You might also like
- Strategies To Prevent COVID 19 by GroupDocument3 pagesStrategies To Prevent COVID 19 by GroupJOY CELESTE SANCHEZNo ratings yet
- Nutrition NarrrativeDocument3 pagesNutrition NarrrativeKristine Mae C. DagatanNo ratings yet
- WAIVER With HeaderDocument4 pagesWAIVER With HeaderWILSON RIVERANo ratings yet
- Limited F2F Learning Contingency PlanDocument33 pagesLimited F2F Learning Contingency PlanDaniel MingoyNo ratings yet
- Immersion Letter To Mho and BarangaysDocument5 pagesImmersion Letter To Mho and BarangaysJules GajesNo ratings yet
- Class Monitoring Tool f2fDocument4 pagesClass Monitoring Tool f2fJoan Eve CabelloNo ratings yet
- School's Plan Integrating Minimum Health Standards in Light of Development of COVID 19 SituationsDocument1 pageSchool's Plan Integrating Minimum Health Standards in Light of Development of COVID 19 SituationsRobelyn Fababier VeranoNo ratings yet
- Kindergarten Narrative Report On SLM DistributionDocument4 pagesKindergarten Narrative Report On SLM DistributionCarlz Brian100% (2)
- Checklist V.O 2Document34 pagesChecklist V.O 2Patrick Zion TesalonaNo ratings yet
- Good MoralDocument8 pagesGood Moralhazel palabasanNo ratings yet
- Pangasinan State University: (NSTP 2 Instructor)Document2 pagesPangasinan State University: (NSTP 2 Instructor)Mary Cris LapitanNo ratings yet
- Certificate of Good Moral CharacterDocument24 pagesCertificate of Good Moral CharacterArchie UgbamenNo ratings yet
- DRRM Contingency Plan For Face To FaceDocument33 pagesDRRM Contingency Plan For Face To FaceEdward GolilaoNo ratings yet
- Limited Face To Face Contingency PlanDocument16 pagesLimited Face To Face Contingency PlanAriel PunzalanNo ratings yet
- Department of Education: Doris Dj. Estalilla, Ceso ViDocument1 pageDepartment of Education: Doris Dj. Estalilla, Ceso ViMhalou Jocson EchanoNo ratings yet
- Gwa CertificationDocument2 pagesGwa CertificationTintin ArcalasNo ratings yet
- Department of Education: Wash in Schools Programs (WINS)Document5 pagesDepartment of Education: Wash in Schools Programs (WINS)RONALYN ALVAREZNo ratings yet
- Edited 1 Curriculum VitaeDocument1 pageEdited 1 Curriculum Vitaerichie lapizNo ratings yet
- Good Moral CertificateDocument2 pagesGood Moral CertificateAnabel VillamorNo ratings yet
- Wins Narrative Reports1Document10 pagesWins Narrative Reports1Wenralf NagangdangNo ratings yet
- John Mark InauditoDocument2 pagesJohn Mark Inauditojoal.inaudito.uiNo ratings yet
- Pasilenges Contingency Plan For f2f Classess 2022Document38 pagesPasilenges Contingency Plan For f2f Classess 2022Angie Lea Serra-Ylarde100% (1)
- Department of Education: Republic of The PhilippinesDocument8 pagesDepartment of Education: Republic of The PhilippinesCarolina FornollesNo ratings yet
- Party ListDocument3 pagesParty ListVivian Artiaga TequilloNo ratings yet
- March-2024.Dengue NEW BUCAODocument1 pageMarch-2024.Dengue NEW BUCAOgladys pepitoNo ratings yet
- Final Research 1 3Document22 pagesFinal Research 1 3Xander LeeNo ratings yet
- Good MoralDocument3 pagesGood MoralMark Bryan CervantesNo ratings yet
- School-Memo-No-12-s-2022-CONDUCT OF EARLY REGISTRATION-SY-2022-2023Document3 pagesSchool-Memo-No-12-s-2022-CONDUCT OF EARLY REGISTRATION-SY-2022-2023Janice G. FelipeNo ratings yet
- GAD CertificatesDocument4 pagesGAD CertificatesCristilyn Saagundo100% (2)
- Abm 1 Meeting's Narrative ReportDocument4 pagesAbm 1 Meeting's Narrative Reportedilyn yansonNo ratings yet
- COVID 19 Monitoring ToolDocument6 pagesCOVID 19 Monitoring ToolAmelinda ManigosNo ratings yet
- Gulayan Sa TahananDocument7 pagesGulayan Sa TahananJohn Lerry IbuanNo ratings yet
- EPISODE 2 Narrative Report ARHDocument3 pagesEPISODE 2 Narrative Report ARHSHAIRUZ DUGAYNo ratings yet
- Contigency Plan For Lf2f Corrected 2Document10 pagesContigency Plan For Lf2f Corrected 2VICTORIANO B. INDAYA JRNo ratings yet
- MOA Failing GradesDocument4 pagesMOA Failing Gradesjecelyn mae Baluro100% (1)
- Good MoralDocument8 pagesGood MoralMary Grace LemonNo ratings yet
