You might also like
- Oral Manifestations of Gardner's Syndrome in Young Patients: Report of Three CasesDocument5 pagesOral Manifestations of Gardner's Syndrome in Young Patients: Report of Three Casesromy100% (1)
- Us B2B With Contact Person Info - IiDocument18 pagesUs B2B With Contact Person Info - Iiraymond arabeNo ratings yet
- Cytoreductive Surgery and IntraperitonealDocument11 pagesCytoreductive Surgery and IntraperitonealJorge FallasNo ratings yet
- Acs 06 02 167Document8 pagesAcs 06 02 167MixalisKaplanisNo ratings yet
- The Incidence and Risk of Early Postoperative Small Bowel Obstruction After Laparoscopic Resection For Colorectal Cancer 2014Document7 pagesThe Incidence and Risk of Early Postoperative Small Bowel Obstruction After Laparoscopic Resection For Colorectal Cancer 2014alemago90No ratings yet
- A Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerDocument9 pagesA Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerFarizka Dwinda HNo ratings yet
- Long-Term Outcomes of Primary Endoscopic Resection Vs Surgery For T1Document16 pagesLong-Term Outcomes of Primary Endoscopic Resection Vs Surgery For T1ellya zalfaNo ratings yet
- Laparoscopic Resection of Rectal CancerDocument4 pagesLaparoscopic Resection of Rectal CancerhoangducnamNo ratings yet
- A Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerDocument9 pagesA Randomized Trial of Laparoscopic Versus Open Surgery For Rectal CancerOtoyGethuNo ratings yet
- Glandula SalivarDocument8 pagesGlandula SalivarporsanimedNo ratings yet
- 2021 Recomendations For Srveillance and Manangemnt of Recurrent Esophageal Cancer Following Endoscopic TherapiesDocument12 pages2021 Recomendations For Srveillance and Manangemnt of Recurrent Esophageal Cancer Following Endoscopic TherapiesykommNo ratings yet
- P. Wang Et Al.2019Document6 pagesP. Wang Et Al.2019Mai M. AlshalNo ratings yet
- Incidental Gallbladder Cancer. Residual Cancer Discovered at Oncologic Extended Resection Determines Outcome. A Report From High - and Low-IncidencDocument10 pagesIncidental Gallbladder Cancer. Residual Cancer Discovered at Oncologic Extended Resection Determines Outcome. A Report From High - and Low-IncidencCarlos SotoNo ratings yet
- Baek 2017Document10 pagesBaek 2017witaNo ratings yet
- Abdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceDocument8 pagesAbdominoperineal Resection For Squamous Cell Anal Carcinoma: Survival and Risk Factors For RecurrenceWitrisyah PutriNo ratings yet
- Abstract 2015 in Surgery PDFDocument281 pagesAbstract 2015 in Surgery PDFDrAmmar MagdyNo ratings yet
- 10 1111@codi 15424Document22 pages10 1111@codi 15424yongky sugandaNo ratings yet
- Esmo Guidline: Presentasi Oleh: Dr.I Nyoman Dwija Putra SP.BDocument45 pagesEsmo Guidline: Presentasi Oleh: Dr.I Nyoman Dwija Putra SP.BIrbah NabilaNo ratings yet
- Clinical Outcomes of Laparoscopic Surgery For Transverse and Descending Colon Cancers in A Community SettingDocument6 pagesClinical Outcomes of Laparoscopic Surgery For Transverse and Descending Colon Cancers in A Community SettingpingusNo ratings yet
- 014 - Primary-Colorectal-Cancer - 2023 - Surgical-Oncology-Clinics-of-North-AmericaDocument16 pages014 - Primary-Colorectal-Cancer - 2023 - Surgical-Oncology-Clinics-of-North-AmericaDr-Mohammad Ali-Fayiz Al TamimiNo ratings yet
