You might also like
- Herpes Simplex Varicella and Zoster: Clinical Manifestations and TreatmentFrom EverandHerpes Simplex Varicella and Zoster: Clinical Manifestations and TreatmentRating: 5 out of 5 stars5/5 (19)
- MeningitisDocument3 pagesMeningitisSuhana JahangeerNo ratings yet
- Non-Sporing Anaerobic: InfectionsDocument14 pagesNon-Sporing Anaerobic: InfectionsZeth MoturiNo ratings yet
- VESICULOBULLOUS DISEASE by AMDocument4 pagesVESICULOBULLOUS DISEASE by AMbasitcontentNo ratings yet
- AAD-BF-Cutaneous-Manifestations-of-HIV-InfectionsDocument2 pagesAAD-BF-Cutaneous-Manifestations-of-HIV-Infectionskahkashanahmed065No ratings yet
- 2.congenital TORCH InfDocument24 pages2.congenital TORCH Infelka.kgmaNo ratings yet
- Diseases of Poultry: Identification and PathologyDocument23 pagesDiseases of Poultry: Identification and PathologyFlaviu TabaranNo ratings yet
- DNA and RNA VirusesDocument6 pagesDNA and RNA VirusesjeffdelacruzNo ratings yet
- Health ManagementDocument6 pagesHealth ManagementDave DimayugaNo ratings yet
- Microbiolog - VirologyDocument16 pagesMicrobiolog - Virologytdci.franceskorineganzaNo ratings yet
- Derma Transcribed Table FormDocument9 pagesDerma Transcribed Table FormGerlyn MarcelinoNo ratings yet
- Pedia Resident's CompetencyDocument12 pagesPedia Resident's CompetencyElizabeth MaderazoNo ratings yet
- Normal Body FloraDocument1 pageNormal Body FloraJulia IshakNo ratings yet
- Dermatology Condition Description Signs/symptoms DDX Viral InfectionsDocument40 pagesDermatology Condition Description Signs/symptoms DDX Viral InfectionsWaseem Ullah100% (1)
- White LesionsDocument25 pagesWhite LesionsKyla JoelleNo ratings yet
- Infection 2021Document32 pagesInfection 2021noor.albseerawiNo ratings yet
- Tonsilitis + Scarlet + MeningitisDocument3 pagesTonsilitis + Scarlet + Meningitisd3mooz13No ratings yet
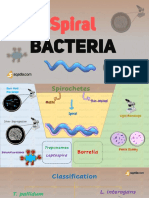
- Spiral: BacteriaDocument28 pagesSpiral: BacteriaZeth MoturiNo ratings yet
- Dna PDFDocument1 pageDna PDFAhmed SobhNo ratings yet
- MB Yeasts PassDocument1 pageMB Yeasts PassJulia IshakNo ratings yet
- Cerebellum ORR Derma ImagesDocument25 pagesCerebellum ORR Derma Imagessubramaniam krishnamoorthiNo ratings yet
- Bullous Pemphigoid Vs Epydermolysis Bullosa Acquisita: Diagnosis and How To DifferentiateDocument12 pagesBullous Pemphigoid Vs Epydermolysis Bullosa Acquisita: Diagnosis and How To DifferentiateIrene Irene100% (1)
- Herpes Simplex Virus: 2 SerotypesDocument18 pagesHerpes Simplex Virus: 2 Serotypespedia blue bookNo ratings yet
- Herpes Simplex Virus Types, Sites, Lesions and TreatmentsDocument1 pageHerpes Simplex Virus Types, Sites, Lesions and Treatmentsmkct111No ratings yet
- BULLOUS DISORDER (4th Yr)Document45 pagesBULLOUS DISORDER (4th Yr)Yahya IftekharNo ratings yet
- Aids, Hiv, CancerDocument38 pagesAids, Hiv, CancerJianni ClaridadNo ratings yet
- Fever With RashDocument2 pagesFever With RashzahraaNo ratings yet
- Bovine Viral Diarrhoea: BVD Is A Sub Acute, Acute or INAPPARENT Contagious Disease Characterized byDocument27 pagesBovine Viral Diarrhoea: BVD Is A Sub Acute, Acute or INAPPARENT Contagious Disease Characterized byhari krishnaa athotaNo ratings yet
- Ves Icu Bull OusDocument59 pagesVes Icu Bull Ousv sreedharNo ratings yet
- The Newborn at Risk of A Maternal Infection Opthalmia NeonatorumDocument2 pagesThe Newborn at Risk of A Maternal Infection Opthalmia NeonatorumIren Rose PañaNo ratings yet
- Oral Manifestation of HivDocument1 pageOral Manifestation of HivDurva JainNo ratings yet
- DiagnosticDocument21 pagesDiagnosticFRI CHIKSNo ratings yet
