Professional Documents
Culture Documents
NCMB 316
Uploaded by
andreatrojilloOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
NCMB 316
Uploaded by
andreatrojilloCopyright:
Available Formats
CARE OF CLIENTS WITH PROBLEMS IN NUTRITIONAL & GASTROINTESTINAL METABOLISM &
ENDOCRINE, PERCEPTION & COORDINATION (ACUTE & CHRONIC) (NCMB 316)
PRELIMS
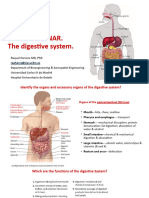
● The organs of the digestive system can be separated into two main
POINTERS: COURSE MODULES groups: those forming the alimentary canal and the accessory digestive
organs
WEEK 1: DISTURBANCES IN INGESTION, DIGESTION, AND
ABSORPTION
WEEK 3: DISORDERS OF THE LIVER, PANCREAS, AND
GALLBLADDER
WEEK 4: DIABETES MELLITUS AND PITUITARY DISORDERS
WEEK 5: SYNDROME OF INAPPROPRIATE ANTIDIURETIC
HORMONE SECRETION, DIABETES INSIPIDUS & THYROID
DISORDERS
WEEK 1: DISTURBANCES IN INGESTION, DIGESTION, AND
ABSORPTION
I. Functions of the Digestive System:
1. Ingestion.
● Food must be placed into the mouth before it can be acted on; this
is an active, voluntary process called ingestion.
2. Propulsion.
● If foods are to be processed by more than one digestive organ, they
must be propelled from one organ to the next; swallowing is one
example of food movement that depends largely on the propulsive
process called peristalsis (involuntary, alternating waves of
contraction and relaxation of the muscles in the organ wall).
3. Food breakdown: mechanical digestion.
● Mechanical digestion prepares food for further degradation by
enzymes by physically fragmenting the foods into smaller pieces,
and examples of mechanical digestion are: mixing of food in the
mouth by the tongue, churning of food in the stomach, and
segmentation in the small intestine.
4. Food breakdown: chemical digestion.
● The sequence of steps in which the large food molecules are broken
down into their building blocks by enzymes is called chemical
digestion.
5. Absorption
● Transport of digested end products from the lumen of the GI tract
to the blood or lymph is absorption, and for absorption to happen,
the digested foods must first enter the mucosal cells by active or
passive transport processes.
6. Defecation
● Defecation is the elimination of indigestible residues from the GI
tract via the anus in the form of feces.
Functions of Digestive System
Ingestion: Secretion: Mixing and
taking food into the release of water, acid, propulsion:
mouth. buffers, and enzymes churning and
into the lumen of the propulsion of food
GI tract. through the GI tract.
Digestion: Absorption: Defecation:
mechanical and passage of digested the elimination of feces
chemical breakdown of products from the GI from the GI tract.
food. tract into the blood
and lymph.
II. Functions of the Digestive System:
● Mechanical digestion in the mouth results from chewing, or
mastication.
● Salivary amylase, which is secreted by the salivary glands, initiates the
breakdown of starch.
● Lingual lipase, which is secreted by lingual glands in the tongue. It breaks
down dietary triglycerides into fatty acids and diglycerides.
III. Anatomy of the Digestive System
1 (Khlaryzel, Mary, Mae, Shane, Rocette)
● Tongue. The muscular tongue occupies the floor of the mouth and has
several bony attachments two of these are to the hyoid bone and the
styloid processes of the skull.
● Lingual frenulum. The lingual frenulum, a fold of mucous membrane,
secures the tongue to the floor of the mouth and limits its posterior
movements.
● Palatine tonsils. At the posterior end of the oral cavity are paired masses
of lymphatic tissue, the palatine tonsils.
● Lingual tonsil. The lingual tonsils cover the base of the tongue just
beyond.
B. PHARYNX
From the mouth, food passes posteriorly into the oropharynx
and laryngopharynx
● Oropharynx. The oropharynx is posterior to the oral cavity.
● Laryngopharynx. The laryngopharynx is continuous with the esophagus
below; both of which are common passageways for food, fluids, and air.
● The pharynx, a funnel-shaped tube that extends from the internal nares
to the esophagus posteriorly and to the larynx anteriorly.
● The pharynx is composed of skeletal muscle and lined by mucous
membrane, and is divided into three parts: the nasopharynx, the
oropharynx, and the laryngopharynx.
C. ESOPHAGUS
The esophagus or gullet, runs from the pharynx through the
diaphragm to the stomach.
● Size and function. About 25 cm (10 inches) long, it is essentially a
passageway that conducts food by peristalsis to the stomach.
● Structure. The walls of the alimentary canal organs from the esophagus
to the large intestine are made up of the same four basic tissue layers or
tunics.
○ The esophagus is a collapsible muscular tube, about 25 cm (10 in.)
long, that lies posterior to the trachea. The esophagus begins at
the inferior end of the laryngopharynx and passes through the
mediastinum anterior to the vertebral column.
○ Then it pierces the diaphragm through an opening called the
esophageal hiatus, and ends in the superior portion of the
stomach.
● Mucosa. The mucosa is the innermost layer, a moist membrane that lines
the cavity, or lumen, of the organ; it consists primarily of a surface
epithelium, plus a small amount of connective tissue (lamina propria)
and a scanty smooth muscle layer.
○ The mucosa of the esophagus consists of nonkeratinized stratified
squamous epithelium, lamina propria, and a muscularis muscosae.
○ At each end of the esophagus, the muscularis becomes slightly
more prominent and forms two sphincters—
■ the upper esophageal sphincter (UES), which consists of
skeletal muscle, and
■ the lower esophageal sphincter (LES), which consists of
smooth muscle.
● Submucosa. The submucosa is found just beneath the mucosa; it is a soft
connective tissue layer containing blood vessels, nerve endings, lymph
nodules, and lymphatic vessels.
● Muscularis externa. The muscularis externa is a muscle layer typically
made up of an inner circular layer and an outer longitudinal layer of
smooth muscle cells.
● Serosa. The serosa is the outermost layer of the wall that consists of a
single layer of flat serous fluid-producing cells, the visceral peritoneum.