- Department of Education: Region Vii Schools Division of Negros Oriental Bulak Elementary School Dauin DistrictDocument4 pagesDepartment of Education: Region Vii Schools Division of Negros Oriental Bulak Elementary School Dauin DistrictannieNo ratings yet
- Q1 - Report On SARDO 1Document5 pagesQ1 - Report On SARDO 1Patrick Zion Tesalona0% (1)
- Annex G - Sample Health FormDocument1 pageAnnex G - Sample Health Formmary rose cornitoNo ratings yet
- Dalanguiring Is Monitoring Tool For School Opening Sy 2020 20211Document5 pagesDalanguiring Is Monitoring Tool For School Opening Sy 2020 20211armand resquir jrNo ratings yet
- Narrative Report On Module DistributionsDocument1 pageNarrative Report On Module DistributionsMargie RodriguezNo ratings yet
- Enrolment CampaignDocument2 pagesEnrolment Campaignnica pidlaoan100% (1)
- Letter For SBM Team DO Asking Technical AssistanceDocument2 pagesLetter For SBM Team DO Asking Technical AssistanceJohn Paul Dela PeñaNo ratings yet
- Letter To Sir PeterDocument1 pageLetter To Sir PeterNerwin IbarrientosNo ratings yet
- CONTINGENCY PLAN For Limited Face To FaceDocument15 pagesCONTINGENCY PLAN For Limited Face To FaceMaricar Dimas100% (3)
- Certification: Kidalos Elementary SchoolDocument2 pagesCertification: Kidalos Elementary SchoolADRIAN BUASANNo ratings yet
- Department of Education: Republic of The PhilippinesDocument22 pagesDepartment of Education: Republic of The PhilippinesSherwin DimaanoNo ratings yet
- Grade IV RBB Narrative Pictorial ReportDocument2 pagesGrade IV RBB Narrative Pictorial ReportJayr CaponponNo ratings yet
- Activity Bus - Math EditedDocument2 pagesActivity Bus - Math EditedCarlaNo ratings yet
- Letter Request For MedicineDocument2 pagesLetter Request For MedicinePrincess Joy Gavileño50% (2)
- Q1 ACR-DistributionDocument6 pagesQ1 ACR-DistributionCATHERINE MAGATNo ratings yet
- Immunization: Accomplishment ReportDocument2 pagesImmunization: Accomplishment ReportRachelle Annie TagamNo ratings yet
- Narrative Report - School DisinfectionDocument3 pagesNarrative Report - School DisinfectionBENES DOPITILLONo ratings yet
- Department of Education: I.Background/Introduction History of The SchoolDocument19 pagesDepartment of Education: I.Background/Introduction History of The SchoolSharme Cagalawan AmahanNo ratings yet
- To The Class Adviser: Check The Box To Indicate Your Assessment Guided by The Scale BelowDocument2 pagesTo The Class Adviser: Check The Box To Indicate Your Assessment Guided by The Scale BelowJesselly ValesNo ratings yet
- Republic of The Philippines Matalino St. D.M. Government Center, Maimpis, City of San Fernando (P)Document45 pagesRepublic of The Philippines Matalino St. D.M. Government Center, Maimpis, City of San Fernando (P)ShoeviceNo ratings yet
- Ssat Sgod DRRM Checklist Pagsangjan Es 159004Document45 pagesSsat Sgod DRRM Checklist Pagsangjan Es 159004ShoeviceNo ratings yet
- Learning Continuity Plan For The Limited Face To Face ClassesDocument41 pagesLearning Continuity Plan For The Limited Face To Face ClassesHaimen BuisanNo ratings yet
- Summary of Seminar Attended 2020-2021 - LACARDocument2 pagesSummary of Seminar Attended 2020-2021 - LACARCarlz BrianNo ratings yet
- Achieving Inclusive Education in the Caribbean and Beyond: From Philosophy to PraxisFrom EverandAchieving Inclusive Education in the Caribbean and Beyond: From Philosophy to PraxisStacey N. J. BlackmanNo ratings yet
- Class Summary of Pupils (DIORAMA)Document1 pageClass Summary of Pupils (DIORAMA)JOY CELESTE SANCHEZNo ratings yet
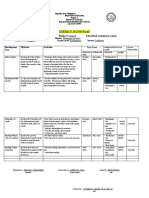
- Action PlanDocument4 pagesAction PlanJOY CELESTE SANCHEZNo ratings yet
- School ClearanceDocument1 pageSchool ClearanceJOY CELESTE SANCHEZNo ratings yet
- Narraive Report On Teachers Day 2022Document3 pagesNarraive Report On Teachers Day 2022JOY CELESTE SANCHEZNo ratings yet
- Accomplishment Report On 2021 Brigada Eskwela PlusDocument2 pagesAccomplishment Report On 2021 Brigada Eskwela PlusJOY CELESTE SANCHEZNo ratings yet
- Letter Informing of Distribution of SRCDocument1 pageLetter Informing of Distribution of SRCJOY CELESTE SANCHEZNo ratings yet
- Narrative Report of Distribution 2021Document2 pagesNarrative Report of Distribution 2021JOY CELESTE SANCHEZNo ratings yet
