You might also like
- Ao 2021-0056-ADocument2 pagesAo 2021-0056-AHarold Paulo Mejia100% (1)
- DC No. 2022-0382 - FY 2022 2Q LHS ML Progress Monitoring ReportDocument19 pagesDC No. 2022-0382 - FY 2022 2Q LHS ML Progress Monitoring ReportHarold Paulo Mejia100% (1)
- GTA 03-08-002 Contaminated Casualty CareDocument2 pagesGTA 03-08-002 Contaminated Casualty Carerickoshea160No ratings yet
- KRA-2 1 6 B - RHADocument3 pagesKRA-2 1 6 B - RHAJustine Grace TolentinoNo ratings yet
- Form 3 HEARS Field Report 1Document1 pageForm 3 HEARS Field Report 1Meme LangNo ratings yet
- Rha Municipal Consolidation'Document3 pagesRha Municipal Consolidation'D Alfz EinsTein JDNo ratings yet
- (Oct. 2016) Braindump2go AWS Certified Solutions Architect Associate Exam Dumps 423q (1 20)Document2 pages(Oct. 2016) Braindump2go AWS Certified Solutions Architect Associate Exam Dumps 423q (1 20)Swayampu Sree AnirudhNo ratings yet
- Death Certificate Amended FormDocument1 pageDeath Certificate Amended FormMohammad FamuNo ratings yet
- Disaster ManagementDocument3 pagesDisaster ManagementAarti DivyaNo ratings yet
- Result Report Print1Document10 pagesResult Report Print1GeoVakNo ratings yet
- WAH & Confined Space Rescue Plan Formats 1Document2 pagesWAH & Confined Space Rescue Plan Formats 1soumyajeet NayakNo ratings yet
- 3559 JordanNPPresentationDocument15 pages3559 JordanNPPresentationMahendra KakdeNo ratings yet
- RiskAssessment For Precast Foundation and Road MarkingDocument13 pagesRiskAssessment For Precast Foundation and Road MarkingAneessh KumarNo ratings yet
- Role of Armed Forces in Disaster ManagemDocument16 pagesRole of Armed Forces in Disaster ManagemMIZANUR RAHMANNo ratings yet
- EIA WarehouseDocument3 pagesEIA WarehouseAnnabella1234No ratings yet
- Camera Booking PaperworkDocument5 pagesCamera Booking Paperworkapi-531920961No ratings yet
- Sample Only Do Not Reproduce: Hazmat Incident ChecklistDocument1 pageSample Only Do Not Reproduce: Hazmat Incident ChecklistLuis Diaz CerdanNo ratings yet
- Triage During A Mass Casualty Incidents (MCI)Document54 pagesTriage During A Mass Casualty Incidents (MCI)SyifaNo ratings yet
- Disaster Management in Japan: Cabinet Office Government of JapanDocument40 pagesDisaster Management in Japan: Cabinet Office Government of JapanAngelica NainggolanNo ratings yet
- Event Risk Assessment1Document10 pagesEvent Risk Assessment1kieran binnsNo ratings yet
- Hai Toolkit For LTCDocument82 pagesHai Toolkit For LTCShannaNo ratings yet
- EIA ShippingDocument1 pageEIA ShippingAnnabella1234No ratings yet
- Thunderstorms, Tornadoes, Lightning: Nature's Most Dangerous StormsDocument16 pagesThunderstorms, Tornadoes, Lightning: Nature's Most Dangerous Stormspolitix100% (2)
- Code Yellow - GnopDocument70 pagesCode Yellow - GnopLinda andayaniNo ratings yet
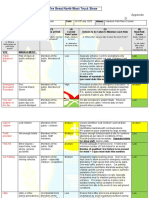
- AW2E - Threat Map & Threat Sheets (Fillable)Document6 pagesAW2E - Threat Map & Threat Sheets (Fillable)Guilherme SouzaNo ratings yet
- JSA 03 - Rev 00B Painting WorksDocument4 pagesJSA 03 - Rev 00B Painting WorksShaffi MohammedNo ratings yet
- Camera Booking PaperworkDocument5 pagesCamera Booking Paperworkapi-545836679No ratings yet
- EC2203Document20 pagesEC2203HoiTik UCNo ratings yet
- Disaster Readiness PROFILEDocument6 pagesDisaster Readiness PROFILEBRGY SEVENONEPAYBNo ratings yet
- Emergency Action Plan Fillable 2022Document2 pagesEmergency Action Plan Fillable 2022Jose E RafolsNo ratings yet
- 1.8 Annex 4 - Bopis DCF Form 3Document3 pages1.8 Annex 4 - Bopis DCF Form 3Aida TagaroNo ratings yet
- Distress ProcedureDocument2 pagesDistress Procedurerigel100% (1)
- 1.8 Standard Operating ProceduresDocument14 pages1.8 Standard Operating ProceduresLalaine Abalos100% (1)
- Military Triag ADocument14 pagesMilitary Triag Asupit1No ratings yet
- Equipment Booking Form 1Document5 pagesEquipment Booking Form 1api-479589840No ratings yet
