You might also like
- Food Exchange List by PNS.Document46 pagesFood Exchange List by PNS.Muhammad ShaffiNo ratings yet
- BiPAP Full FlowchartDocument1 pageBiPAP Full FlowchartArjun KumarNo ratings yet
- PUB 540 Topic 4 Calculating Ratio OddsDocument6 pagesPUB 540 Topic 4 Calculating Ratio OddsKevin Nyasogo100% (1)
- Overcoming Stress-Induced Brain Fog 10 Simple Ways To Find Focus Improve Memory and Feel Grounded Jill WeberDocument194 pagesOvercoming Stress-Induced Brain Fog 10 Simple Ways To Find Focus Improve Memory and Feel Grounded Jill WeberTyler Vint100% (1)
- Seafastening ExcelDocument13 pagesSeafastening ExcelRiyan EsapermanaNo ratings yet
- Coagulation DrugsDocument1 pageCoagulation Drugsmed testNo ratings yet
- Program Graduate Competency ReflectionDocument11 pagesProgram Graduate Competency Reflectionapi-458433381No ratings yet
- CKD Algorithm Final - 2011 - May 18Document1 pageCKD Algorithm Final - 2011 - May 18AnjaniNo ratings yet
- Hyperkalemia Metabolic Acidosis Hyperuricemia: Xanthine Oxidase InhibitorsDocument1 pageHyperkalemia Metabolic Acidosis Hyperuricemia: Xanthine Oxidase InhibitorsTyler VintNo ratings yet
- Rational Use of Single Pill CombinationDocument19 pagesRational Use of Single Pill CombinationStella CooKeyNo ratings yet
- ATOMAC Guideline v11.0 PDFDocument1 pageATOMAC Guideline v11.0 PDFFernando GarciaNo ratings yet
- 080630 고혈압최신지견 (조장현 과장님)Document46 pages080630 고혈압최신지견 (조장현 과장님)hongmyongNo ratings yet
- 5Th FloorDocument8 pages5Th FloorGerald AndersonNo ratings yet
- Critical Care Drug Reference SheetDocument12 pagesCritical Care Drug Reference SheetYanina CoxNo ratings yet
- QR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Document1 pageQR ANTIBIOTIC GUIDELINE A3 Size - 210628 - 082213 - 210628 - 082342 - 210628 - 082357-1Munirah YusoffNo ratings yet
- Anti CoagulationDocument2 pagesAnti Coagulationsundance127No ratings yet
- Intravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury HospitalDocument39 pagesIntravenous Infusion Orders For Common Medications in The ED and ICU - Bunbury Hospital9wb646hq7mNo ratings yet
- Medications Doc XDocument4 pagesMedications Doc Xezinne obinna-umaNo ratings yet
- NebivololDocument2 pagesNebivololSophia MarieNo ratings yet
- RahpoDocument3 pagesRahpoassouma16052002No ratings yet
- Course in The Ward: Date and Time Focus Doctor's Order Nurses Note August 28, 2018 3:50PM Vital Signs: AdmissionDocument4 pagesCourse in The Ward: Date and Time Focus Doctor's Order Nurses Note August 28, 2018 3:50PM Vital Signs: AdmissionMartin T ManuelNo ratings yet
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNo ratings yet
- 22 Jaga EDP-AGS 13-7-15Document12 pages22 Jaga EDP-AGS 13-7-15eka dharmaNo ratings yet
- DUNGOG - Gestational Hypertension Drug StudyDocument2 pagesDUNGOG - Gestational Hypertension Drug Studytophergonzales45No ratings yet
- Drug SummariesDocument10 pagesDrug SummariesSlavi StanimirovNo ratings yet
- Acute Heart FailureDocument1 pageAcute Heart FailureJuan HarshaNo ratings yet
- Doctor's Order Sample 1 IMDocument2 pagesDoctor's Order Sample 1 IMfujoji92No ratings yet
- Yes No: Propranolol AtenololDocument1 pageYes No: Propranolol AtenololLuthfi IndiwirawanNo ratings yet
- Beta BlockertreatmentalgorithmDocument1 pageBeta BlockertreatmentalgorithmLind YLNo ratings yet