- Short-Term Surgical and Long-Term Survival Outcomes After Laparoscopic Distal Gastrectomy With D Lymphadenectomy For Gastric CancerDocument7 pagesShort-Term Surgical and Long-Term Survival Outcomes After Laparoscopic Distal Gastrectomy With D Lymphadenectomy For Gastric CancerThế VũNo ratings yet
- Reducing Recurrence Rates in Non-Muscle Invasive Bladder CancerDocument1 pageReducing Recurrence Rates in Non-Muscle Invasive Bladder CancerOkki Masitah Syahfitri NasutionNo ratings yet
- Modified Technique of Radical Inguinal Lymphadenectomy For Penile Carcinoma: Morbidity and OutcomeDocument7 pagesModified Technique of Radical Inguinal Lymphadenectomy For Penile Carcinoma: Morbidity and OutcomeAlwin PrasetyaNo ratings yet
- AppendicitisDocument3 pagesAppendicitisRindayu Julianti NurmanNo ratings yet
- LAPAROSDocument13 pagesLAPAROSpancholin_9No ratings yet
- Astec1 PDFDocument29 pagesAstec1 PDFSohailKhanNo ratings yet
- J Gastrointest SurgDocument6 pagesJ Gastrointest SurgAnitei GabrielaNo ratings yet
- Nej Mo A 1414882Document9 pagesNej Mo A 1414882Corina Hagiu-RaduNo ratings yet
- HPCDocument6 pagesHPCPrathita AmandaNo ratings yet
- Soria 2019Document7 pagesSoria 2019Dr. Alexandre SatoNo ratings yet
- Analysis of The Risk Factors of Untransplantable Recurrence After Primary Curative Resection For Patients With Hepatocellular CarcinomaDocument8 pagesAnalysis of The Risk Factors of Untransplantable Recurrence After Primary Curative Resection For Patients With Hepatocellular CarcinomaJoão Gabriel Ferreira ArgondizziNo ratings yet
- Lessismore:Minimally Invasiveandquality Surgicalmanagementof GynecologiccancerDocument12 pagesLessismore:Minimally Invasiveandquality Surgicalmanagementof GynecologiccancerNita AgarwalNo ratings yet
- Research Article: Characteristics of Patients With Colonic Polyps Requiring Segmental ResectionDocument7 pagesResearch Article: Characteristics of Patients With Colonic Polyps Requiring Segmental ResectionAkiko Syawalidhany TahirNo ratings yet
- Wimmer2020 Article ImpactOfSurgicalMarginsInBreasDocument8 pagesWimmer2020 Article ImpactOfSurgicalMarginsInBreasNelly ChacónNo ratings yet
- Laparoscopic-Assisted Radical Vaginal Hysterectomy (LARVH) : Prospective Evaluation of 200 Patients With Cervical CancerDocument7 pagesLaparoscopic-Assisted Radical Vaginal Hysterectomy (LARVH) : Prospective Evaluation of 200 Patients With Cervical CancerHari NugrohoNo ratings yet
- Adenocarcinoma of The Gastroesophageal JunctionDocument8 pagesAdenocarcinoma of The Gastroesophageal JunctionKiara GovenderNo ratings yet
- SMJ 60 247Document6 pagesSMJ 60 247Chee Yung NgNo ratings yet
- Article - Laparoscopic Versus Open Surgery For Rectal Cancer (COLOR II) - Short-Term Outcomes of A Randomised, Phase 3 Trial - 2013Document9 pagesArticle - Laparoscopic Versus Open Surgery For Rectal Cancer (COLOR II) - Short-Term Outcomes of A Randomised, Phase 3 Trial - 2013Trí Cương NguyễnNo ratings yet
- Minimally Invasive Surgery For Esophageal Cancer: Review of The Literature and Institutional ExperienceDocument8 pagesMinimally Invasive Surgery For Esophageal Cancer: Review of The Literature and Institutional ExperienceNurulArifahAmirNo ratings yet
- Klatskin Tumor 2Document8 pagesKlatskin Tumor 2Florian JeffNo ratings yet
