You might also like
- Ocular Pathology Case Reviews - Azari, Amir (SRG) PDFDocument423 pagesOcular Pathology Case Reviews - Azari, Amir (SRG) PDFRamiro Calcina100% (1)
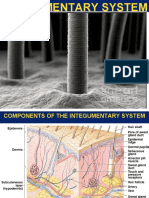
- Integumentary System ReviewerDocument12 pagesIntegumentary System ReviewerLly Isidoro100% (2)
- Skin Disorders and Diseases: Chapter OutlineDocument22 pagesSkin Disorders and Diseases: Chapter Outlinejessafesalazar100% (1)
- Inflammatory Diseases of The Skin: M. Angelica Selim, M.D. Dermatopathology Unit Pathology DepartmentDocument53 pagesInflammatory Diseases of The Skin: M. Angelica Selim, M.D. Dermatopathology Unit Pathology DepartmentIsaac MaderoNo ratings yet
- Topic 5 & 6Document18 pagesTopic 5 & 6PhoebeNo ratings yet
- Zoology Lecture (Reviewer)Document4 pagesZoology Lecture (Reviewer)Maria GrasyaNo ratings yet
- Integumentary System - ANAPHYDocument7 pagesIntegumentary System - ANAPHYmariaNo ratings yet
- Integumentary System 1Document12 pagesIntegumentary System 1Akemi LeeNo ratings yet
- Integumentary SystemDocument9 pagesIntegumentary SystemCelyn DeañoNo ratings yet
- A. I. Ii. Iii.: Protection. Serving As The Covering of The Body, ItDocument9 pagesA. I. Ii. Iii.: Protection. Serving As The Covering of The Body, ItFrancis100% (1)
- Burns SemDocument29 pagesBurns SemEsther Marie SazonNo ratings yet
- Anaphy ReviewerDocument8 pagesAnaphy ReviewerMark GonzalesNo ratings yet
- Sistem Integumen: Kulit & DerivatnyaDocument25 pagesSistem Integumen: Kulit & DerivatnyaUniversal DiscoveringNo ratings yet
- 5 Integumentary SystemDocument5 pages5 Integumentary SystemEly FructuosoNo ratings yet
- Anaphy - IntegumentaryDocument4 pagesAnaphy - IntegumentaryYo1No ratings yet
- Layers of The SkinDocument7 pagesLayers of The SkinJeah LourraineNo ratings yet
- Integumentary SystemDocument56 pagesIntegumentary SystemSamantha Kaye ReclaNo ratings yet
- Structure of Skin, Skin Problems, Hair Structure and Hair Growth CycleDocument8 pagesStructure of Skin, Skin Problems, Hair Structure and Hair Growth CycleRakshita GroverNo ratings yet
- Integumentary SystemDocument3 pagesIntegumentary SystemCarmela Cordon FelixNo ratings yet
- PowerPoint - Presentation - About - Integumentary - SystemDocument27 pagesPowerPoint - Presentation - About - Integumentary - SystemPrayl Hope NapanoNo ratings yet
- A-P Chapter 5 Integumentary SystemDocument19 pagesA-P Chapter 5 Integumentary SystemMONIQUE VELASCO100% (1)
- Anaphy Lec Midterm ReviewerDocument27 pagesAnaphy Lec Midterm ReviewerFAITH EFONDONo ratings yet
- Integumentary ReviewerDocument3 pagesIntegumentary ReviewerJomar ManalangNo ratings yet
- Lecture 1Document30 pagesLecture 1Dr. Rabail MalikNo ratings yet
- Practical Part: Associate Professor of Anatomy and HistologyDocument39 pagesPractical Part: Associate Professor of Anatomy and HistologyRuby BhattyNo ratings yet
- Reviewer Integumentary DigestiveDocument11 pagesReviewer Integumentary DigestiveMariah Alexa LibaoNo ratings yet
- Cells Are Scattered Around: Pigment That Affords The Skin Some Protection Against Ultraviolet RadiationDocument5 pagesCells Are Scattered Around: Pigment That Affords The Skin Some Protection Against Ultraviolet RadiationDimple Lexiry GloriaNo ratings yet
- Integumentary SystemDocument74 pagesIntegumentary SystemririyoruNo ratings yet
- Anaphy MidtermsDocument28 pagesAnaphy MidtermsxeanNo ratings yet
- BIOL 2210 Chapter 6, Integument System-1Document15 pagesBIOL 2210 Chapter 6, Integument System-1KellyPatrick SpencerNo ratings yet