- Hypertension ProtocolDocument1 pageHypertension ProtocolkalyanigomathinayagamNo ratings yet
- PocketCard UPDATE2013 EnglishDocument2 pagesPocketCard UPDATE2013 EnglishTowhidulIslamNo ratings yet
- Ninja - Anti-HTN PDFDocument6 pagesNinja - Anti-HTN PDFErica Hyeyeon Lee100% (2)
- Generic/ Brand Name Humulin RDocument7 pagesGeneric/ Brand Name Humulin Rshujin_sama100% (2)
- Trauma Male A: General Surgery: Team I Dr. Tamani/Lingan/Aguisanda/Baculi/Casco/ BulusanDocument7 pagesTrauma Male A: General Surgery: Team I Dr. Tamani/Lingan/Aguisanda/Baculi/Casco/ BulusanLuis PadillaNo ratings yet
- Ppi1637a01 CK MB TabletsDocument2 pagesPpi1637a01 CK MB TabletsNehul PatilNo ratings yet
- Map DkaDocument1 pageMap DkaSH PrageethNo ratings yet
- COVID 19 Anticoagulation Algorithm Version Final 1.1Document2 pagesCOVID 19 Anticoagulation Algorithm Version Final 1.1Emi PuspitasariNo ratings yet
- CEG Formulary: Cardiac Medications For Dogs: ... Bringing Cardiology Into PracticeDocument6 pagesCEG Formulary: Cardiac Medications For Dogs: ... Bringing Cardiology Into PracticeAngeles MerinoNo ratings yet
- Table 48A-1R - Second Line Antiepileptic Drug Dosing and SerumDocument1 pageTable 48A-1R - Second Line Antiepileptic Drug Dosing and SerumDragutin PetrićNo ratings yet
- Mono Dual Triple Therapy DiabetesDocument1 pageMono Dual Triple Therapy DiabetesbharatNo ratings yet
- JNC8 HTNGuidelines Book BookletDocument2 pagesJNC8 HTNGuidelines Book BookletDestya SNNo ratings yet
- Hypertension Mind MapDocument1 pageHypertension Mind MapBrett DaleNo ratings yet
- AMPRAHAN UNIT INFEKSI RSUP HAM Minggu Pagi, 26 November 2023Document9 pagesAMPRAHAN UNIT INFEKSI RSUP HAM Minggu Pagi, 26 November 2023alfaz zamzamiNo ratings yet
- Respiratory DrugsDocument2 pagesRespiratory Drugsmed testNo ratings yet
- Pharmacology (Must Know)Document88 pagesPharmacology (Must Know)Wahib ZaidiNo ratings yet
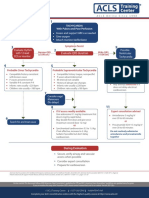
- ACLS ChartDocument1 pageACLS ChartJev DespiNo ratings yet
- 2020 ESC Guidelines For The Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-segment (22-24)Document3 pages2020 ESC Guidelines For The Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-segment (22-24)Sheila Setiawati TanzilNo ratings yet
- PharmacologyDocument21 pagesPharmacologySophia Kyla AcerNo ratings yet
- Rawabi Saleh Bakrman Fatima Mohammed Dawood Supervision: Dr. Hassan BayashootDocument21 pagesRawabi Saleh Bakrman Fatima Mohammed Dawood Supervision: Dr. Hassan BayashootRawabi SalehNo ratings yet
- Carta AntibiotikDocument1 pageCarta AntibiotikShazwani KKTSNo ratings yet
- PharmacologyDocument8 pagesPharmacologynazbeen.ahmadiNo ratings yet
- HAPTODocument4 pagesHAPTOLaboratorios HerliNo ratings yet
- Clinical Asthma Pathway: ED Phase 1a: Initial Assessment - 1st HourDocument2 pagesClinical Asthma Pathway: ED Phase 1a: Initial Assessment - 1st Hourd'Agung NugrohoNo ratings yet
- Drug List: Medication Adult Dosing Pediatric DosingDocument14 pagesDrug List: Medication Adult Dosing Pediatric DosingAndrew JamesNo ratings yet
- KEM Protocols - Hypertensive Emergency (Dr. Pritha)Document3 pagesKEM Protocols - Hypertensive Emergency (Dr. Pritha)Sonu AntonyNo ratings yet
- Barbiturates Drug SummaryDocument5 pagesBarbiturates Drug SummarySydney JenningsNo ratings yet
- Algo Pals TachycardiaDocument1 pageAlgo Pals TachycardiaArdie FratamaNo ratings yet