● Intrinsic nerve plexuses. The alimentary canal wall contains two
important intrinsic nerve plexuses- the submucosal nerve plexus and the
myenteric nerve plexus, both of which are networks of nerve fibers that
Organs of the Alimentary (Gastrointestinal) Canal are actually part of the autonomic nervous system and help regulate the
mobility and secretory activity of the GI tract organs.
● The alimentary canal, also called the gastrointestinal tract, is a
continuous, hollow muscular tube that winds through the ventral body Three Stages of Deglutition (Swallowing)
cavity and is open at both ends.
● Its organs include the mouth, most of the pharynx, esophagus, stomach,
small intestine, and large intestine voluntary stage: pharyngeal stage: esophageal stage:
in which the bolus is the involuntary the involuntary
A. MOUTH passed into the passage of the bolus passage of the bolus
Food enters the digestive tract through the mouth, or oral oropharynx through the pharynx through the esophagus
cavity, a mucous membrane-lined cavity. into the esophagus into the stomach
● Lips. The lips (labia) protect its anterior opening.
● Cheeks. The cheeks form its lateral walls.
● Palate. The hard palate forms its anterior roof, and the soft palate forms
its posterior roof.
● Uvula. The uvula is a fleshy finger-like projection of the soft palate, which
extends inferiorly from the posterior edge of the soft palate.
● Vestibule. The space between the lips and the cheeks externally and the
teeth and gums internally is the vestibule.
● Oral cavity proper. The area contained by the teeth is the oral cavity
proper.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 2
about 4 liters (1 gallon) of food, but when it is empty it collapses inward
on itself.
● Rugae. The mucosa of the stomach is thrown into large folds called rugae
when it is empty.
● Greater curvature. The convex lateral surface of the stomach is the
greater curvature.
● Lesser curvature. The concave medial surface is the lesser curvature.
● Lesser omentum. The lesser omentum, a double layer of peritoneum,
extends from the liver to the greater curvature.
● Greater omentum. The greater omentum, another extension of the
peritoneum, drapes downward and covers the abdominal organs like a
lacy apron before attaching to the posterior body wall, and is riddled with
fat, which helps to insulate, cushion, and protect the abdominal organs.
● Stomach mucosa. The mucosa of the stomach is a simple columnar
epithelium composed entirely of mucous cells that produce a protective
layer of bicarbonate-rich alkaline mucus that clings to the stomach
mucosa and protects the stomach wall from being damaged by acid and
digested by enzymes.
● Gastric glands. This otherwise smooth lining is dotted with millions of
deep gastric pits, which lead into gastric glands that secrete the solution
called gastric juice.
● Intrinsic factor. Some stomach cells produce intrinsic factor, a substance
needed for the absorption of vitamin b12 from the small intestine.
● Chief cells. The chief cells produce protein-digesting enzymes, mostly
pepsinogens.
● Parietal cells. The parietal cells produce corrosive hydrochloric acid,
which makes the stomach contents acidic and activates the enzymes.
● Enteroendocrine cells. The enteroendocrine cells produce local
hormones such as gastrin, that are important to the digestive activities
of the stomach.
● Chyme. After food has been processed, it resembles heavy cream and is
D. STOMACH called chyme
Different regions of the stomach have been named, and they
include the following: E. SMALL INTESTINE
The small intestine is the body’s major digestive organ.
● Location. The C-shaped stomach is on the left side of the abdominal ● Location. The small intestine is a muscular tube extending from the
cavity, nearly hidden by the liver and the diaphragm. pyloric sphincter to the large intestine.
● Function. The stomach acts as a temporary “storage tank” for food as ● Size. It is the longest section of the alimentary tube, with an average
well as a site for food breakdown. length of 2.5 to 7 m (8 to 20 feet) in a living person.
○ Mixes saliva, food, and gastric juice to form chyme. ● Subdivisions. The small intestine has three subdivisions: the duodenum,
○ Serves as a reservoir for food before release into small intestine. the jejunum, and the ileum, which contribute 5 percent, nearly 40
○ Secretes gastric juice, which contains HCl, percent, and almost 60 percent of the small intestine, respectively.
pepsin, intrinsic factor, and gastric lipase . ● Ileocecal valve. The ileum meets the large intestine at the ileocecal
○ Secretes gastrin into blood. valve, which joins the large and small intestine.
● Cardiac region. The cardiac region surrounds the cardioesophageal ● Hepatopancreatic ampulla. The main pancreatic and bile ducts join at
sphincter, through which food enters the stomach from the esophagus. the duodenum to form the flasklike hepatopancreatic ampulla, literally,
● Fundus. The fundus is the expanded part of the stomach lateral to the the ” liver-pacreatic-enlargement”.
cardiac region. ● Duodenal papilla. From there, the bile and pancreatic juice travel
● Body. The body is the midportion, and as it narrows inferiorly, it becomes through the duodenal papilla and enter the duodenum together.
the pyloric antrum, and then the funnel-shaped pylorus. ● Microvilli. Microvilli are tiny projections of the plasma membrane of the
● Pylorus. The pylorus is the terminal part of the stomach and it is mucosa cells that give the cell surface a fuzzy appearance, sometimes
continuous with the small intestine through the pyloric sphincter or referred to as the brush border; the plasma membranes bear enzymes
valve. (brush border enzymes) that complete the digestion of proteins and
● Size. The stomach varies from 15 to 25 cm in length, but its diameter and carbohydrates in the small intestine.
volume depend on how much food it contains; when it is full, it can hold
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 3
● Villi. Villi are fingerlike projections of the mucosa that give it a velvety
appearance and feel, much like the soft nap of a towel.
● Lacteal. Within each villus is a rich capillary bed and a modified lymphatic
capillary called a lacteal.
● Circular folds. Circular folds, also called plicae circulares, are deep folds
of both mucosa and submucosa layers, and they do not disappear when
food fills the small intestine.
● Peyer’s patches. In contrast, local collections of lymphatic tissue found
in the submucosa increase in number toward the end of the small
intestine.
● Functions.
○ Segmentations mix chyme with digestive juices and bring food into
contact with the mucosa for absorption; peristalsis propels chyme
through the small intestine.