- Anatomy & Physiology Reviewer: Stratum GerminativumDocument5 pagesAnatomy & Physiology Reviewer: Stratum GerminativumChris Deinielle Marcoleta SumaoangNo ratings yet
- Dermatology NotesDocument37 pagesDermatology NotesTamilmani n.mNo ratings yet
- Histology: Nails Skin Glands Skin Repair Presented by Sultan Hafiz Adil Group 12Document15 pagesHistology: Nails Skin Glands Skin Repair Presented by Sultan Hafiz Adil Group 12Hafiz AdilNo ratings yet
- MODULE 4 Ana PhysioDocument11 pagesMODULE 4 Ana Physiojoshua ordenaNo ratings yet
- Basic DermatologyDocument43 pagesBasic Dermatologyarslan63637363No ratings yet
- UntitledDocument59 pagesUntitledKenneth PalermoNo ratings yet
- The SkinDocument3 pagesThe SkinStargazer FrouxNo ratings yet
- Chapter 5 - Integumentary SystemDocument5 pagesChapter 5 - Integumentary SystemLora Mae Delos SantosNo ratings yet
- Skin Histology 1Document72 pagesSkin Histology 1ace danielNo ratings yet
- And Its Appendages: Dr. Archana Rani Associate Professor Department of Anatomy KGMU UP, LucknowDocument44 pagesAnd Its Appendages: Dr. Archana Rani Associate Professor Department of Anatomy KGMU UP, LucknowCesar Ivan Ruiz DiazNo ratings yet
- Parts of Human SkinDocument1 pageParts of Human SkinDivine SantotomeNo ratings yet
- Body Support ModuleDocument5 pagesBody Support ModuleBen MoldenhaurNo ratings yet
- Learning Outcomes:: Layers of The SkinDocument4 pagesLearning Outcomes:: Layers of The SkinRumaisa ChowdhuryNo ratings yet
- The Skin (Anaphy)Document2 pagesThe Skin (Anaphy)ALEXANDRA COLLEEN ALEGRENo ratings yet
- Development of IntegumentaryDocument5 pagesDevelopment of IntegumentaryAkachukwu ObunikeNo ratings yet
- Bercadez, Ma. Benita GROUP 1 - BSN 1 I - Laboratory Exercise No. 4 5Document15 pagesBercadez, Ma. Benita GROUP 1 - BSN 1 I - Laboratory Exercise No. 4 5Ma. Benita BercadezNo ratings yet
- Functions of Integumentary SystemDocument5 pagesFunctions of Integumentary SystemgrapikmsNo ratings yet
- 001 - Skin AnatomyDocument46 pages001 - Skin AnatomyLucas Victor AlmeidaNo ratings yet
- INTEGUMENTARY SYsTEMDocument42 pagesINTEGUMENTARY SYsTEMGabNo ratings yet
- Integumentary System - Anatomy and PhysiologyDocument2 pagesIntegumentary System - Anatomy and PhysiologyHan CallejaNo ratings yet
- Integumentary System TransesDocument5 pagesIntegumentary System Transesadrielvamos28No ratings yet
- جلدية Coppy AllowedDocument118 pagesجلدية Coppy AllowedAssssssNo ratings yet
- Epidermis: - Five Sub-Layers of The EpidermisDocument7 pagesEpidermis: - Five Sub-Layers of The EpidermisPau De GuzmanNo ratings yet
- Biol163 Integumentary SystemDocument46 pagesBiol163 Integumentary SystemGladdyll Raico DizonNo ratings yet
- Histology of The SkinDocument32 pagesHistology of The SkinAbdishakur AdanNo ratings yet
- The Skin Structure: Presentation ofDocument35 pagesThe Skin Structure: Presentation ofdimple bachkaniwalaNo ratings yet
- Corneum and Is Directly Exposed To TheDocument3 pagesCorneum and Is Directly Exposed To Theydnic alykPNo ratings yet
- Integumentary 2Document14 pagesIntegumentary 2Grace JaimeNo ratings yet
- AP 5 IntegumentaryDocument6 pagesAP 5 Integumentaryneriza bloreciaNo ratings yet
- Nursing AnaPhy Integumentary SystemDocument22 pagesNursing AnaPhy Integumentary SystemGail Chantel Spring PerlasNo ratings yet
- CH 5: Integumentary SystemDocument36 pagesCH 5: Integumentary SystemHurtlock HurtlockNo ratings yet
