You might also like
- Community Health Profile Worksheet (Worksheet C)Document10 pagesCommunity Health Profile Worksheet (Worksheet C)Jahay NielNo ratings yet
- Family Assessment Guide Family No. 4Document8 pagesFamily Assessment Guide Family No. 4Andrix Wynken SapanNo ratings yet
- Family Assessment Guide Family No. 5Document8 pagesFamily Assessment Guide Family No. 5Andrix Wynken SapanNo ratings yet
- Student InventoryDocument2 pagesStudent Inventoryleo dumapiNo ratings yet
- Family Assessment GuideDocument4 pagesFamily Assessment Guidejpoti0% (1)
- Needs Assessment SurveyDocument2 pagesNeeds Assessment SurveyPatrick SanchezNo ratings yet
- Family Assessment GuideDocument5 pagesFamily Assessment GuideAngelica Jane GomezNo ratings yet
- Family Health Problem (Common) / Abnormality: (E.g. Uncle)Document2 pagesFamily Health Problem (Common) / Abnormality: (E.g. Uncle)Evelyn Medina100% (1)
- I. Demographic Data II. Family Data: College of Nursing Health Care 1BDocument4 pagesI. Demographic Data II. Family Data: College of Nursing Health Care 1BFatima Diane S. MondejarNo ratings yet
- Idb Assessment Form2Document6 pagesIdb Assessment Form2GemNo ratings yet
- Individual Inventory FormDocument2 pagesIndividual Inventory FormALLAN PALATTAO100% (1)
- Idb Assessment FormDocument6 pagesIdb Assessment FormCorillo, Fionnula JeanNo ratings yet
- St. Paul College of Ilocos SurDocument13 pagesSt. Paul College of Ilocos SurJemina Rafanan RacadioNo ratings yet
- Family Members: M Married College Graduate Tricycle Operator F Married College Graduate Housewife 19 M Single N/ADocument4 pagesFamily Members: M Married College Graduate Tricycle Operator F Married College Graduate Housewife 19 M Single N/Aaron frondaNo ratings yet
- Family Assessment GuideDocument5 pagesFamily Assessment GuideHappyOwl01No ratings yet
- GivenDocument4 pagesGivenKaren Lou SalimNo ratings yet
- Local Media8154377969260507143 1Document3 pagesLocal Media8154377969260507143 1Johanie Bolawan MamaNo ratings yet
- Gco Form 1personal Data RecordDocument5 pagesGco Form 1personal Data RecordROMELYN BALBIDONo ratings yet
- St. Paul College of Ilocos SurDocument5 pagesSt. Paul College of Ilocos SurRica machells DaydaNo ratings yet
- Family Assessment ToolDocument5 pagesFamily Assessment Toolkjmafioso17No ratings yet
- New Patient PaperworkDocument3 pagesNew Patient PaperworkThomas CampbellNo ratings yet
- Oct. 17 2020 CHN1 FAMILY HEALTH ASSESSMENT FORMDocument7 pagesOct. 17 2020 CHN1 FAMILY HEALTH ASSESSMENT FORMFoxtrot Nursing100% (1)
- Barangay Profile Survey Form: I. Family Members and CharacteristicsDocument5 pagesBarangay Profile Survey Form: I. Family Members and CharacteristicsCharlene Grace Regino100% (1)
- 2021 Family Assessment ToolDocument3 pages2021 Family Assessment Toolanchetajennifer39No ratings yet
- OSCA ID Application For Senior CitizenDocument2 pagesOSCA ID Application For Senior Citizenbarangay twentynineNo ratings yet
- NSTP CWTS Final Output QuestionnaireDocument2 pagesNSTP CWTS Final Output QuestionnaireANJHIELYN MAE CAHILIGNo ratings yet
- SCSIT Family-Assessment-GuideDocument5 pagesSCSIT Family-Assessment-GuideRS BuenavistaNo ratings yet
- NaturalhealthhistoryqDocument9 pagesNaturalhealthhistoryqapi-293713675No ratings yet
- Final Community FormDocument7 pagesFinal Community FormalyanadayritNo ratings yet
- Guidance Inventory FormDocument3 pagesGuidance Inventory FormChrishelle PalacpacNo ratings yet
- SOM Application FormDocument5 pagesSOM Application FormMark MejiaNo ratings yet