○ Completes the digestion of carbohydrates, proteins, and lipids;
begins and completes the digestion of nucleic acids.
○ Absorbs about 90% of nutrients and water that pass through the
digestive system.
MECHANICAL DIGESTION IN THE SMALL INTESTINE
● Size. About 1.5 m (5 feet) long, it extends from the ileocecal valve to the
anus.
● The two types of movements of the small intestine: ● Functions. Its major functions are to dry out indigestible food residue by
● Segmentations absorbing water and to eliminate these residues from the body as feces.
○ Segmentations mix chyme with the digestive juices and bring the ● Subdivisions. It frames the small intestines on three sides and has the
particles of food into contact with the mucosa for absorption following subdivisions: cecum, appendix, colon, rectum, and anal canal.
● Migrating motility complex (MMC) ● Cecum. The saclike cecum is the first part of the large intestine.
○ begins in the lower portion of the stomach and pushes chyme ● Appendix. Hanging from the cecum is the wormlike appendix, a potential
forward along a short stretch of small intestine before dying out trouble spot because it is an ideal location for bacteria to accumulate and
multiply.
F. LARGE INTESTINE ● Ascending colon. The ascending colon travels up the right side of the
The large intestine is much larger in diameter than the small abdominal cavity and makes a turn, the right colic (or hepatic) flexure, to
intestine but shorter in length. travel across the abdominal cavity.
● Transverse colon. The ascending colon makes a turn and continuous to
be the transverse colon as it travels across the abdominal cavity.
● Descending colon. It then turns again at the left colic (or splenic) flexure,
and continues down the left side as the descending colon.
● Sigmoid colon. The intestine then enters the pelvis, where it becomes
the S-shaped sigmoid colon.
● Anal canal. The anal canal ends at the anus which opens to the exterior.
● External anal sphincter. The anal canal has an external voluntary
sphincter, the external anal sphincter, composed of skeletal muscle.
● Internal involuntary sphincter. The internal involuntary sphincter is
formed by smooth muscles.
● Functions:
○ Haustral churning, peristalsis, and mass peristalsis drive the
contents of the colon into the rectum.
○ Bacteria in the large intestine convert proteins to amino acids,
break down amino acids, and produce some B vitamins and
vitamin K.
○ Absorbing some water, ions, and vitamins.
○ Forming feces.
○ Defecating (emptying the rectum).
THE DEFECATION REFLEX
● Diarrhea is an increase in the frequency, volume, and fluid content of the
feces caused by increased motility of and decreased absorption by the
intestines.
● Constipation refers to infrequent or difficult defecation caused by
decreased motility of the intestines.
PHASES OF DIGESTION
● During the cephalic phase of digestion, the smell, sight, thought, or initial
taste of food activates neural centers in the cerebral cortex,
hypothalamus, and brain stem. The brain stem then activates the facial
(VII), glossopharyngeal (IX), and vagus (X) nerves. The facial and
glossopharyngeal nerves stimulate the salivary glands to secrete saliva,
while the vagus nerves stimulate the gastric glands to secrete gastric
juice.
● The intestinal phase of digestion begins once food enters the small
intestine.
● The intestinal phase of digestion begins once food enters the small
intestine. Those occurring during the intestinal phase have inhibitory
effects that slow the exit of chyme from the stomach.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 4
● The branch of dentistry that is concerned with the prevention, diagnosis,
and treatment of diseases that affect the pulp, root, periodontal
ligament, and alveolar bone is known as Endodontics.
● Orthodontics is a branch of dentistry that is concerned with the
prevention and correction of abnormally aligned teeth.
● Periodontics is a branch of dentistry concerned with the treatment of
abnormal conditions of the tissues immediately surrounding the teeth,
such as gingivitis.
Accessory Digestive Organs
● Other than the intestines and the stomach include the teeth, tongue,
salivary glands, liver, gallbladder, and pancreas.
● The following are also part of the digestive system:
G. TEETH
The role the teeth play in food processing needs little introduction; we
masticate, or chew, by opening and closing our jaws and moving them
from side to side while continuously using our tongue to move the food
between our teeth.
● Function. The teeth tear and grind the food, breaking it down into
smaller fragments.
● Deciduous teeth. The first set of teeth is the deciduous teeth, also called
baby teeth or milk teeth, and they begin to erupt around 6 months, and
a baby has a full set (20 teeth) by the age of 2 years.
● Permanent teeth. As the second set of teeth, the deeper permanent
teeth, enlarge and develop, the roots of the milk teeth are reabsorbed,
and between the ages of 6 to 12 years they loosen and fall out.
● Incisors. The chisel-shaped incisors are adapted for cutting. H. SALIVARY GLANDS
● Canines. The fanglike canines are for tearing and piercing. Three pairs of salivary glands empty their secretions into the mouth.
● Premolars and molars. Premolars (bicuspids) and molars have broad
crowns with round cusps (tips) and are best suited for grinding. ● Parotid glands. The large parotid glands lie anterior to the ears and
● Crown. The enamel-covered crown is the exposed part of the tooth empty their secretions into the mouth.
above the gingiva or gum. ● Submandibular and sublingual glands. The submandibular and
● Enamel. Enamel is the hardest substance in the body and is fairly brittle sublingual glands empty their secretions into the floor of the mouth
because it is heavily mineralized with calcium salts. through tiny ducts.
● Root. The outer surface of the root is covered by a substance called ● Saliva. The product of the salivary glands, saliva, is a mixture of mucus
cementum, which attaches the tooth to the periodontal membrane and serous fluids.
(ligament). ● Salivary amylase. The clear serous portion contains an enzyme, salivary
● Dentin. Dentin, a bonelike material, underlies the enamel and forms the amylase, in a bicarbonate-rich juice that begins the process of starch
bulk of the tooth. digestion in the mouth.
● Pulp cavity. It surrounds a central pulp cavity, which contains a number
of structures (connective tissue, blood vessels, and nerve fibers)
collectively called the pulp.