- Impetigo, Erysipela S, Cellulitis: Rasay, Joana Mikee DDocument48 pagesImpetigo, Erysipela S, Cellulitis: Rasay, Joana Mikee DJoana Mikee RasayNo ratings yet
- Herpes Simplex - PathophysiologyDocument1 pageHerpes Simplex - PathophysiologyRainny CommsNo ratings yet
- Nematodes Common Name Characteristic S Host Disease Produced Diagnosis MOT Location EggsDocument8 pagesNematodes Common Name Characteristic S Host Disease Produced Diagnosis MOT Location EggsGumimba, Ma. Mae JoyceNo ratings yet
- Cims Case 1 - SGD A4Document16 pagesCims Case 1 - SGD A4SGD A4No ratings yet
- Concept MapDocument2 pagesConcept MapRAYAMAE LUMOGDANGNo ratings yet
- Female Genital Tract Infections and PathologyDocument16 pagesFemale Genital Tract Infections and Pathologymiguel cuevasNo ratings yet
- Intraepidermal Autoimmune Bullous Dermatoses: Principles of DiagnosisDocument31 pagesIntraepidermal Autoimmune Bullous Dermatoses: Principles of DiagnosisCiubuc AndrianNo ratings yet
- 2010 First Aid Microbiology HIV-positive Adult NeoplasmsDocument1 page2010 First Aid Microbiology HIV-positive Adult NeoplasmsGabriel F. SotoNo ratings yet
- Pediatrics: Compilation of Tables From Topnotch Pedia HandoutDocument6 pagesPediatrics: Compilation of Tables From Topnotch Pedia HandoutCielo Lomibao0% (1)
- CNS Infection, ReviewsDocument17 pagesCNS Infection, ReviewsAbdulelah MurshidNo ratings yet
- Iva Kak PettyDocument43 pagesIva Kak PettyNita VilinNo ratings yet
- Rach15 - Infection Control and Asepsis NuDocument1 pageRach15 - Infection Control and Asepsis NuFalqueza JanelleNo ratings yet
- Microbio Report (Dellava and Mamae)Document3 pagesMicrobio Report (Dellava and Mamae)JamesBuensalidoDellavaNo ratings yet
- Dermatology PDFDocument57 pagesDermatology PDFSheikhEras100% (1)
- EedDocument70 pagesEedzihniyya471No ratings yet
- Haemophilus Bacteria Identification GuideDocument11 pagesHaemophilus Bacteria Identification GuideADINo ratings yet
- Staph. Aureus Staph. Epidermidis Staph. SaprophyticusDocument5 pagesStaph. Aureus Staph. Epidermidis Staph. SaprophyticusTom PedersonNo ratings yet
- 07-08 Fmui Student DotsDocument59 pages07-08 Fmui Student Dotsdiklat pkckramatjatiNo ratings yet
- Diseases of Lab AnimalsDocument45 pagesDiseases of Lab AnimalsvetpathforumNo ratings yet
- Laboratory Diagnosis of Eye Infection: WinartoDocument56 pagesLaboratory Diagnosis of Eye Infection: WinartoozierefNo ratings yet
- Approach Bullous Disorders PatientDocument50 pagesApproach Bullous Disorders PatientAbhirut ThakurNo ratings yet
- Diseases of External Ear MindmapDocument1 pageDiseases of External Ear MindmapLu YaNo ratings yet
- Presentation 1Document15 pagesPresentation 1vampirehulkNo ratings yet
- On Demand Pediatric SkullDocument20 pagesOn Demand Pediatric SkullMalekseuofi مالك السيوفيNo ratings yet
- Infections of the Skin and MeningesDocument10 pagesInfections of the Skin and MeningesNoelani-Mei AscioNo ratings yet
- Bacterial meningitis CSF analysisDocument3 pagesBacterial meningitis CSF analysisBang QuachNo ratings yet
- 12-07 TB ImmunopathogenesisDocument44 pages12-07 TB ImmunopathogenesisrizaparamithaNo ratings yet
- Day 1 - 01. LY - EBV Biology in Nasopharyngeal CancerDocument5 pagesDay 1 - 01. LY - EBV Biology in Nasopharyngeal CancerHari PranotoNo ratings yet
- AmendmentsDocument1 pageAmendmentsJaime GaviolaNo ratings yet
- Postpartum Care and Breastfeeding GuidanceDocument2 pagesPostpartum Care and Breastfeeding GuidanceArjay EllaNo ratings yet
- Nepal 3 Year Interim Plan EngDocument42 pagesNepal 3 Year Interim Plan Engparbatdhungana100% (1)