- Atrial Fibrillation - Student ResidencyDocument6 pagesAtrial Fibrillation - Student Residencyapi-404356063No ratings yet
- Day - 2 - Date - Se P T e Mber 2 6, 2 0 2 0 Area - Shift - 7 A M - 3 P M Clinical Instructor: S I R Roy L I N AoDocument4 pagesDay - 2 - Date - Se P T e Mber 2 6, 2 0 2 0 Area - Shift - 7 A M - 3 P M Clinical Instructor: S I R Roy L I N AorlinaoNo ratings yet
- Apo B 2013Document2 pagesApo B 2013susey tepaNo ratings yet
- Mdbsis04 Bili T-Dmso 2017Document4 pagesMdbsis04 Bili T-Dmso 2017dr_joe23No ratings yet
- Blood ComponentsDocument5 pagesBlood ComponentsoxalateNo ratings yet
- Cardio Oncology TableDocument5 pagesCardio Oncology TableCyNo ratings yet
- Drugs Reconst. Dilution Stability After Reconst. Dose Adjustment Infusion Rate NotesDocument13 pagesDrugs Reconst. Dilution Stability After Reconst. Dose Adjustment Infusion Rate NotesRania ElwatidyNo ratings yet
- HD ComplicationsDocument1 pageHD ComplicationsTyler VintNo ratings yet
- Uhh I AgreeDocument3 pagesUhh I AgreeTyler VintNo ratings yet
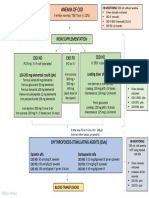
- Anemia of CKD: Iron SupplementationDocument1 pageAnemia of CKD: Iron SupplementationTyler VintNo ratings yet
- Copper IUD: Wilson's Disease LNG-IUD: Progestin-DependentDocument2 pagesCopper IUD: Wilson's Disease LNG-IUD: Progestin-DependentTyler VintNo ratings yet
- Lecture 10Document1 pageLecture 10Tyler VintNo ratings yet
- CKD-MBD Targets:: ParathyroidectomyDocument1 pageCKD-MBD Targets:: ParathyroidectomyTyler VintNo ratings yet
- Uno and We WatchDocument4 pagesUno and We WatchTyler VintNo ratings yet
- DeadDocument1 pageDeadTyler VintNo ratings yet
- U1 Lesson PlanDocument8 pagesU1 Lesson PlanTyler VintNo ratings yet
- U1 PowerpointDocument23 pagesU1 PowerpointTyler VintNo ratings yet
- Compilation of Reviewer For Fundamentals of Nursing PDF FreeDocument49 pagesCompilation of Reviewer For Fundamentals of Nursing PDF FreeTyler VintNo ratings yet
- Organ SystemDocument20 pagesOrgan SystemTyler Vint100% (1)
- Sneakers As A First Step in Chemical Engineering Author Margot Vigeant, Richard MooreDocument12 pagesSneakers As A First Step in Chemical Engineering Author Margot Vigeant, Richard MooreTyler VintNo ratings yet
- Dental Education in The PhilippinesDocument4 pagesDental Education in The PhilippinesTyler VintNo ratings yet
- OSS SSGU Entry On Scholarships Evidencev5Document2 pagesOSS SSGU Entry On Scholarships Evidencev5Tyler VintNo ratings yet
- Curriculum Doctor of Dental MedicineDocument3 pagesCurriculum Doctor of Dental MedicineTyler VintNo ratings yet
- Chemical Engineering Thermodynamics Transforming Thermo Lectures Into A Dynamic Experience (Article) Author Rebecca K. ToghianiDocument6 pagesChemical Engineering Thermodynamics Transforming Thermo Lectures Into A Dynamic Experience (Article) Author Rebecca K. ToghianiTyler VintNo ratings yet
- Chemical Engineering Matters For A Modern World Author Raffaella OconeDocument24 pagesChemical Engineering Matters For A Modern World Author Raffaella OconeTyler VintNo ratings yet
- Collecting DataDocument6 pagesCollecting DataTyler VintNo ratings yet
- Presentation of DataDocument18 pagesPresentation of DataTyler VintNo ratings yet
- 2019 2020-HandbookSUBMITTEDDocument41 pages2019 2020-HandbookSUBMITTEDTyler VintNo ratings yet