- Exact ArticleDocument6 pagesExact ArticleMuhammad WaqasNo ratings yet
- 17-09-2019 Lower GI FINALDocument32 pages17-09-2019 Lower GI FINALNaima HabibNo ratings yet
- Tratamiento Esofago Cervical Mendenhall 1994Document13 pagesTratamiento Esofago Cervical Mendenhall 1994Carlos N. Rojas PuyolNo ratings yet
- Anterior Resection With Low AnastomosisDocument10 pagesAnterior Resection With Low AnastomosisOhana S.No ratings yet
- Role of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomaDocument8 pagesRole of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomadickyaririsandyNo ratings yet
- Barton 2013Document5 pagesBarton 2013Diederick de JongNo ratings yet
- Low Anterior Resection TechniquesDocument15 pagesLow Anterior Resection Techniquesdrneeraj168No ratings yet
- Article Oesophage CorrectionDocument11 pagesArticle Oesophage CorrectionKhalilSemlaliNo ratings yet
- Controversies in Abdominoperineal Excision: Torbjörn HolmDocument19 pagesControversies in Abdominoperineal Excision: Torbjörn HolmPriscilla Rockbrand CamposNo ratings yet
- Simultaneous Versus Delayed Resection For Initially Resectable Synchronous Colorectal Cancer Liver MetastasesDocument8 pagesSimultaneous Versus Delayed Resection For Initially Resectable Synchronous Colorectal Cancer Liver MetastasesDr Shiv ChopraNo ratings yet
- A Prospective Evaluation of Serum Carcinoembryonic Antigen (CEA) Levels in The Management of Colorectal CarcinomaDocument2 pagesA Prospective Evaluation of Serum Carcinoembryonic Antigen (CEA) Levels in The Management of Colorectal CarcinomaVitjki PramadiNo ratings yet
- Worldwide Trends in Surgical Techniques in The Treatment of Esophageal and Gastroesophageal Junction CancerDocument7 pagesWorldwide Trends in Surgical Techniques in The Treatment of Esophageal and Gastroesophageal Junction CancerLuca BellaioNo ratings yet
- Bun V34N3p223Document6 pagesBun V34N3p223pingusNo ratings yet
- Managementofgastric Adenocarcinomaforgeneral Surgeons: Hisakazu HoshiDocument12 pagesManagementofgastric Adenocarcinomaforgeneral Surgeons: Hisakazu HoshiNelson William UsnayoNo ratings yet
- Kanker ParuDocument10 pagesKanker Parunovi hidayahNo ratings yet
- 1 s2.0 S1015958417305833 MainDocument7 pages1 s2.0 S1015958417305833 Mainyerich septaNo ratings yet
- RT Urothelial Carcinomas Radu MitricaDocument37 pagesRT Urothelial Carcinomas Radu MitricaStirNo ratings yet
- Retroperitoneal Nodal Metastases From Colorectal Cancer: Curable Metastases With Radical Retroperitoneal Lymphadenectomy in Selected PatientsDocument8 pagesRetroperitoneal Nodal Metastases From Colorectal Cancer: Curable Metastases With Radical Retroperitoneal Lymphadenectomy in Selected PatientsSchiopu VictorNo ratings yet
- Tratamiento Esofago Cervical Lu, 2021Document9 pagesTratamiento Esofago Cervical Lu, 2021Carlos N. Rojas PuyolNo ratings yet
- Radiotherapy of Liver CancerFrom EverandRadiotherapy of Liver CancerJinsil SeongNo ratings yet
- Endoscopic Management of Colorectal T1(SM) CarcinomaFrom EverandEndoscopic Management of Colorectal T1(SM) CarcinomaShinji TanakaNo ratings yet
- Biliopancreatic Endoscopy: Practical ApplicationFrom EverandBiliopancreatic Endoscopy: Practical ApplicationKwok-Hung LaiNo ratings yet
- Hepatitis B InfectionDocument8 pagesHepatitis B Infectionto van quyenNo ratings yet