- Mechanics On LR Distribution & Retrieval of Self Learning ModulesDocument2 pagesMechanics On LR Distribution & Retrieval of Self Learning ModulesJOY CELESTE SANCHEZNo ratings yet
- MINUTES OF GENERAL PTA Meeting Held at Kindergarten ClassroomDocument4 pagesMINUTES OF GENERAL PTA Meeting Held at Kindergarten ClassroomJOY CELESTE SANCHEZNo ratings yet
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination Detailsdanial erham72No ratings yet
- Executive Order No. 015 Organizing BhertDocument2 pagesExecutive Order No. 015 Organizing Bhert잔돈100% (1)
- Covid-19 Communication ChartDocument1 pageCovid-19 Communication ChartSreekanth PCNo ratings yet
- Columbus Consolidated Government: Media ReleaseDocument3 pagesColumbus Consolidated Government: Media ReleaseDajhea JonesNo ratings yet
- Viernes 3 - 2° Dosis SputnikDocument48 pagesViernes 3 - 2° Dosis SputnikSilvio GuanucoNo ratings yet
- Jurnal KKN - Singgih Dwi Prasetyo UNSDocument11 pagesJurnal KKN - Singgih Dwi Prasetyo UNSSinggih Dwi PrasetyoNo ratings yet
- Self Declaration Form Details For International Arriving PassengersDocument2 pagesSelf Declaration Form Details For International Arriving Passengersmobile walaNo ratings yet
- JCI TT BidDocument9 pagesJCI TT BidJanis Medina ReginioNo ratings yet
- California Department of Corrections EmailDocument3 pagesCalifornia Department of Corrections EmailHeidi McCaffertyNo ratings yet
- Scrapbook in EAPPDocument8 pagesScrapbook in EAPPFercylaine EsponillaNo ratings yet
- CertificateDocument1 pageCertificatechinni kumarNo ratings yet
- Dec. 13, 2021 Letter of Instruction To Peterborough WorkplacesDocument4 pagesDec. 13, 2021 Letter of Instruction To Peterborough WorkplacesPeterborough ExaminerNo ratings yet
- Updated Signs and Symptoms Monitoring Sheet For COVID 19Document1 pageUpdated Signs and Symptoms Monitoring Sheet For COVID 19Marlon AbellanaNo ratings yet
- Timoteo Paez Integrated School (SHS) : Research PlanDocument9 pagesTimoteo Paez Integrated School (SHS) : Research PlanEzekiel AvisoNo ratings yet
- Bill Little, CPRMC CEO, Letter To The CommunityDocument1 pageBill Little, CPRMC CEO, Letter To The CommunityWMBF NewsNo ratings yet
- NHS COVID Pass - Vaccinated: 2D Barcode e Xpiry Sye D Abbas Ple Ase Che CK Against The Be Are R's Ide NtityDocument2 pagesNHS COVID Pass - Vaccinated: 2D Barcode e Xpiry Sye D Abbas Ple Ase Che CK Against The Be Are R's Ide NtityAli Abbas LeicesterNo ratings yet
- History Holiday Homework FinalDocument14 pagesHistory Holiday Homework FinalKavin UpretiNo ratings yet
- Mozart Andante in C MajorDocument7 pagesMozart Andante in C Majorparia dNo ratings yet
- IP Project Covid-19 ImpactDocument24 pagesIP Project Covid-19 ImpactLawanya VermaNo ratings yet
- CTA Mandate Policy (11/01 Deadline)Document5 pagesCTA Mandate Policy (11/01 Deadline)Chicago Transit Justice CoalitionNo ratings yet
- EZMSA COVID AnnouncementDocument2 pagesEZMSA COVID AnnouncementEmily Mertz100% (1)
- Covid 19: No Contract Thermal Scanning, No-Mask, No Entry PlociyDocument2 pagesCovid 19: No Contract Thermal Scanning, No-Mask, No Entry PlociyJanine Binbing0% (1)
- 2020 KOICA Scholarship Program Fellows Guidelines For Entry To KoreaDocument2 pages2020 KOICA Scholarship Program Fellows Guidelines For Entry To KoreaTikoto BackupNo ratings yet
- Self Declaration Form Details For International Arriving PassengersDocument2 pagesSelf Declaration Form Details For International Arriving PassengersRakesh SinghNo ratings yet
- Richland County School District 1 COVID ProtocolsDocument1 pageRichland County School District 1 COVID ProtocolsWLTXNo ratings yet
- 2020 Contracts With Negative SlippageDocument105 pages2020 Contracts With Negative SlippageJasper Kenneth PeraltaNo ratings yet
- Guidelines For Deploying Student NursesDocument2 pagesGuidelines For Deploying Student NursesDivya ToppoNo ratings yet
- TranzacțieDocument2 pagesTranzacțieAlexandra TanaseNo ratings yet
- Covid-19 Expose (Unmask)Document2 pagesCovid-19 Expose (Unmask)Eduardo CasesNo ratings yet
- Sabarimala: Virtual-Q Booking CouponDocument2 pagesSabarimala: Virtual-Q Booking CouponST COMMNICATIONNo ratings yet