- Registered Dietitian Role DescriptionDocument2 pagesRegistered Dietitian Role DescriptionTyler VintNo ratings yet
- 1 Summative Test (1 Quarter) IN PE 11 (HE, SMAW, STEM-A & B, and ABM)Document3 pages1 Summative Test (1 Quarter) IN PE 11 (HE, SMAW, STEM-A & B, and ABM)Tyler VintNo ratings yet
- Done Hope1 q1 Mod4 Skill Related FitnessDocument25 pagesDone Hope1 q1 Mod4 Skill Related FitnessTyler VintNo ratings yet
- JEY ANN CANDAME UNDERSTANDING THE SELF Module 7Document8 pagesJEY ANN CANDAME UNDERSTANDING THE SELF Module 7ren alvaradoNo ratings yet
- McDonal Data Analysis PDFDocument16 pagesMcDonal Data Analysis PDFAnandha SayanamNo ratings yet
- 2nd Quarter-Module2-Personal Development 11Document6 pages2nd Quarter-Module2-Personal Development 11TJ ArgunaNo ratings yet
- Jharkhand ReportDocument133 pagesJharkhand ReportNutan TiggaNo ratings yet
- Brochure BOP PODDocument4 pagesBrochure BOP PODtkthird siaminterNo ratings yet
- Appendicitis Case StudyDocument35 pagesAppendicitis Case StudyWilliam Soneja CalapiniNo ratings yet
- Anal Sex Basics (Carlyle Jansen)Document222 pagesAnal Sex Basics (Carlyle Jansen)huora100% (2)
- OPD Group Insurance PolicyDocument26 pagesOPD Group Insurance PolicyRakshith RaghuNo ratings yet
- Presentation, Analysis and Interpretation of DataDocument11 pagesPresentation, Analysis and Interpretation of DataDjameica GuerreroNo ratings yet
- Getaizenpower24 Com Start Index PHPDocument5 pagesGetaizenpower24 Com Start Index PHPmyousaf2121No ratings yet
- How To Remove Gallstones NaturallyDocument11 pagesHow To Remove Gallstones NaturallyRichard Bersola Estonilo100% (4)
- Dissociative Identity Disorder PDFDocument8 pagesDissociative Identity Disorder PDFapek leeNo ratings yet
- Heat Stress NotesDocument38 pagesHeat Stress Notesnurjamima96No ratings yet
- Kyla Mae UlatDocument6 pagesKyla Mae UlatKyla UlatNo ratings yet
- Impact of Social Media On Youth Comprehensive AnalysisDocument17 pagesImpact of Social Media On Youth Comprehensive AnalysisSenthil RajuNo ratings yet
- Health, Safety & Environment Standard Products CatalogDocument87 pagesHealth, Safety & Environment Standard Products Catalogvikrant911No ratings yet
- Unit 6: Q2e Listening & Speaking 3: Audio ScriptDocument8 pagesUnit 6: Q2e Listening & Speaking 3: Audio ScriptQuỳnh LươngNo ratings yet
- Nutrients 14 00427 v3Document14 pagesNutrients 14 00427 v3Edson HilárioNo ratings yet
- ECS HFC-227ea - Owner's Manual - February 2001-06-236118-001 - Rev - AADocument36 pagesECS HFC-227ea - Owner's Manual - February 2001-06-236118-001 - Rev - AAgilangolandiaNo ratings yet
- Public HealthDocument8 pagesPublic HealthThess Cahigas - NavaltaNo ratings yet
- Understanding The Codex AlimentariusDocument28 pagesUnderstanding The Codex AlimentariusIsobelNo ratings yet
- COVID-19: The Moral Obligation of Nurse LeadersDocument3 pagesCOVID-19: The Moral Obligation of Nurse Leaderszaenal abidinNo ratings yet
- TIMOTHYDocument3 pagesTIMOTHYShan ElahiNo ratings yet
- La ConsolacionDocument2 pagesLa ConsolacionRex RegioNo ratings yet
- Radiographic Special Procedures: Kenneth M. Luciano, RRTDocument36 pagesRadiographic Special Procedures: Kenneth M. Luciano, RRTKaye A. JardinicoNo ratings yet
- 40726-Article Text-143632-1-10-20190330 PDFDocument10 pages40726-Article Text-143632-1-10-20190330 PDFAshik Das 172-34-653No ratings yet