- Updated Counseling Referral FormDocument11 pagesUpdated Counseling Referral FormcelestinoptrixieNo ratings yet
- NSTP 12 Requirement - Community ProfileDocument5 pagesNSTP 12 Requirement - Community ProfileFrancisco NiegasNo ratings yet
- Department of Education: Region: - DivisionDocument2 pagesDepartment of Education: Region: - DivisionKristofer Aaron UngriaNo ratings yet
- Hyde Square Task Force Youth Leadership ApplicationDocument9 pagesHyde Square Task Force Youth Leadership ApplicationKaren BossNo ratings yet
- Community Survey Tool 2Document8 pagesCommunity Survey Tool 2Erika BacarroNo ratings yet
- 04survey Form Urban 2022 EngDocument6 pages04survey Form Urban 2022 EngisahNo ratings yet
- Gordons Functional Health Patterns Assessment 1Document11 pagesGordons Functional Health Patterns Assessment 1Katherine Lizell LopezNo ratings yet
- Instituto de Idiomas Teacher: Mg. Danny Percy Ureña VillazanteDocument3 pagesInstituto de Idiomas Teacher: Mg. Danny Percy Ureña VillazanteEC MariaNo ratings yet
- Personal Background Form Updated 8.22.17Document6 pagesPersonal Background Form Updated 8.22.17Marichelle AbreganaNo ratings yet
- Northwestern University, Inc: Laoag City, Ilocos NorteDocument3 pagesNorthwestern University, Inc: Laoag City, Ilocos NorteAlex MarcosNo ratings yet
- St. Paul College of Ilocos SurDocument15 pagesSt. Paul College of Ilocos SurJemina Rafanan RacadioNo ratings yet
- Nursing Care Health Assessment FormDocument5 pagesNursing Care Health Assessment FormMelanie Bagasol SisonNo ratings yet
- Community Health Diagnosis Survey Tool - docx.FINALDocument3 pagesCommunity Health Diagnosis Survey Tool - docx.FINALMonalisa TrayaNo ratings yet
- Annex B. Intake Sheet InterviewDocument4 pagesAnnex B. Intake Sheet InterviewcelestinoptrixieNo ratings yet
- Survey QuestionnaireDocument9 pagesSurvey QuestionnaireMannieNadateCatriz100% (6)
- Pender Humane Adoption Form3 PDFDocument6 pagesPender Humane Adoption Form3 PDFEneida Martinez CintronNo ratings yet
- GFHP QuestionsDocument16 pagesGFHP QuestionsaviaquaNo ratings yet
- Art of Growing Questionnaire For EntomologistsDocument3 pagesArt of Growing Questionnaire For EntomologistsDarniel YamsNo ratings yet
- Homeroom Guidance AnswersheetDocument7 pagesHomeroom Guidance AnswersheetMaria Anna Estorgio TrayaNo ratings yet
- Idb Assessment FormDocument7 pagesIdb Assessment FormNeri DelfinNo ratings yet
- Periodical Exam 9Document4 pagesPeriodical Exam 9Jassien Moring FlorentinoNo ratings yet
- Family Assessment GuideDocument9 pagesFamily Assessment GuideChristine Lindsey BenaroNo ratings yet
- Initial Data Base For Family Nursing PracticeDocument9 pagesInitial Data Base For Family Nursing PracticeMD PraxNo ratings yet
- 2019 01 30 19 24 04 Jose - Cardenas JOSE CARDENA 2018110340 UNIT2Document8 pages2019 01 30 19 24 04 Jose - Cardenas JOSE CARDENA 2018110340 UNIT2ANA MICHELLE FRANCO VELASQUEZ33% (3)
- DH Health Assessment FormDocument3 pagesDH Health Assessment FormRayceNo ratings yet
- Fichapreparaçao TespDocument8 pagesFichapreparaçao TespMargarida GuimaraesNo ratings yet
- Ateneo de Zamboanga Som - ApplicationDocument5 pagesAteneo de Zamboanga Som - ApplicationKai BenlotNo ratings yet
- Governmental Traumatizing Investigations: An Application to Get a New Toilet, Part IFrom EverandGovernmental Traumatizing Investigations: An Application to Get a New Toilet, Part INo ratings yet
- NCP Stab Wound (Artillo)Document7 pagesNCP Stab Wound (Artillo)Al TheóNo ratings yet
- ARTILLO Losartan Drug StudyDocument3 pagesARTILLO Losartan Drug StudyAl TheóNo ratings yet