- Mental: Your Health MattersDocument2 pagesMental: Your Health MattersKrsnaPentayahNo ratings yet
- Community-Based Approach For Dengue Prevention and Control in Sta. Cruz, Laguna, PhilippinesDocument7 pagesCommunity-Based Approach For Dengue Prevention and Control in Sta. Cruz, Laguna, PhilippinesBella LifindraNo ratings yet
- Safety, Health and Environment Manual and ProceduresDocument20 pagesSafety, Health and Environment Manual and ProceduresYan's Senora BescoroNo ratings yet
- Virtual Simulation Learning among Student Nurses in PACUDocument4 pagesVirtual Simulation Learning among Student Nurses in PACUJessa BorreNo ratings yet
- Health Services ManagementDocument6 pagesHealth Services ManagementWanyonyi JustusNo ratings yet
- Assessment Report Cinnamomum VerumDocument22 pagesAssessment Report Cinnamomum VerumAlejandra Rodriguez SolanoNo ratings yet
- Uncope Sa BJ DW 170819 PDFDocument2 pagesUncope Sa BJ DW 170819 PDFanon_717360607No ratings yet
- Quadas 2Document10 pagesQuadas 2Lya QillahNo ratings yet
- Enteral Tube Administration of Oral Chemotherapy DrugsDocument15 pagesEnteral Tube Administration of Oral Chemotherapy DrugsCoté HuertaNo ratings yet
- HTM 01 01 PartADocument59 pagesHTM 01 01 PartAwaseem kausarNo ratings yet
- CPE5601 Diagnosis and Treatment of Feeding and Eating DisordersDocument16 pagesCPE5601 Diagnosis and Treatment of Feeding and Eating DisordersSiti MuslihaNo ratings yet
- Roger A. Mackinnon, Robert Michels, Peter J. Buckley-The Psychiatric Interview in Clinical Practice (2015)Document724 pagesRoger A. Mackinnon, Robert Michels, Peter J. Buckley-The Psychiatric Interview in Clinical Practice (2015)Selma Churukova92% (12)
- Culture Level On Patient Safety in Nursing StaffDocument13 pagesCulture Level On Patient Safety in Nursing StaffInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NCP 5 Ovarian CancerDocument6 pagesNCP 5 Ovarian Cancersaint_ronald886% (29)
- Precision Medicine in Cancers and Non-Communicable DiseasesDocument343 pagesPrecision Medicine in Cancers and Non-Communicable DiseasesBenaia João NHAMITAMBONo ratings yet
- How staying up late affects your sleep and healthDocument16 pagesHow staying up late affects your sleep and healthHelder BalantaNo ratings yet
- 5 Horrifying Facts About FDA-Vaccine-Approval-Process-2019Document24 pages5 Horrifying Facts About FDA-Vaccine-Approval-Process-2019Pollyana Furtado JunqueiraNo ratings yet
- Adivasi Journal Vol-45Document97 pagesAdivasi Journal Vol-45hndashNo ratings yet
- Cases in Human Parasitology: AcknowledgmentsDocument2 pagesCases in Human Parasitology: AcknowledgmentsAngelo GreenNo ratings yet
- NCP KateDor NewDocument6 pagesNCP KateDor NewSteffi GolezNo ratings yet
- Pharma Sales Crediting Incentives For Accurate and Compliant Processes Codex3444Document11 pagesPharma Sales Crediting Incentives For Accurate and Compliant Processes Codex3444pranali100% (2)
- Jac420-Musical Influence OnDocument3 pagesJac420-Musical Influence Onapi-238822444No ratings yet
- Domperidone For Increasing Breast Milk Supply 260219 PDFDocument2 pagesDomperidone For Increasing Breast Milk Supply 260219 PDFANneNo ratings yet
- Mamusha PDFDocument72 pagesMamusha PDFFikadu WendmtayeNo ratings yet
- Ambassador EveningDocument11 pagesAmbassador Eveningakshayapril24No ratings yet
- Dysfunctional Uterine Bleeding History CollectionDocument4 pagesDysfunctional Uterine Bleeding History CollectionAnitha BalakrishnanNo ratings yet
- Makabuhay (Tinospora RumphiiDocument4 pagesMakabuhay (Tinospora RumphiiErica Ritz TrainNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)