- Fire Drill Evaluation FormDocument2 pagesFire Drill Evaluation FormQuality Assurance OfficeNo ratings yet
- Report Treatment @kyoceraDocument1 pageReport Treatment @kyoceraJokosatya99 Jokosatya99No ratings yet
- Recording Form1 Masterlist of Grade 1 StudentsDocument1 pageRecording Form1 Masterlist of Grade 1 StudentsSandra Nicole TorresNo ratings yet
- Accident Prevention: Training Module Prepared By:Safety Dept - GCL LoteDocument30 pagesAccident Prevention: Training Module Prepared By:Safety Dept - GCL LotednkishoreNo ratings yet
- Psi On Char SheetDocument4 pagesPsi On Char SheetBrunoNo ratings yet
- Emergency Drill April 2022Document5 pagesEmergency Drill April 2022Zohaib TahirNo ratings yet
- CHRC SWMS Lifting OperationsDocument6 pagesCHRC SWMS Lifting OperationsvsfchanNo ratings yet
- Step 5 - DRADocument19 pagesStep 5 - DRACHICKYNo ratings yet
- Gar 19 DistilledDocument28 pagesGar 19 DistilledAntoni Gonsalo Narvaez CcoyoNo ratings yet
- Okta - Contingency Plan & Hospital Disaster PlanDocument38 pagesOkta - Contingency Plan & Hospital Disaster PlanWidhy Reza PutraNo ratings yet
- Disaster NursingDocument7 pagesDisaster NursingachiemandacNo ratings yet
- Living in Camp Accommodation RA-R9-01-010-01Document1 pageLiving in Camp Accommodation RA-R9-01-010-01cmrig74No ratings yet
- Emergency Action Plan NEWDocument9 pagesEmergency Action Plan NEWMd. Shahadat HossainNo ratings yet
- Who Standardized Emergency Unit Form TraumaDocument2 pagesWho Standardized Emergency Unit Form TraumaJm uniteNo ratings yet
- Manifest Fecal-Septage Form - Tagum City Final 2024Document1 pageManifest Fecal-Septage Form - Tagum City Final 2024lbbagoNo ratings yet
- ReportDocument3 pagesReportSultan Sikandar SajidNo ratings yet
- Daily Consolidated Report of EmergenciesDocument3 pagesDaily Consolidated Report of EmergenciesSultan Sikandar SajidNo ratings yet
- IC Tax Risk Register 9419Document3 pagesIC Tax Risk Register 9419Jamil TchamambeNo ratings yet
- Hot Work PermitDocument1 pageHot Work Permitsaran985100% (1)
- "Year of The Fight Against Corruption and Impunity": National University Jose Faustino Sanchez CarrionDocument34 pages"Year of The Fight Against Corruption and Impunity": National University Jose Faustino Sanchez CarrionSol Julissa Pacheco MillaNo ratings yet
- Disaster NursingDocument52 pagesDisaster Nursingsweta100% (1)
- The Expanse Character SheetDocument2 pagesThe Expanse Character SheetglottNo ratings yet
- Non-Neonatal Tetanus: (ICD 10 Code: A35)Document2 pagesNon-Neonatal Tetanus: (ICD 10 Code: A35)CHICKY100% (1)
- Umass Lowell PCRDocument1 pageUmass Lowell PCRdandude505No ratings yet
- Chelsea Version2Document1 pageChelsea Version2Health BrookNo ratings yet
- Form 2 Information Management System Assessment and Needs Analysis (IMSANA) ToolDocument36 pagesForm 2 Information Management System Assessment and Needs Analysis (IMSANA) ToolHarold Paulo MejiaNo ratings yet
- dm2022-0029 Issuance of Provisional Certification of PCW in 2020Document3 pagesdm2022-0029 Issuance of Provisional Certification of PCW in 2020Harold Paulo MejiaNo ratings yet
- Citizens CharterDocument29 pagesCitizens CharterHarold Paulo MejiaNo ratings yet
- UHC PresentationDocument21 pagesUHC PresentationHarold Paulo Mejia100% (1)
- CHD I Memo Circular 2022 027 Reporting of Monthly Routine Immunization Services Through Web Based Spreadsheet Based On FHSIS Template.Document1 pageCHD I Memo Circular 2022 027 Reporting of Monthly Routine Immunization Services Through Web Based Spreadsheet Based On FHSIS Template.Harold Paulo MejiaNo ratings yet
- (LHS ML) Monitoring TimelinesDocument15 pages(LHS ML) Monitoring TimelinesHarold Paulo MejiaNo ratings yet
- (DOH HPB) PA1 Playbook 2021 - Karinderya para Sa Healthy Pilipinas March 2021 v5Document123 pages(DOH HPB) PA1 Playbook 2021 - Karinderya para Sa Healthy Pilipinas March 2021 v5Harold Paulo MejiaNo ratings yet