- Mental Status Exam (MSE-ABC) - 1Document1 pageMental Status Exam (MSE-ABC) - 1Al TheóNo ratings yet
- HTP Lacerated Wound Case 1 Group1 BN3BDocument9 pagesHTP Lacerated Wound Case 1 Group1 BN3BAl TheóNo ratings yet
- Lacerated Wound Forms (Artillo)Document9 pagesLacerated Wound Forms (Artillo)Al TheóNo ratings yet
- Sakit Akon Tiyan Kada Mag Ubo-Ubo Ko.": Predisposing Factors: Precipitating FactorsDocument4 pagesSakit Akon Tiyan Kada Mag Ubo-Ubo Ko.": Predisposing Factors: Precipitating FactorsAl TheóNo ratings yet
- University of St. La Salle College of Nursing Nursing Care Plan Name of Student: - Artillo, Aljean Altheo L Name of CIDocument2 pagesUniversity of St. La Salle College of Nursing Nursing Care Plan Name of Student: - Artillo, Aljean Altheo L Name of CIAl TheóNo ratings yet
- Worksheet C & Upgraded Scenario (Artillo)Document15 pagesWorksheet C & Upgraded Scenario (Artillo)Al TheóNo ratings yet
- Schizophrenia (DS)Document7 pagesSchizophrenia (DS)Al TheóNo ratings yet
- Tita Senal RN, MN, PHD - Area of Exposure: - Bacolod City Mental Health Care CenterDocument4 pagesTita Senal RN, MN, PHD - Area of Exposure: - Bacolod City Mental Health Care CenterAl TheóNo ratings yet
- Aljean Altheo L. Artillo BSN-3B "Describe Your Community" Location/Address of Your Communit: Block 2 Lot 5, Alida Residences, Silay CityDocument9 pagesAljean Altheo L. Artillo BSN-3B "Describe Your Community" Location/Address of Your Communit: Block 2 Lot 5, Alida Residences, Silay CityAl TheóNo ratings yet
- Research Ethics Review Committee: Urc@usls - Edu.phDocument3 pagesResearch Ethics Review Committee: Urc@usls - Edu.phAl TheóNo ratings yet
- Aljean Altheo L. Artillo BSN-3B Anxiety LogDocument1 pageAljean Altheo L. Artillo BSN-3B Anxiety LogAl TheóNo ratings yet
- Who Surgical Safety Checklist: Be Polite. Thank EveryoneDocument1 pageWho Surgical Safety Checklist: Be Polite. Thank EveryoneAl TheóNo ratings yet
- Surgery Case Scenario 1Document5 pagesSurgery Case Scenario 1Al TheóNo ratings yet
- Case Scenario 2 MarioDocument1 pageCase Scenario 2 MarioAl TheóNo ratings yet
- Medication Sheet: Complete Name and Initials of Medication NurseDocument1 pageMedication Sheet: Complete Name and Initials of Medication NurseAl TheóNo ratings yet
- ARTILLO Drug StudyDocument5 pagesARTILLO Drug StudyAl TheóNo ratings yet
- Date: November 6, 2021 Date: Date:: Date Hospital Days Post-Op/Post-Partu Hour AM PM AM PM AM PM Pulse Rate 150Document1 pageDate: November 6, 2021 Date: Date:: Date Hospital Days Post-Op/Post-Partu Hour AM PM AM PM AM PM Pulse Rate 150Al TheóNo ratings yet
- Artillo-Fdar Nurses NotesDocument2 pagesArtillo-Fdar Nurses NotesAl TheóNo ratings yet
- Intravenous/Parenteral Fluid SheetDocument1 pageIntravenous/Parenteral Fluid SheetAl TheóNo ratings yet
- Artillo NCP Renal Cell CarcinomaDocument5 pagesArtillo NCP Renal Cell CarcinomaAl TheóNo ratings yet
- Artillo NCP Renal Cell CarcinomaDocument5 pagesArtillo NCP Renal Cell CarcinomaAl TheóNo ratings yet
- Drug Study SitagliptinDocument2 pagesDrug Study SitagliptinAl Theó0% (1)
- Health Teaching: Medication Exercise Treatment Hygiene Outpatient DietDocument3 pagesHealth Teaching: Medication Exercise Treatment Hygiene Outpatient DietAl TheóNo ratings yet
- My COPD Action Plan: Green Zone: I Am Doing Well Today ActionsDocument2 pagesMy COPD Action Plan: Green Zone: I Am Doing Well Today ActionsAl TheóNo ratings yet
- GRD HeimlichDocument1 pageGRD HeimlichAl TheóNo ratings yet
