Metabolic EffectsDocument31 pagesGlucagon and Its Metabolic EffectsnikenNo ratings yet
- Endocrine DisordersDocument5 pagesEndocrine DisordersMae Arra Gilbao Lecobu-anNo ratings yet
- CalciumDocument1 pageCalciumGILIANNE MARIE JIMENEANo ratings yet
- Schematic DiagramDocument4 pagesSchematic DiagramEmber Marie SaymanNo ratings yet
- Liver Cirrhosis Melena Episodes of Fainting Disturbance in Sleep-Wake Pattern Epigastric Pain Passage of Black StoolsDocument7 pagesLiver Cirrhosis Melena Episodes of Fainting Disturbance in Sleep-Wake Pattern Epigastric Pain Passage of Black StoolsLyndon SayongNo ratings yet
- Diabetes Lecture Note-6thDocument46 pagesDiabetes Lecture Note-6tholawandeilo123No ratings yet
- Drug Study TemplateDocument2 pagesDrug Study TemplateMary hope DomalaonNo ratings yet
- Regulare GastricăDocument3 pagesRegulare GastricăAurelia AlexandraNo ratings yet
- Drug Study: West Visayas State UniversityDocument2 pagesDrug Study: West Visayas State UniversityDivine Mercy De JulianNo ratings yet
- 1.2 Patient PreparationDocument4 pages1.2 Patient PreparationKenneth Brayan B. CastilloNo ratings yet
- HEG PathoPhyDocument1 pageHEG PathoPhyQuintin MangaoangNo ratings yet
- Predisposing Factor Disease Process Signs and Symptoms Medications Medical Interventions Medical DiagnosisDocument4 pagesPredisposing Factor Disease Process Signs and Symptoms Medications Medical Interventions Medical DiagnosisSkyla FiestaNo ratings yet
- Drug Card UpdateDocument12 pagesDrug Card UpdatekeenyadeniseNo ratings yet
- Name of Student Nurse: Medication Study GuideDocument1 pageName of Student Nurse: Medication Study GuideGracia Dela CruzNo ratings yet
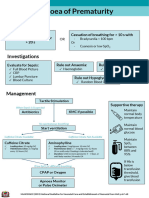
- 17 Apnoea PrematurityDocument1 page17 Apnoea PrematurityYassboy MsdNo ratings yet
- Drug Study - Med WardDocument13 pagesDrug Study - Med WardFretzgine Lou ManuelNo ratings yet
- Drug Study: CNS: FeverDocument13 pagesDrug Study: CNS: FeverRoland YusteNo ratings yet
- PATHOPHYSIOLOGYDocument2 pagesPATHOPHYSIOLOGYGerome ManantanNo ratings yet
- Metformin classification, indications, actions, contraindications and nursing responsibilitiesDocument7 pagesMetformin classification, indications, actions, contraindications and nursing responsibilitiesgateway1119No ratings yet
- Hormone regulation and the hypothalamus-pituitary axisDocument16 pagesHormone regulation and the hypothalamus-pituitary axisCal GoNo ratings yet
- IM - DKA PathophysDocument2 pagesIM - DKA PathophysTrisNo ratings yet
- Topic 2.1: Organisation & HomeostasisDocument21 pagesTopic 2.1: Organisation & HomeostasisJun Hong TeeNo ratings yet
- Nursing Care Plan for Patient with DiarrheaDocument2 pagesNursing Care Plan for Patient with DiarrheaThan Ramile Dela CruzNo ratings yet
- MCN Form 014Document4 pagesMCN Form 014jericho dinglasanNo ratings yet
- Systemic and Local ChangesDocument4 pagesSystemic and Local ChangesAristia ObeliaNo ratings yet
- Drug Study On Agents Used Thyroid and Glucose Metabolism - ClementeDocument18 pagesDrug Study On Agents Used Thyroid and Glucose Metabolism - ClementeJames Emman ClementeNo ratings yet
- 6 Stages Of Fasting - Based On The Teachings Of Dr. Eric Berg: The Evolution Of FastingFrom Everand6 Stages Of Fasting - Based On The Teachings Of Dr. Eric Berg: The Evolution Of FastingNo ratings yet
