You might also like
- 2020 Acls Megacode Testing Scenarios - 2Document13 pages2020 Acls Megacode Testing Scenarios - 2Dr. Saqib RazaNo ratings yet
- Care For Mechanical VentilationDocument14 pagesCare For Mechanical Ventilationmaeya186135100% (3)
- Bronchitis Care PlanDocument2 pagesBronchitis Care PlanNatalié Dee86% (21)
- Code Blue Running SheetDocument2 pagesCode Blue Running Sheetenumula kumar100% (12)
- DR Supriyanto Spa SMF Kes Anak Rsms PurwokertoDocument62 pagesDR Supriyanto Spa SMF Kes Anak Rsms PurwokertoSylvia Delti ElviraNo ratings yet
- Adult Pediatric Code Blue Documentation Form UCM - 479871Document3 pagesAdult Pediatric Code Blue Documentation Form UCM - 479871rubertusedy100% (3)
- AHA ACLS Megacode Scenarios PDFDocument6 pagesAHA ACLS Megacode Scenarios PDFNavin ShawnNo ratings yet
- Respiratory Disorders NCLEXDocument22 pagesRespiratory Disorders NCLEXPotchiee Pfizer67% (3)
- Tramadol + ParacetamolDocument4 pagesTramadol + ParacetamolFaye Andrea Francisco100% (2)
- Lung AuscultogramDocument1 pageLung AuscultogramJacklyn M. oNo ratings yet
- ABG Interpretation Made EasyDocument5 pagesABG Interpretation Made EasyChris Chan100% (2)
- Sample: Reading Sub-Test - Text Booklet: Part ADocument24 pagesSample: Reading Sub-Test - Text Booklet: Part AAlwin BrightNo ratings yet
- City College of San Francisco Vocational Nursing Program: Medical Surgical Care Plan Date DateDocument4 pagesCity College of San Francisco Vocational Nursing Program: Medical Surgical Care Plan Date DateShanice CapiliNo ratings yet
- The Anesthesia ChartDocument39 pagesThe Anesthesia Chartnicolinna2000yahoo.comNo ratings yet
- RM PT Age. Ethnicity: Initials M / F Admit Date: Physicians &/or Nurse: Adm. Diagnosis: Health HistoryDocument2 pagesRM PT Age. Ethnicity: Initials M / F Admit Date: Physicians &/or Nurse: Adm. Diagnosis: Health HistoryTi LunNo ratings yet
- Emergency Department Bronchiolitis Care Guideline: Inclusion CriteriaDocument3 pagesEmergency Department Bronchiolitis Care Guideline: Inclusion CriteriaPatricia KoikyNo ratings yet
- PCARE 107 Assignment Chapter 11 Warm-Up Activity: Level of Care Staffing Intervention Package Drugs/Meds EquipmentsDocument3 pagesPCARE 107 Assignment Chapter 11 Warm-Up Activity: Level of Care Staffing Intervention Package Drugs/Meds EquipmentsLaica Mae HusanaNo ratings yet
- Final Pneumonia AlgorithmDocument1 pageFinal Pneumonia AlgorithmWajih FarhanNo ratings yet
- TDM Monitoring Sampling Guideline Form 2022 Iso CodeDocument2 pagesTDM Monitoring Sampling Guideline Form 2022 Iso Codenur nadirahNo ratings yet
- Regis Mani AAOMPT Poster 2008Document1 pageRegis Mani AAOMPT Poster 2008smokey73No ratings yet
- Gina Sa Final WmsDocument21 pagesGina Sa Final WmsCrisell DonathNo ratings yet
- Transition Care ModelDocument2 pagesTransition Care ModelErhyqck De GuzmanNo ratings yet
- 01 Sick Bird SyndromeDocument1 page01 Sick Bird SyndromeAli BakNo ratings yet
- Smart Independent Dependent Collaborative: General Malvar ST., Davao CityDocument2 pagesSmart Independent Dependent Collaborative: General Malvar ST., Davao CityKhim BalcitaNo ratings yet
- NCCN Head-And-neck 2020 HipofaringeDocument11 pagesNCCN Head-And-neck 2020 Hipofaringed.ayala1006No ratings yet
- نسخة Weekly Report Nur 423 2021Document29 pagesنسخة Weekly Report Nur 423 2021raneemNo ratings yet
- Checklist IOT UTIA HIBA Feb2020Document2 pagesChecklist IOT UTIA HIBA Feb2020Juan FiigueerooaNo ratings yet
- Persiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairDocument5 pagesPersiapan Osce Nasional: Dept. Obstetri Dan Ginekologi FK UnairYanis Widhiya NingrumNo ratings yet
- All Ima DoctorsDocument35 pagesAll Ima DoctorssrisaravananNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument62 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineIrsyah Dwi RNo ratings yet
- (According To Priority) (Cues & Evidences/ Objective & Subjective) (Objectives-Long Term & Short Term)Document1 page(According To Priority) (Cues & Evidences/ Objective & Subjective) (Objectives-Long Term & Short Term)opxNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument71 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineRosyid PrasetyoNo ratings yet
- This Chart Is Printed With The Permission of The Author, Tom BallesDocument5 pagesThis Chart Is Printed With The Permission of The Author, Tom BallesIdannNo ratings yet
- Team Multi Rescuer, Code Blue System RSUD ENDEDocument35 pagesTeam Multi Rescuer, Code Blue System RSUD ENDEMarsel DonaNo ratings yet
- Egla Ramirez 11/3/21 LG III Stage II Grade B Carolyn C.: Student Daily Clinic Self EvaluationDocument1 pageEgla Ramirez 11/3/21 LG III Stage II Grade B Carolyn C.: Student Daily Clinic Self Evaluationapi-547172617No ratings yet
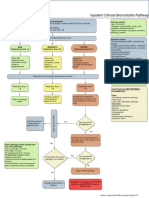
- Bronchiolitis Pathway InpatientDocument1 pageBronchiolitis Pathway Inpatientd'Agung NugrohoNo ratings yet
- Update Prime Emergency Unit - MEDIKA 2017Document34 pagesUpdate Prime Emergency Unit - MEDIKA 2017adiborthopaediNo ratings yet
- Irst Esponders: Dario GonzalezDocument16 pagesIrst Esponders: Dario GonzalezAlha MidaNo ratings yet
- Airway & Breathing ManagementDocument75 pagesAirway & Breathing ManagementirmayaniNo ratings yet
- Inpatientpathway PDFDocument2 pagesInpatientpathway PDFLuis Fernando SaraviaNo ratings yet
- Managed Clinical Network For Stroke Stroke Unit Protocol/GuidelineDocument5 pagesManaged Clinical Network For Stroke Stroke Unit Protocol/GuidelineRicky Cik KoharNo ratings yet
- ESC - Diagnosis of HFDocument29 pagesESC - Diagnosis of HFDumora FatmaNo ratings yet
- COVID Positive/PUI: PAPR Prioritization MatrixDocument1 pageCOVID Positive/PUI: PAPR Prioritization MatrixJesse M. MassieNo ratings yet
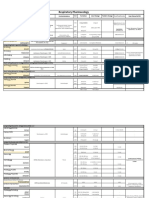
- Respiratory Pharmacology: Accuneb Proair Proventil Proair Respiclick VentolinDocument3 pagesRespiratory Pharmacology: Accuneb Proair Proventil Proair Respiclick VentolinRobert BrowningNo ratings yet
- TRIAGEDocument55 pagesTRIAGELaveena AswaleNo ratings yet
- Adenosine 8-28-22Document1 pageAdenosine 8-28-22ladawskiNo ratings yet
- Joshua Taylor 12/2/2021 Mod Iii/ Heavy Iii Carmon S.: Disclosed and Reinforced The Use of Brushing DailyDocument1 pageJoshua Taylor 12/2/2021 Mod Iii/ Heavy Iii Carmon S.: Disclosed and Reinforced The Use of Brushing Dailyapi-547172617No ratings yet
- Name of Drug Classificatio N Mechanism of Action Indications Contraindication S Adverse Effects Side EffectsDocument7 pagesName of Drug Classificatio N Mechanism of Action Indications Contraindication S Adverse Effects Side EffectsHilario. Hayascent.Reign.M.No ratings yet
- HiraDocument1 pageHirajanisha11No ratings yet
- ABCDE Table Crib SheetDocument1 pageABCDE Table Crib SheetdaeyangmgrNo ratings yet
- UNC ED Code Stroke Pathway 9 2016 FINALDocument2 pagesUNC ED Code Stroke Pathway 9 2016 FINALJackNo ratings yet
- Code Blue DocumentationDocument2 pagesCode Blue Documentationtuti utamaNo ratings yet
- Nursing Care Record: - Pain AssessmentDocument2 pagesNursing Care Record: - Pain AssessmentMohamed MahmoudNo ratings yet
- First RespondersDocument16 pagesFirst RespondersydtrgnNo ratings yet
- 2.3 Cập nhật chẩn đoán và điều trị suy tim-14-11-2021 - .pptx 2Document1 page2.3 Cập nhật chẩn đoán và điều trị suy tim-14-11-2021 - .pptx 2tranlekieutrinh166No ratings yet
- Time To ACT Proforma - Feb 2021 - 0 - 0Document2 pagesTime To ACT Proforma - Feb 2021 - 0 - 0echa okta anggrainiNo ratings yet
- ICU One Pager - Pulmonary Embolism RX PDFDocument1 pageICU One Pager - Pulmonary Embolism RX PDFAbdul RaufNo ratings yet
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Suez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)Document18 pagesSuez Canal University/ Faculty of Nursing (Medical Surgical Nursing/ Clinical Assessment Sheet 2 Year 2020/2021)طالب جامعة100% (1)
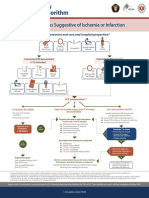
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument8 pagesSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionNugroho TeguhNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- Family Medicine LectureDocument24 pagesFamily Medicine Lectureapi-549451092No ratings yet