● Root canal. Where the pulp cavity extends into the root, it becomes the
root canal, which provides a route for blood vessels, nerves, and other
pulp structures to enter the pulp cavity of the tooth
Study for Teeth
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 5
I. PANCREAS
Only the pancreas produces enzymes that break down all
categories of digestible foods.
● Location. Located under the diaphragm, more to the right side of the
body, it overlies and almost completely covers the stomach.
● Falciform ligament. The liver has four lobes and is suspended from the
diaphragm and abdominal wall by a delicate mesentery cord, the
falciform ligament.
● Location. The pancreas is a soft, pink triangular gland that extends across ● Function. The liver’s digestive function is to produce bile.
the abdomen from the spleen to the duodenum; but most of the ○ Carbohydrate metabolism.
pancreas lies posterior to the parietal peritoneum, hence its location is ○ Lipid metabolism.
referred to as retroperitoneal. ○ Protein metabolism.
● Pancreatic enzymes. The pancreatic enzymes are secreted into the ○ Processing of drugs and hormones.
duodenum in an alkaline fluid that neutralizes the acidic chyme coming ○ Excretion of bilirubin.
in from the stomach. ○ Synthesis of bile salts.
● Endocrine function. The pancreas also has an endocrine function; it ○ Storage for certain vitamins (A, B12, D, E, and K) and minerals (iron
produces hormones insulin and glucagon. and copper)
○ Phagocytosis.
○ Activation of vitamin D.
● Bile. Bile is a yellow-to-green, watery solution containing bile salts, bile
pigments, cholesterol, phospholipids, and a variety of electrolytes.
● Bile salts. Bile does not contain enzymes but its bile salts emulsify fats by
physically breaking large fat globules into smaller ones, thus providing
more surface area for the fat-digesting enzymes to work on.
ROLE AND COMPOSITION OF BILE
● Each day, hepatocytes secrete 800–1000 mL (about 1 qt) of bile, a yellow,
brownish, or olive-green liquid. It has a pH of 7.6–8.6 and consists mostly
of water, bile salts, cholesterol, a phospholipid called lecithin, bile
pigments, and several ions.
● The principal bile pigment is bilirubin. The phagocytosis of aged red blood
cells liberates iron, globin, and bilirubin.
● One of its breakdown products—stercobilin—gives feces their normal
brown color.
● Bile salts, play a role in emulsification, the breakdown of large lipid
globules into a suspension of small lipid globules.
J. LIVER ● Between meals, after most absorption has occurred, bile flows into the
The liver is the largest gland in the body. gallbladder for storage because the sphincter of the hepatopancreatic
ampulla (sphincter of Oddi) closes off the entrance to the duodenum.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 6
Food Propulsion
K. GALLBLADDER ● Peristalsis is responsible for the movement of food towards the digestive
While in the gallbladder, bile is concentrated by the removal of water. site until the intestines.
○ Peristalsis. Once the food has been well mixed, a rippling peristalsis
● Location. The gallbladder is a small, thin-walled green sac that snuggles
begins in the upper half of the stomach, and the contractions
in a shallow fossa in the inferior surface of the liver.
increase in force as the food approaches the pyloric valve.
● Cystic duct. When food digestion is not occurring, bile backs up the cystic
○ Pyloric passage. The pylorus of the stomach, which holds about 30
duct and enters the gallbladder to be stored.
ml of chyme, acts like a meter that allows only liquids and very
IV. Physiology of the Digestive System small particles to pass through the pyloric sphincter; and because
the pyloric sphincter barely opens, each contraction of the stomach
● Specifically, the digestive system takes in food (ingests it), breaks it down muscle squirts 3 ml or less of chyme into the small intestine.
physically and chemically into nutrient molecules (digests it), and ○ Enterogastric reflex. When the duodenum is filled with chyme and
absorbs the nutrients into the bloodstream, then, it rids the body of its wall is stretched, a nervous reflex, the enterogastric reflex,
indigestible remains (defecates). occurs; this reflex “puts the brakes on” gastric activity and slows
the emptying of the stomach by inhibiting the vagus nerves and
A. Activities Occurring in the Mouth, Pharynx, and tightening the pyloric sphincter, thus allowing time for intestinal
Esophagus processing to catch up.
● The activities that occur in the mouth, pharynx, and esophagus are food C. Activities of the Small Intestine
ingestion, food breakdown, and food propulsion.
Food Ingestion and Breakdown. ● The activities of the small intestine are food breakdown and absorption
● Once food is placed in the mouth, both mechanical and chemical and food propulsion.
digestion begin. Food Breakdown and Absorption
○ Physical breakdown. First, the food is physically broken down into ● Food reaching the small intestine is only partially digested.
smaller particles by chewing. ○ Digestion. Food reaching the small intestine is only partially
○ Chemical breakdown. Then, as the food is mixed with saliva, digested; carbohydrate and protein digestion has begun, but
salivary amylase begins the chemical digestion of starch, breaking virtually no fats have been digested up to this point.
it down into maltose. ○ Brush border enzymes. The microvilli of small intestine cells bears
○ Stimulation of saliva. When food enters the mouth, much larger a few important enzymes, the so-called brush border enzymes, that
amounts of saliva pour out; however, the simple pressure of break down double sugars into simple sugars and complete protein
anything put into the mouth and chewed will also stimulate the digestion.
release of saliva. ○ Pancreatic juice. Foods entering the small intestine are literally
○ Passageways. The pharynx and the esophagus have no digestive deluged with enzyme-rich pancreatic juice ducted in from the
function; they simply provide passageways to carry food to the next pancreas, as well as bile from the liver; pancreatic juice contains
processing site, the stomach. enzymes that, along with brush border enzymes, complete the
Food Propulsion – Swallowing and Peristalsis. digestion of starch, carry out about half of the protein digestion,
● For food to be sent on its way to the mouth, it must first be swallowed. and are totally responsible for fat digestion and digestion of nucleic
○ Deglutition. Deglutition, or swallowing, is a complex process that acids.
involves the coordinated activity of several structures (tongue, soft ○ Chyme stimulation. When chyme enters the small intestine, it
palate, pharynx, and esophagus). stimulates the mucosa cells to produce several hormones; two of
○ Buccal phase of deglutition. The first phase, the voluntary buccal these are secretin and cholecystokinin which influence the release
phase, occurs in the mouth; once the food has been chewed and of pancreatic juice and bile.