- Ketogenic Diet for Beginners - How to Get Started on the Keto Diet: Unlock the Superfuel of Your Body, Burn the Stubborn Fats while you Sleep & Lose Weight PermanentlyFrom EverandKetogenic Diet for Beginners - How to Get Started on the Keto Diet: Unlock the Superfuel of Your Body, Burn the Stubborn Fats while you Sleep & Lose Weight PermanentlyRating: 5 out of 5 stars5/5 (2)
- 2020 The Essential Diets - All Diets in One Book - Ketogenic, Mediterranean, Mayo, Zone Diet, High Protein, Vegetarian, Vegan, Detox, Paleo, Alkaline Diet and Much More: COOKBOOK, #2From Everand2020 The Essential Diets - All Diets in One Book - Ketogenic, Mediterranean, Mayo, Zone Diet, High Protein, Vegetarian, Vegan, Detox, Paleo, Alkaline Diet and Much More: COOKBOOK, #2No ratings yet
- Ketosis Strips User’s Guide: Quick & Easy Guide to Using Keto Test Strips to Correctly Measure ketone Levels in Urine, Blood and Getting into Ketosis fasterFrom EverandKetosis Strips User’s Guide: Quick & Easy Guide to Using Keto Test Strips to Correctly Measure ketone Levels in Urine, Blood and Getting into Ketosis fasterRating: 5 out of 5 stars5/5 (1)
- Amputation and Appendectomy Nursing CareDocument2 pagesAmputation and Appendectomy Nursing CareSOPHIA LOISE TEJANO FULACHENo ratings yet
- Predisposing Factors Disease Precipitating Factors: LegendDocument3 pagesPredisposing Factors Disease Precipitating Factors: LegendSOPHIA LOISE TEJANO FULACHENo ratings yet
- CHF: Congestive Heart Failure Diagnosis, Pathophysiology, and ManagementDocument6 pagesCHF: Congestive Heart Failure Diagnosis, Pathophysiology, and ManagementSOPHIA LOISE TEJANO FULACHENo ratings yet
- Predisposing Factors Disease Precipitating Factors: LegendDocument3 pagesPredisposing Factors Disease Precipitating Factors: LegendSOPHIA LOISE TEJANO FULACHENo ratings yet
- Predisposing Factors Disease Precipitating Factors: LegendDocument3 pagesPredisposing Factors Disease Precipitating Factors: LegendSOPHIA LOISE TEJANO FULACHENo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Cause PathophysiologyDocument3 pagesChronic Obstructive Pulmonary Disease (COPD) : Cause PathophysiologySOPHIA LOISE TEJANO FULACHENo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Cause PathophysiologyDocument3 pagesChronic Obstructive Pulmonary Disease (COPD) : Cause PathophysiologySOPHIA LOISE TEJANO FULACHENo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) : Cause PathophysiologyDocument3 pagesChronic Obstructive Pulmonary Disease (COPD) : Cause PathophysiologySOPHIA LOISE TEJANO FULACHENo ratings yet
- CHF: Congestive Heart Failure Diagnosis, Pathophysiology, and ManagementDocument6 pagesCHF: Congestive Heart Failure Diagnosis, Pathophysiology, and ManagementSOPHIA LOISE TEJANO FULACHENo ratings yet
- Teltonika Networks CatalogueDocument40 pagesTeltonika Networks CatalogueazizNo ratings yet
- Economic and Eco-Friendly Analysis of Solar Power Refrigeration SystemDocument5 pagesEconomic and Eco-Friendly Analysis of Solar Power Refrigeration SystemSiddh BhattNo ratings yet
- 1958 - The Automatic Creation of Literature AbstractsDocument7 pages1958 - The Automatic Creation of Literature AbstractsFranck DernoncourtNo ratings yet