- Gastroesophagus Reflux Disease (GERD)Document5 pagesGastroesophagus Reflux Disease (GERD)to van quyenNo ratings yet
- Helicobacter Pylori Infection and TreatmentDocument3 pagesHelicobacter Pylori Infection and Treatmentto van quyenNo ratings yet
- Causes of Vomiting and How To Treat in AdultsDocument8 pagesCauses of Vomiting and How To Treat in Adultsto van quyenNo ratings yet
- Ulcerative Colitis Viêm Loét Đ I TràngDocument12 pagesUlcerative Colitis Viêm Loét Đ I Tràngto van quyenNo ratings yet
- Endoscopy Consent Form enDocument1 pageEndoscopy Consent Form ento van quyenNo ratings yet
- Hemorrhoids DiseaseDocument3 pagesHemorrhoids Diseaseto van quyenNo ratings yet
- IBS Disease H I CH NG Ru T Kích ThíchDocument19 pagesIBS Disease H I CH NG Ru T Kích Thíchto van quyenNo ratings yet
- Hepatitis B Viêm Gan Siêu Vi BDocument4 pagesHepatitis B Viêm Gan Siêu Vi Bto van quyenNo ratings yet
- Understanding Colonoscopy ENG VERSIONDocument2 pagesUnderstanding Colonoscopy ENG VERSIONto van quyenNo ratings yet
- Irritable Bowel Syndrome H I CH NG Ru T Kích ThíchDocument3 pagesIrritable Bowel Syndrome H I CH NG Ru T Kích Thíchto van quyenNo ratings yet
- Abdomen Pain Cause Nguyên Nhân Đau B NGDocument5 pagesAbdomen Pain Cause Nguyên Nhân Đau B NGto van quyenNo ratings yet
- Discharge Instructions For ColonosDocument1 pageDischarge Instructions For Colonosto van quyenNo ratings yet
- Discharge Instructions For Upper EndosDocument1 pageDischarge Instructions For Upper Endosto van quyenNo ratings yet
- ULCERATIVE COLITIS DISEASE BỆNH VIÊM LOÉT ĐẠI TRÀNGDocument2 pagesULCERATIVE COLITIS DISEASE BỆNH VIÊM LOÉT ĐẠI TRÀNGto van quyenNo ratings yet
- GASTROESOPHAGEAL REFLUX DISEASE INFORMATIONS - THÔNG TIN BỆNH TRÀO NGƯỢC DẠ DÀY THỰC QUẢNDocument4 pagesGASTROESOPHAGEAL REFLUX DISEASE INFORMATIONS - THÔNG TIN BỆNH TRÀO NGƯỢC DẠ DÀY THỰC QUẢNto van quyenNo ratings yet
- UPPER GI ENDOSCOPY INFORMATIONDocument5 pagesUPPER GI ENDOSCOPY INFORMATIONto van quyenNo ratings yet
- Helicobacter Pylori Treatment Summary and RecommendationsDocument2 pagesHelicobacter Pylori Treatment Summary and Recommendationsto van quyenNo ratings yet
- CROHN DISEASE BỆNH CROHNDocument5 pagesCROHN DISEASE BỆNH CROHNto van quyenNo ratings yet
- GASTRITIS DISEASE INFORMATIONS THÔNG TIN VỀ VIÊM DẠ DÀYDocument6 pagesGASTRITIS DISEASE INFORMATIONS THÔNG TIN VỀ VIÊM DẠ DÀYto van quyenNo ratings yet
- The Role of Endoscopy in The Management of Patientswith Peptic Ulcer DiseaseDocument6 pagesThe Role of Endoscopy in The Management of Patientswith Peptic Ulcer DiseaseLopez HenryNo ratings yet
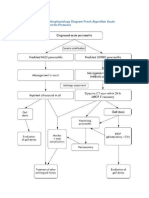
- Chronic Pancreatitis Pathophysiology Diagram Fresh Algorithm Acute Pancreatitis Management RN PinterestDocument2 pagesChronic Pancreatitis Pathophysiology Diagram Fresh Algorithm Acute Pancreatitis Management RN Pinterestto van quyenNo ratings yet
- Fibroadenoma of BreastDocument3 pagesFibroadenoma of BreastVirag PatilNo ratings yet
- Cisplatin's Molecular Mechanisms in Cancer TherapyDocument15 pagesCisplatin's Molecular Mechanisms in Cancer TherapyJuanita Pulido TeutaNo ratings yet
- Unit 1 The Integumentary SystemDocument3 pagesUnit 1 The Integumentary SystemSharva BhasinNo ratings yet