well mixed with saliva, the bolus (food mass) is forced into the ○ Absorption. Absorption of water and of the end products of
pharynx by the tongue. digestion occurs all along the length of the small intestine; most
○ Pharyngeal-esophageal phase. The second phase, the involuntary substances are absorbed through the intestinal cell plasma
pharyngeal-esophageal phase, transports food through the membranes by the process of active transport.
pharynx and esophagus; the parasympathetic division of the ○ Diffusion. Lipids or fats are absorbed passively by the process of
autonomic nervous system controls this phase and promotes the diffusion.
mobility of the digestive organs from this point on. ○ Debris. At the end of the ileum, all that remains are some water,
○ Food routes. All routes that the food may take, except the desired indigestible food materials, and large amounts of bacteria; this
route distal into the digestive tract, are blocked off; the tongue debris enters the large intestine through the ileocecal valve.
blocks off the mouth; the soft palate closes off the nasal passages; Food Propulsion
the larynx rises so that its opening is covered by the flaplike ● Peristalsis is the major means of propelling food through the digestive
epiglottis. tract.
○ Stomach entrance. Once food reaches the distal end of the ○ Peristalsis. The net effect is that the food is moved through the
esophagus, it presses against the cardioesophageal sphincter, small intestine in much the same way that toothpaste is squeezed
causing it to open, and food enters the stomach. from the tube.
○ Constrictions. Rhythmic segmental movements produce local
B. Activities of the Stomach constrictions of the intestine that mix the chyme with the digestive
juices, and help to propel food through the intestine.
● The activities of the stomach involve food breakdown and food
propulsion. D. Activities of the Large Intestine
Food Breakdown
● The sight, smell, and taste of food stimulate parasympathetic nervous ● The activities of the large intestine are food breakdown and absorption
system reflexes, which increase the secretion of gastric juice by the and defecation.
stomach glands Food Breakdown and Absorption
○ Gastric juice. Secretion of gastric juice is regulated by both neural ● What is finally delivered to the large intestine contains few nutrients, but
and hormonal factors. that residue still has 12 to 24 hours more to spend there.
○ Gastrin. The presence of food and a rising pH in the stomach ○ Metabolism. The “resident” bacteria that live in its lumen
stimulate the stomach cells to release the hormone gastrin, which metabolize some of the remaining nutrients, releasing gases
prods the stomach glands to produce still more of the protein (methane and hydrogen sulfide) that contribute to the odor of
digesting enzymes (pepsinogen), mucus, and hydrochloric acid. feces.
○ Pepsinogen. The extremely acidic environment that hydrochloric ○ Flatus. About 50 ml of gas (flatus) is produced each day, much more
acid provides is necessary, because it activates pepsinogen to when certain carbohydraterich foods are eaten.
pepsin, the active protein-digesting enzyme. ○ Absorption. Absorption by the large intestine is limited to the
○ Rennin. Rennin, the second protein-digesting enzyme produced by absorption of vitamin K, some B vitamins, some ions, and most of
the stomach, works primarily on milk protein and converts it to a the remaining water.
substance that looks like sour milk. ○ Feces. Feces, the more or less solid product delivered to the
○ Food entry. As food enters and fills the stomach, its wall begins to rectum, contains undigested food residues, mucus, millions of
stretch (at the same time as the gastric juices are being secreted). bacteria, and just enough water to allow their smooth passage.
○ Stomach wall activation. Then the three muscle layers of the Propulsion of the Residue and Defecation
stomach wall become active; they compress and pummel the food, ● When presented with residue, the colon becomes mobile, but its
breaking it apart physically, all the while continuously mixing the contractions are sluggish or shortlived.
food with the enzyme-containing gastric juice so that the semifluid
chyme is formed.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 7
○ Haustral contractions. The movements most seen in the colon are recommend not chewing gum, eating mints, or smoking cigarettes after
haustral contractions, slow segmenting movements lasting about midnight the night before a barium swallow test.
one minute that occur every 30 minutes or so. ● The test takes around 60 minutes and will take place in the X-ray
○ Propulsion. As the haustrum fills with food residue, the distension department of the hospital. A person will need to change into a hospital
stimulates its muscle to contract, which propels the luminal gown.
contents into the next haustrum. ● In the X-ray room, the person drinks the barium liquid. It often has a
○ Mass movements. Mass movements are long, slow-moving, but chalky taste but can sometimes be flavored.
powerful contractile waves that move over large areas of the colon ● A person will lie on a tilting table for part of the examination.
three or four times daily and force the contents toward the rectum. ● In some cases, a person will be given an injection to relax their stomach.
○ Rectum. The rectum is generally empty, but when feces are forced ● A person will be standing for some parts of the examination, and lying
into it by mass movements and its wall is stretched, the defecation down on a tilting table for other parts. This allows the liquid to travel
reflex is initiated. through the body, and for the radiologist and radiographer to take a
○ Defecation reflex. The defecation reflex is a spinal (sacral region) selection of images.
reflex that causes the walls of the sigmoid colon and the rectum to ● People do not have to stay in hospital after the test and are free to go
contract and anal sphincters to relax. home as soon as it is complete. The results usually arrive within 1-2
○ Impulses. As the feces is forced into the anal canal, messages reach weeks.
the brain giving us time to make a decision as to whether the
external voluntary sphincter should remain open or be constricted B. BARIUM ENEMA TEST
to stop passage of feces.
○ Relaxation. Within a few seconds, the reflex contractions end and
rectal walls relax; with the next mass movement, the defecation
reflex is initiated again.
V. Laboratory Assessments
A. BARIUM SWALLOW TEST
● A barium enema is an X-ray procedure used to examine the rectum and
colon, often used as a complement to lower gastrointestinal (GI)
endoscopy.
● It is a diagnostic tool for patients with, for example, lower GI bleeding,
altered bowel habit or abdominal pain, or to screen for polyps and
colorectal cancer.