- ProtocolDocument27 pagesProtocolDk YadavNo ratings yet
- Covid Flow ChartDocument1 pageCovid Flow ChartPeeaar Green Energy SolutionsNo ratings yet
- Monitoring Mechanical Ventilation Using Ventilator WaveformsFrom EverandMonitoring Mechanical Ventilation Using Ventilator WaveformsNo ratings yet
- Pengaruh Kombinasi Pursed-Lip Breathing Dan Guided Imagery Music TerhadapDocument7 pagesPengaruh Kombinasi Pursed-Lip Breathing Dan Guided Imagery Music TerhadapFaisal AmirNo ratings yet
- Aspirasi Pneumonia Cetak RDocument51 pagesAspirasi Pneumonia Cetak RFadhli Abd EssentialNo ratings yet
- Entrenar Miusculatura Respiratoria Adiciona Beneficio Durante Rehabiltiacion en Pacientes EpidDocument13 pagesEntrenar Miusculatura Respiratoria Adiciona Beneficio Durante Rehabiltiacion en Pacientes Epidignacio sepulvedaNo ratings yet
- Format Laporan Ispa Juni 2019Document3 pagesFormat Laporan Ispa Juni 2019Erpiani Mardin LNo ratings yet
- Kurikulum Vitae: DR Finny Fitry Yani Spa (K)Document21 pagesKurikulum Vitae: DR Finny Fitry Yani Spa (K)Anonymous ujOv31SNo ratings yet
- Respiratory Effects of Amyotrophic Lateral Sclerosis, Problems and SolutionsDocument14 pagesRespiratory Effects of Amyotrophic Lateral Sclerosis, Problems and SolutionsMarcelaNo ratings yet
- Evita XL ModesDocument2 pagesEvita XL ModesJohn JohnsonNo ratings yet
- Telangana Ehs HospitalsDocument9 pagesTelangana Ehs HospitalsAkbar MohammedNo ratings yet
- New Trends in Mechanical VentilationDocument4 pagesNew Trends in Mechanical Ventilationashley_castro_4No ratings yet
- Clinical Manifestations and Diagnosis of Idiopathic Pulmonary Fibrosis - UpToDateDocument23 pagesClinical Manifestations and Diagnosis of Idiopathic Pulmonary Fibrosis - UpToDateTatiana Valencia CastañoNo ratings yet
- Pediatric Airway Card (Dual)Document1 pagePediatric Airway Card (Dual)Brian CloughNo ratings yet
- PulmonologyDocument175 pagesPulmonologyJohanna GarciaNo ratings yet
- Weaning Patients With Obesity From Ventilatory Support: ReviewDocument9 pagesWeaning Patients With Obesity From Ventilatory Support: ReviewGian CarloNo ratings yet
- General & Multi Speciality Hospitals: Iyyappan K 9844535502Document17 pagesGeneral & Multi Speciality Hospitals: Iyyappan K 9844535502Nandeesh SNo ratings yet
- Teaching Slide Set 2019: Global Initiative For Chronic Obstructive Lung Disease (Gold)Document128 pagesTeaching Slide Set 2019: Global Initiative For Chronic Obstructive Lung Disease (Gold)Gevi Lia SariNo ratings yet
- Pediatric Noninvasive Ventilation: Cathy HautDocument7 pagesPediatric Noninvasive Ventilation: Cathy HautsiputamaliaputriNo ratings yet
- Respi Medsurg TestDocument17 pagesRespi Medsurg TestPINKY CUARESMANo ratings yet
- El Flujómetro de Wright - Una Herramienta Indispensable en La Práctica Ambulatoria Sepulveda 2004Document5 pagesEl Flujómetro de Wright - Una Herramienta Indispensable en La Práctica Ambulatoria Sepulveda 2004paola vanessa magdalena pormaNo ratings yet
- Angka Tahan Hidup Penderita Kanker Paru Bukan KarsinomaDocument8 pagesAngka Tahan Hidup Penderita Kanker Paru Bukan KarsinomaFebrinaHutasosweetNo ratings yet
- Inpatient Asthma: Clinical PathwayDocument9 pagesInpatient Asthma: Clinical PathwaydedeNo ratings yet
- Spirometry: An Essential Clinical MeasurementDocument5 pagesSpirometry: An Essential Clinical MeasurementMarc AbellaNo ratings yet
- Thesis Topics For MD Respiratory MedicineDocument7 pagesThesis Topics For MD Respiratory Medicinelindseyriverakansascity100% (2)
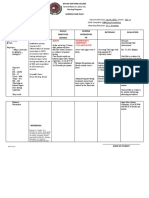
- Assessment Diagnosis Planning Intervention Rationale Evaluation Short Term: Independent: Independent: Short TermDocument2 pagesAssessment Diagnosis Planning Intervention Rationale Evaluation Short Term: Independent: Independent: Short TermDYNA GISELLE ROMERONo ratings yet
- Bhs Inggris AsthmaDocument7 pagesBhs Inggris AsthmaAnita nur hidayatiNo ratings yet