- Chemical Leukoderma To Hair DyeDocument2 pagesChemical Leukoderma To Hair DyeCHONG WEI SHENGNo ratings yet
- Dermatologic Manifestations of Miliaria Workup - Laboratory Studies, Imaging Studies, Histologic Findings 4Document3 pagesDermatologic Manifestations of Miliaria Workup - Laboratory Studies, Imaging Studies, Histologic Findings 4Norhalisya UtamiNo ratings yet
- Microbial Diseases of Skin & EyesDocument29 pagesMicrobial Diseases of Skin & Eyesbriterry2008No ratings yet
- MATH187 Answer 3Document5 pagesMATH187 Answer 3Brilian BowoNo ratings yet
- Incontinence Associated Dermatitis Made EasyDocument6 pagesIncontinence Associated Dermatitis Made EasyRismaNo ratings yet
- Іst degree of complexityDocument45 pagesІst degree of complexityMohammad MohyeddienNo ratings yet
- Skin & STDDocument8 pagesSkin & STDskNo ratings yet
- Dermatitits StasisDocument11 pagesDermatitits StasisRiyan TjahyaNo ratings yet
- Elementary Skin LesionsDocument5 pagesElementary Skin LesionsYdeli DetanNo ratings yet
- BC-NSG-SKC201 Session 2 - Health Assessment Part 1Document153 pagesBC-NSG-SKC201 Session 2 - Health Assessment Part 1Precious C. MamaradloNo ratings yet
- Dermatology MDMSDocument64 pagesDermatology MDMSDipesh Shrestha0% (1)
- Fitzpatricks Dermatology 9th Edition 3121Document1 pageFitzpatricks Dermatology 9th Edition 3121DennisSujayaNo ratings yet
- Differential Diagnosis Oral LesionsDocument41 pagesDifferential Diagnosis Oral Lesionssgoeldoc_550661200No ratings yet
- Stanford Medicine25 - Dermatology Exam - Learning The LanguageDocument16 pagesStanford Medicine25 - Dermatology Exam - Learning The LanguageOlaNo ratings yet
- Fever and Rash: Dr. Karwan Hawez Sulaiman MBCHB, Ficms, FM Family Medicine Specialist College of MedicineDocument20 pagesFever and Rash: Dr. Karwan Hawez Sulaiman MBCHB, Ficms, FM Family Medicine Specialist College of MedicinesamiNo ratings yet
- ERMP 2021, Part II-1Document16 pagesERMP 2021, Part II-1kude kulayeNo ratings yet
- Health AssessmentDocument160 pagesHealth AssessmentJerome TingNo ratings yet
- Mycobacterial Granulomas, Opportunistic Granulomas and Other Bacterial DiseasesDocument25 pagesMycobacterial Granulomas, Opportunistic Granulomas and Other Bacterial DiseasesBiancaNo ratings yet
- Skinhairnail Ass 1Document43 pagesSkinhairnail Ass 1Airene Aquino BusaniaNo ratings yet
- Fowl PoxDocument17 pagesFowl PoxUsman KhalidNo ratings yet
- Dissertation PsoriasisDocument7 pagesDissertation PsoriasisPayingSomeoneToWriteAPaperSingapore100% (1)
- Pathology of Integument System: Djoko Legowo, Mkes., DRHDocument135 pagesPathology of Integument System: Djoko Legowo, Mkes., DRHPilar Mitra QurbanNo ratings yet
- Dermatological Manifestations in AyurvedaDocument18 pagesDermatological Manifestations in AyurvedaFarooq Bin MahfoozNo ratings yet
- Lichen Simplex ChronicusDocument10 pagesLichen Simplex ChronicusGita PermatasariNo ratings yet
- GMFD Year 234 - 2 PDFDocument247 pagesGMFD Year 234 - 2 PDFHussein NazzalNo ratings yet
- Skin Examination: Dr. Ploesteanu Rodica Emergency Hospital Sfantul Pantelimon" 2018Document167 pagesSkin Examination: Dr. Ploesteanu Rodica Emergency Hospital Sfantul Pantelimon" 2018Arleen MatincaNo ratings yet
- Syllabus Fellowcosmet 22122016 PDFDocument6 pagesSyllabus Fellowcosmet 22122016 PDFKinger KingerNo ratings yet
- Scaling & Crusting Skin Disease: Comparative ImageryDocument4 pagesScaling & Crusting Skin Disease: Comparative Imageryavenger 2No ratings yet