Contraindications include:
● acute colitis/diverticulitis
● A special type of imaging test that uses barium and Xrays to create ● recent polypectomy or colonic biopsy
images of your upper gastrointestinal (GI) tract. Your upper GI tract ● older patients (>70 years old)
includes the back of your mouth and throat (pharynx) and your ● pregnancy
esophagus. How does it work?
● Barium is used during a swallowing test to make certain areas of the body ● Contrast is passed into the rectum to enhance X-ray pictures of the
show up more clearly on an X-ray. The radiologist will be able to see size bowel. Barium enemas may use a single contrast (barium only) or double
and shape of the pharynx and esophagus. He or she will also be able see contrast (barium and air). Double-contrast studies are more common
how you swallow. These details might not be seen on a standard X-ray. and successful.
● Barium is used only for imaging tests for the GI tract. ● Patient Preparation
● A barium swallow test may be used by itself or as part of an upper GI ● Bowel preparation: this varies, but often involves a period of low-residue
series. This series looks at your esophagus, stomach, and the first part of diet and oral/laxative washout. Preparation is vital for good views of the
the small intestine (duodenum). bowel: the patient should receive full instructions on preparation and the
● Fluoroscopy is often used during a barium swallow test. Fluoroscopy is a procedure.
kind of X-ray “movie.” ● The radiologist should be supplied with a full patient history.
● Barium is a white liquid that is visible on X-rays. Barium passes through
the digestive system and does not cause a person any harm.
● As it passes through the body, barium coats the inside of the food pipe, The Procedure
stomach, or bowel, causing the outlines of the organs to appear on X- ● The patient is cannulated and may be given intravenous antispasmodic
ray. medication (for example hyoscine butylbromide) to make the procedure
Why are barium swallow tests used? more comfortable and to aid the passage of barium.
● A barium swallow can help a doctor identify problems in the food pipe, ● The patient is positioned in a left lateral position on an X-ray table.
stomach, or bowel. ● A digital rectal examination is then performed.
● A barium swallow test may be used if someone has any of the following ● A rectal catheter is lubricated and inserted into the rectum. This has two
conditions: connectors. One connector is for for passing barium and the other is for
○ frequent, painful heartburn insufflating air.
○ gastric reflux, where food or acid keeps coming back up the food ● The patient is placed prone.
pipe ● Liquid barium is passed via a giving set into the catheter. It is passed
○ difficulty eating, drinking, or swallowing slowly to prevent the patient experiencing discomfort or an urge to
● This test can give a doctor information about how the person is defecate.
swallowing. ● X-ray screening takes place as the barium is passed so the radiologist can
● It can also reveal if someone has any of the following in their food pipe, observe filling. The amount instilled depends on the patient. The
stomach, or the first part of the radiologist stops once the rectum is filled and the barium continues to
● bowel: pass around the colon. The radiologist may change the patient’s position
○ ulcers as necessary in order to aid filling.
○ abnormal growths ● Once the contrast reaches the splenic flexure, the patient returns to the
○ blockages prone position and air is insufflated. As air enters, the colon inflates and
○ narrowing the images of the mucosa become clearer.
● If someone has a tumor, this will show up on the X-ray as an irregular ● Radiography staff may assist in moving the patient to aid filling and to
outline that extends from the wall provide reassurance.
● of the affected organ. ● Screening continues until the radiologist identifies the caecum, by seeing
Procedure the appendix or by seeing barium entering the small bowel.
● People who are undergoing a barium swallow should not eat or drink for ● Once the entire colon is filled further pictures are taken in individual
a few hours before the test. In some cases, the doctor may ask the positions to obtain complete views.
person to stop taking medication before the test. Some hospitals ● The radiographer ensures all pictures are valid.
● The rectum is emptied of barium and the catheter removed.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 8
● The patient passes barium for several hours after the procedure. ● A gastroscopy is a very safe procedure, but like all medical procedures it
Risks and side effects does carry a risk of complications. Possible complications that can occur
● Patients may feel nauseous after a barium swallow test or become include:
constipated. Drinking lots of fluids can help to relieve constipation. ○ a reaction to the sedative, which can cause problems with your
Symptoms of nausea should improve as the barium passes through the breathing, heart rate and blood pressure
system. ○ internal bleeding
● It is normal for people to have white-colored stools the first few times ○ tearing (perforation) of the lining of your oesophagus, stomach or
they use the toilet after having a barium swallow test. duodenum
● Some people might worry about being exposed to radiation as part of
the X-ray process. However, the amount of radiation a person is exposed D. GASTROSCOPY
to is minimal.
● Sometimes, the injection given to relax the stomach can cause
temporary blurred vision.
Special considerations
● People should not have a barium swallow test if they are pregnant.
● If someone has glaucoma or heart problems and needs to have a barium
swallow, the doctor may not give the stomach-relaxing injection.
● If someone has diabetes then the doctor will schedule a morning
appointment for the barium swallow.
● People who use insulin will be asked to miss their morning dose and
maybe the previous evening’s dose. They should bring their insulin and
some food to have after the test. However, those who take long-acting
insulin should continue taking this.
Major Complications
● Colonic perforation.
● Haemorrhage.
● Oversedation.
● Cardiac arrhythmia.
Minor Complications
● Constipation. ● Esophagogastroduodenoscopy (EGD) is a test to examine the lining of
● Abdominal discomfort. the esophagus, stomach, and first part of the small intestine (the
● Rectal bleeding. duodenum).
● Flatus. How the Test is Performed
● EGD is done in a hospital or medical center. The procedure uses an
C. GASTROSCOPY endoscope. This is a flexible tube with a light and camera at the end. The
procedure is done as follows:
○ During the procedure, breathing, heart rate, blood pressure, and
oxygen level are checked. Wires are attached to certain areas of
the body and then to machines that monitor these vital signs.
○ The patient receives medicine into a vein to help you relax. The
patient should feel no pain and not remember the procedure.
○ A local anesthetic may be sprayed into the mouth to prevent you
from coughing or gagging when the scope is inserted.
○ A mouth guard is used to protect the teeth and the scope. Dentures
must be removed before the procedure begins.
○ The patient then lie on your left side.