- (332-345) IE - ElectiveDocument14 pages(332-345) IE - Electivegangadharan tharumarNo ratings yet
- Coaching Can Be Defined As The Process of MotivatingDocument5 pagesCoaching Can Be Defined As The Process of MotivatingDaniel DowdingNo ratings yet
- L-Ascorbic AcidDocument3 pagesL-Ascorbic AcidJemNo ratings yet
- Chapter OneDocument18 pagesChapter Oneحيدر محمدNo ratings yet
- Astm d5580Document9 pagesAstm d5580Nhu SuongNo ratings yet
- The Best Chicken Quesadillas - Mel's Kitchen Cafe 4Document1 pageThe Best Chicken Quesadillas - Mel's Kitchen Cafe 4Yun LiuNo ratings yet
- What is Strategic Human Resource ManagementDocument8 pagesWhat is Strategic Human Resource ManagementYashasvi ParsaiNo ratings yet
- Diease LossDocument10 pagesDiease LossGeetha EconomistNo ratings yet
- Common Phrasal VerbsDocument2 pagesCommon Phrasal VerbsOscar LasprillaNo ratings yet
- Readings in Philippine History: Tanza, Boac, MarinduqueDocument16 pagesReadings in Philippine History: Tanza, Boac, MarinduqueLucy SyNo ratings yet
- Chord MethodDocument17 pagesChord MethodJedielson GirardiNo ratings yet
- Business Math - Interest QuizDocument1 pageBusiness Math - Interest QuizAi ReenNo ratings yet
- 2nd Quarter Week 7Document5 pages2nd Quarter Week 7Lymieng LimoicoNo ratings yet
- Investigating and EvaluatingDocument12 pagesInvestigating and EvaluatingMuhammad AsifNo ratings yet
- NTSE MAT Maharashtra 2011Document38 pagesNTSE MAT Maharashtra 2011Edward FieldNo ratings yet
- Organizational Learning, Innovation, and ChangeDocument37 pagesOrganizational Learning, Innovation, and Changejaypee pengNo ratings yet
- 5 Harms of Excessive Use of Electronic GamesDocument3 pages5 Harms of Excessive Use of Electronic GamesPierre MarucciNo ratings yet
- Python Module 7 AFV Core-Data-StructureDocument48 pagesPython Module 7 AFV Core-Data-StructureLeonardo FernandesNo ratings yet
- Minerals for Civil EngineersDocument6 pagesMinerals for Civil EngineersConrado Seguritan IIINo ratings yet
- Week 14 - LECTURE ACTIVITY 14 - Metamorphic RX Key ConceptsDocument4 pagesWeek 14 - LECTURE ACTIVITY 14 - Metamorphic RX Key ConceptsJessel Razalo BunyeNo ratings yet
- Ch. 8 - Managing Project Quality Flashcards by Brian Weldon - BrainscapeDocument8 pagesCh. 8 - Managing Project Quality Flashcards by Brian Weldon - BrainscapeKay MendozaNo ratings yet
- Lovacka Kamera UputstvoDocument24 pagesLovacka Kamera UputstvoEmir MusijaNo ratings yet
- Group5 AssignmentDocument10 pagesGroup5 AssignmentYenew AyenewNo ratings yet
- Evaluating Usability of Superstore Self-Checkout KioskDocument48 pagesEvaluating Usability of Superstore Self-Checkout Kioskcipiripi14No ratings yet
- Strategic Cost ManagementDocument3 pagesStrategic Cost ManagementShubakar ReddyNo ratings yet
- Syntax Score Calculation With Multislice Computed Tomographic Angiography in Comparison To Invasive Coronary Angiography PDFDocument5 pagesSyntax Score Calculation With Multislice Computed Tomographic Angiography in Comparison To Invasive Coronary Angiography PDFMbak RockerNo ratings yet
- Botulinum Toxin in Aesthetic Medicine Myths and RealitiesDocument12 pagesBotulinum Toxin in Aesthetic Medicine Myths and RealitiesЩербакова ЛенаNo ratings yet