- Neoadjuvant ChemotherapyDocument8 pagesNeoadjuvant ChemotherapyrakaNo ratings yet
- Introduction Cancer BiologyDocument11 pagesIntroduction Cancer BiologySounak MandalNo ratings yet
- Gynecology - VaginalVulvar CancerDocument1 pageGynecology - VaginalVulvar CancerEugen MNo ratings yet
- Bfco193 Radiotherapy Dose Fractionation Third-edition-head-And-neck 0Document6 pagesBfco193 Radiotherapy Dose Fractionation Third-edition-head-And-neck 0Khumaira SantaNo ratings yet
- 2017 Growing Teratoma SyndromeDocument5 pages2017 Growing Teratoma SyndromeOscar GarciaNo ratings yet
- SperantaDocument12 pagesSperantaMonicaNo ratings yet
- Brain Tumors - KY Cancer RegistryDocument45 pagesBrain Tumors - KY Cancer RegistryMohammad Galih PratamaNo ratings yet
- Original ContributionDocument8 pagesOriginal ContributionĐô Lê PhiNo ratings yet
- Osteosarcoma Case StudyDocument17 pagesOsteosarcoma Case StudyleijustinesNo ratings yet
- Readers Digest Feb 2020 PDFDocument148 pagesReaders Digest Feb 2020 PDFMuralidharan KrishnamoorthyNo ratings yet
- Testicular Cancer JUDocument10 pagesTesticular Cancer JUkarla QuinteroNo ratings yet
- Breast Cancer TreatmentDocument13 pagesBreast Cancer TreatmentRissa AlmiraNo ratings yet
- DR Herry Setya Yudha Utama Spb. Finacs. Mhkes. Ics - Breast Cancer at AglanceDocument17 pagesDR Herry Setya Yudha Utama Spb. Finacs. Mhkes. Ics - Breast Cancer at AglanceKarina UtariNo ratings yet
- Breast - Dr. HammouriDocument12 pagesBreast - Dr. HammouriMohammad PropensityNo ratings yet
- Head and Neck OncologyDocument181 pagesHead and Neck OncologylanobregaaNo ratings yet
- secdocument_61Download Breast Pathology 2Nd Edition David J Dabbs full chapterDocument67 pagessecdocument_61Download Breast Pathology 2Nd Edition David J Dabbs full chapterjulia.swanson282100% (3)
- Does Neoadjuvant FOLFOX Chemotherapy Improve The Prognosis of High-RiskDocument13 pagesDoes Neoadjuvant FOLFOX Chemotherapy Improve The Prognosis of High-Riskellya zalfaNo ratings yet
- Bekaa Oncology - ProgramDocument7 pagesBekaa Oncology - ProgramhenrisaatjianNo ratings yet
- 10) One Word That Can Save Your LifeDocument4 pages10) One Word That Can Save Your LifeParesh PathakNo ratings yet
- Breast Cancer Early Detection and DiagnosisDocument55 pagesBreast Cancer Early Detection and Diagnosisbelva akbar medicalNo ratings yet
- Nove Farmakološke Strategije U Lečenju Nesitnoćelijskog Karcinoma PlućaDocument8 pagesNove Farmakološke Strategije U Lečenju Nesitnoćelijskog Karcinoma PlućaMomcilo Moca DjurovicNo ratings yet
- Teleoncology What Is It All About?: Prepared By-Shivika Bisen (09Bmd011) Ashita Paliwal (09Bmd006)Document14 pagesTeleoncology What Is It All About?: Prepared By-Shivika Bisen (09Bmd011) Ashita Paliwal (09Bmd006)sudarshan hackerNo ratings yet
- Breast Cancer Prevention: Saint Louis University School of Nursing Research JournalDocument3 pagesBreast Cancer Prevention: Saint Louis University School of Nursing Research JournalDale DeocaresNo ratings yet
- Temozolomide in Glioblastoma Multiforme: Dr. Djoko Widodo, DR., Spbs (K)Document19 pagesTemozolomide in Glioblastoma Multiforme: Dr. Djoko Widodo, DR., Spbs (K)Andre KristantoNo ratings yet
- Practice Bulletin: Management of Adnexal MassesDocument14 pagesPractice Bulletin: Management of Adnexal MassesDasha VeeNo ratings yet