○ The scope is inserted through the esophagus (food pipe) to the
stomach and duodenum. The duodenum is the first part of the
small intestine.
● A gastroscopy is a procedure where a thin, flexible tube called an ○ Air is put through the scope to make it easier for the doctor to see.
endoscope is used to look inside the oesophagus (gullet), stomach and ○ The lining of the esophagus, stomach, and upper duodenum is
first part of the small intestine (duodenum). It's also sometimes referred examined. Biopsies can be taken through the scope. Biopsies are
to as an upper gastrointestinal endoscopy. The endoscope has a light and tissue samples that are looked at under the microscope.
a camera at one end. The camera sends images of the inside of your ○ Different treatments may be done, such as stretching or widening
oesophagus, stomach and duodenum to a monitor. a narrowed area of the esophagus.
Why a gastroscopy may be used ○ After the test is finished, the client will not be able to have food
● A gastroscopy can be used to: and liquid until their gag reflex returns (so you do not choke).
○ investigate problems such as difficulty swallowing (dysphagia) or ○ The test lasts about 30 to 60 minutes.
persistent abdominal (tummy) pain Major Complications
○ diagnose conditions such as stomach ulcers or gastro-oesophageal ● Colonic perforation.
reflux disease (GORD) ● Haemorrhage.
○ treat conditions such as bleeding ulcers, a blockage in the ● Oversedation.
oesophagus, non-cancerous growths (polyps) or small cancerous ● Cardiac arrhythmia.
tumours Minor Complications
● A gastroscopy used to check symptoms or confirm a diagnosis is known ● Constipation.
as a diagnostic gastroscopy. A gastroscopy used to treat a condition is ● Abdominal discomfort.
known as a therapeutic gastroscopy. ● Rectal bleeding.
The gastroscopy procedure ● Flatus.
● A gastroscopy often takes less than 15 minutes, although it may take
longer if it's being used to treat a condition. VI. DISEASES OF THE UPPER GASTROINTESTINAL TRACT
● It's usually carried out as an outpatient procedure, which means you
won't have to spend the night in hospital.
● Before the procedure, your throat will be numbed with a local I. Gastroesophageal Reflux Disease (GERD)
anaesthetic spray. You can also choose to have a sedative, if you prefer.
This means you will still be awake, but will be drowsy and have reduced
● Some degree of gastroesophageal reflux (backflow of gastric or duodenal
contents into the esophagus) is normal in both adults and children.
awareness about what's happening.
Excessive reflux may occur because of an incompetent lower esophageal
● The doctor carrying out the procedure will place the endoscope in the sphincter, pyloric stenosis, or a motility disorder. The incidence of GERD
back of your mouth and ask you to swallow the first part of the tube. It seems to increase with aging.
will then be guided down your esophagus and into your stomach. Clinical Manifestations
● The procedure shouldn't be painful, but it may be unpleasant or ● pyrosis (burning sensation in the esophagus),
uncomfortable at times. ● dyspepsia (indigestion),
What are the risks? ● regurgitation, dysphagia or odynophagia (pain on swallowing),
● hypersalivation, and
● esophagitis.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 9
Assessment and Diagnostic Findings ○ If symptoms persist, intravenous fluids may be necessary. If
● Diagnostic testing may include an endoscopy or barium swallow to bleeding is present, management is similar to that of upper GI tract
evaluate damage to the esophageal mucosa. hemorrhage. If gastritis is due to ingestion of strong acids or alkali,
● Ambulatory 12- to 36-hour esophageal pH monitoring is used to evaluate dilute and neutralize the acid with common antacids (eg, aluminum
the degree of acid reflux. hydroxide); neutralize alkali with diluted lemon juice or diluted
● Bilirubin monitoring (Bilitec) is used to measure bile reflux patterns. vinegar.
Exposure to bile can cause mucosal damage. ○ If corrosion is extensive or severe, avoid emetics and lavage
Management because of danger of perforation. Supportive therapy may include
● Management begins with teaching the patient to avoid situations that nasogastric intubation, analgesic agents and sedatives, antacids,
decrease lower esophageal sphincter pressure or cause esophageal and IV fluids.
irritation. ○ Fiberoptic endoscopy may be necessary; emergency surgery may
● The patient is instructed to eat a low-fat diet; to avoid caffeine, tobacco, be required to remove gangrenous or perforated tissue; gastric
beer, milk, foods containing peppermint or spearmint, and carbonated resection (gastrojejunostomy) may be necessary to treat pyloric
beverages; to avoid eating or drinking 2 hours before bedtime; to obstruction.
maintain normal body weight; to avoid tight-fitting clothes; to elevate ● Chronic Gastritis
the head of the bed on 6- to 8-inch (15- to 20-cm) blocks; and to elevate ○ Diet modification, rest, stress reduction, avoidance of alcohol and
the upper body on pillows. NSAIDs, and pharmacotherapy are key treatment measures.
● If reflux persists, antacids or H2 receptor antagonists, such as famotidine Gastritis related to H. pylori infection is treated with selected drug
(Pepcid), nizatidine (Axid), or ranitidine (Zantac), may be prescribed. combinations.
● Proton pump inhibitors (medications that decrease the release of gastric Nursing Management
acid, such as lansoprazole [Prevacid], rabeprazole [AcipHex], Reducing Anxiety
esomeprazole [Nexium], omeprazole [Prilosec], and pantoprazole ● Carry out emergency measures for ingestion of acids or alkalies.
[Protonix]) may be used; however, these products may increase ● Offer supportive therapy to patient and family during treatment and
intragastric bacterial growth and the risk of infection. after the ingested acid or alkali has been neutralized or diluted.
● In addition, the patient may receive prokinetic agents, which accelerate ● Prepare patient for additional diagnostic studies (endoscopy) or surgery.
gastric emptying. These agents include bethanechol (Urecholine), ● Calmly listen to and answer questions as completely as possible; explain
domperidone (Motilium), and metoclopramide (Reglan). Because all procedures and treatments.
metoclopramide can have extrapyramidal side effects that are increased Promoting Optimal Nutrition
in certain neuromuscular disorders, such as Parkinson’s disease, it should ● Provide physical and emotional support for patients with acute gastritis.
be used only if no other option exists, and the patient should be ● Help patient manage symptoms (eg, nausea, vomiting, heartburn, and
monitored closely. fatigue).