- Week 13 CaseDocument1 pageWeek 13 CaseAl TheóNo ratings yet
- ARTILLO-FDAR Nurses NotesDocument2 pagesARTILLO-FDAR Nurses NotesAl TheóNo ratings yet
- Case Scenario 3 RosellaDocument2 pagesCase Scenario 3 RosellaAl TheóNo ratings yet
- Orion Healing 28 Day Renew-RevitalizeDocument12 pagesOrion Healing 28 Day Renew-Revitalizeorionhealing24No ratings yet
- Postal Holiday Homes - ListDocument6 pagesPostal Holiday Homes - ListShatabdi RanoNo ratings yet
- Present PerfectDocument1 pagePresent PerfectFrancs Fuentes100% (1)
- Bishop's Stories - AllDocument260 pagesBishop's Stories - AllJooms Dru50% (2)
- Location Strategy PuneDocument14 pagesLocation Strategy PuneSACHIN MANGALENo ratings yet
- Our Lighthouse: Physical Wellness - Volume 2Document6 pagesOur Lighthouse: Physical Wellness - Volume 2testing1 xtbills1No ratings yet
- Unit 6 - Passive and Causative.Document16 pagesUnit 6 - Passive and Causative.FstNo ratings yet
- HackJournal 4 05Document20 pagesHackJournal 4 05Chorch GimenezNo ratings yet
- Japan Food Service - Hotel Restaurant Institutional Japan HRI Food (PDFDrive)Document31 pagesJapan Food Service - Hotel Restaurant Institutional Japan HRI Food (PDFDrive)Sakesh DhakalNo ratings yet
- Us English 2024Document11 pagesUs English 2024yuniati668No ratings yet
- 3.3.1 Prepare and Serve Coffee and BeveragesDocument4 pages3.3.1 Prepare and Serve Coffee and BeveragesDarvin San PedroNo ratings yet
- Ishara Et Al. 2022Document13 pagesIshara Et Al. 2022claudeNo ratings yet
- Past Simple ExercisesDocument9 pagesPast Simple ExercisesCatalina GabilánNo ratings yet
- Request Letter (Information) : A7/A Zirkon Street, Section 7, 40000 Shah Alam, SelangorDocument2 pagesRequest Letter (Information) : A7/A Zirkon Street, Section 7, 40000 Shah Alam, SelangorVasunNo ratings yet
- BuchiDocument12 pagesBuchilouiege banasNo ratings yet
- Cookworks Mini OvenDocument9 pagesCookworks Mini Ovensum0n3No ratings yet
- Hnology and Livelihood Education: Quarter 1 - Module 2: CookeryDocument22 pagesHnology and Livelihood Education: Quarter 1 - Module 2: CookeryMark Zanne Emia100% (2)
- Full Blast - British - Level - B1+ - Tests - Midterm - Mod - 1-6Document9 pagesFull Blast - British - Level - B1+ - Tests - Midterm - Mod - 1-6Marco AntonioNo ratings yet
- Alphatec Solvex 37 185 Pds UsDocument2 pagesAlphatec Solvex 37 185 Pds Uskris murthiNo ratings yet
- Sınıf İngilizce: Movies - 2Document2 pagesSınıf İngilizce: Movies - 2İlknur DoğanNo ratings yet
- How To Start A Hot Dog Stand - Free GuideDocument43 pagesHow To Start A Hot Dog Stand - Free Guidesteve184837550% (2)
- Rate List (07.07.2023) SouthDocument4 pagesRate List (07.07.2023) Southsubra1032No ratings yet
- MKT465 Gods Own ChipsDocument17 pagesMKT465 Gods Own ChipstinntinnNo ratings yet
- Downloaded PDFDocument93 pagesDownloaded PDFlithium jay litamNo ratings yet
- Kill To Eat - Oodgeroo NoonuccalDocument2 pagesKill To Eat - Oodgeroo NoonuccalAgustín AlemNo ratings yet
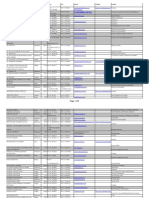
- Company City Phone Fax Email Website Product P.O. Box: Page 1 of 8Document8 pagesCompany City Phone Fax Email Website Product P.O. Box: Page 1 of 8venkwok_sghcableNo ratings yet
- FCE Test Unit 5Document4 pagesFCE Test Unit 5Said Kapanak100% (1)
- 5-ILVE Operations ManualDocument29 pages5-ILVE Operations ManualCharles LeeNo ratings yet
- BPP 1Q QuestionnaireDocument5 pagesBPP 1Q QuestionnaireAron paul San Miguel100% (1)
- Reading Practice School Lunch Menu WorksheetDocument4 pagesReading Practice School Lunch Menu WorksheetPaula GimNo ratings yet