● If medical management is unsuccessful, surgical intervention may be ● Avoid foods and fluids by mouth for hours or days until acute symptoms
necessary. Surgical management involves a Nissen fundoplication subside.
(wrapping of a portion of the gastric fundus around the sphincter area of ● Offer ice chips and clear liquids when symptoms subside.
the esophagus). ● Encourage patient to report any symptoms suggesting a repeat episode
● A Nissen fundoplication can be performed by the open method or by of gastritis as food is introduced.
laparoscopy. ● Discourage caffeinated beverages (caffeine increases gastric activity and
pepsin secretion), alcohol, and cigarette smoking (nicotine inhibits
II. Gastritis neutralization of gastric acid in the duodenum).
● Refer patient for alcohol counseling and smoking cessation when
● Gastritis is inflammation of the stomach mucosa.
appropriate.
● Acute gastritis lasts several hours to a few days and is often caused by
Promoting Fluid Balance
dietary indiscretion (eating irritating food that is highly seasoned or food
● Monitor daily intake and output for dehydration (minimal intake of 1.5
that is infected).
L/day and urine output of 30 mL/h). Infuse intravenous fluids if
○ Other causes include excessive use of aspirin and other
prescribed.
nonsteroidal anti-inflammatory drugs (NSAIDs), excessive alcohol
● Assess electrolyte values every 24 hours for fluid imbalance.
intake, bile reflux, and radiation therapy.
● Be alert for indicators of hemorrhagic gastritis (hematemesis,
○ A more severe form of acute gastritis is caused by strong acids or
tachycardia, hypotension), and notify physician.
alkali, which may cause the mucosa to become gangrenous or to
Relieving Pain
perforate.
● Instruct patient to avoid foods and beverages that may be irritating to
○ Gastritis may also be the first sign of acute systemic infection.
the gastric mucosa.
● Chronic gastritis is a prolonged inflammation of the stomach that may
● Instruct patient in the correct use of medications to relieve chronic
be caused either by benign or malignant ulcers of the stomach or by
gastritis.
bacteria such as Helicobacter pylori.
● Assess pain and attainment of comfort through use of medications and
○ Chronic gastritis may be associated with autoimmune diseases
avoidance of irritating substances
such as pernicious anemia, dietary factors such as caffeine, the use
of medications such as NSAIDs or bisphosphonates (eg, III. Peptic Ulcer
alendronate [Fosamax], risedronate [Actonel], ibandronate
[Boniva]), alcohol, smoking, or chronic reflux of pancreatic ● A peptic ulcer is an excavation formed in the mucosal wall of the
secretions and bile into the stomach. stomach, pylorus, duodenum, or esophagus. It is frequently referred to
○ Superficial ulceration may occur and can lead to hemorrhage. as a gastric, duodenal, or esophageal ulcer, depending on its location. It
Clinical Manifestations is caused by the erosion of a circumscribed area of mucous membrane.
● Acute Gastritis Peptic ulcers are more likely to be in the duodenum than in the stomach.
○ May have rapid onset of symptoms: abdominal discomfort, They tend to occur singly, but there may be several present at one time.
headache, lassitude, nausea, anorexia, vomiting, and hiccupping ● Chronic ulcers usually occur in the lesser curvature of the stomach, near
● Chronic Gastritis the pylorus. Peptic ulcer has been associated with bacterial infection,
○ May be asymptomatic. such as Helicobacter pylori. The greatest frequency is noted in people
○ Complaints of anorexia, heartburn after eating, belching, a sour between the ages of 40 and 60 years. After menopause, the incidence
taste in the mouth, or nausea and vomiting. among women is almost equal to that in men. Predisposing factors
○ Patients with chronic gastritis from vitamin deficiency usually have include family history of peptic ulcer, blood type O, chronic use of
evidence of malabsorption of vitamin B12. nonsteroidal anti-inflammatory drugs (NSAIDs), alcohol ingestion,
Assessment and Diagnostic Findings excessive smoking, and, possibly, high stress.
● Gastritis is sometimes associated with achlorhydria or hypochlorhydria ● Esophageal ulcers result from the backward flow of hydrochloric acid
(absence or low levels of hydrochloric acid) or with high acid levels. from the stomach into the esophagus. Zollinger–Ellison syndrome
● Upper gastrointestinal (GI) x-ray series, endoscopy. (gastrinoma) is suspected when a patient has several peptic ulcers or an
● Biopsy with histologic examination are performed. ulcer that is resistant to standard medical therapy. This syndrome
● Serologic testing for antibodies to the H. pylori antigen and a breath test involves extreme gastric hyperacidity (hypersecretion of gastric juice),
may be performed. duodenal ulcer, and gastrinomas (islet cell tumors). About 90% of tumors
Medical Management are found in the gastric triangle. About one third of gastrinomas are
● Acute Gastritis malignant. Diarrhea and steatorrhea (unabsorbed fat in the stool) may
○ The gastric mucosa is capable of repairing itself after an episode of be evident. These patients may have coexistent parathyroid adenomas
gastritis. As a rule, the patient recovers in about 1 day, although or hyperplasia and exhibit signs of hypercalcemia. The most frequent
the appetite may be diminished for an additional 2 or 3 days. The complaint is epigastric pain.
patient should refrain from alcohol and eating until symptoms ● The presence of H. pylori is not a risk factor. Stress ulcer (not to be
subside. Then the patient can progress to a nonirritating diet. confused with Cushing’s or Curling’s ulcers) is a term given to acute
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 10
mucosal ulceration of the duodenal or gastric area that occurs after ● Obtain a family history of ulcer disease.
physiologically stressful events, such as burns, shock, severe sepsis, and ● Assess vital signs for indicators of anemia (tachycardia, hypotension).
multiple organ trauma. Fiberoptic endoscopy within 24 hours of trauma ● Assess for blood in the stools with an occult blood test.
or injury shows shallow erosions of the stomach wall; by 72 hours, ● Palpate abdomen for localized tenderness.
multiple gastric erosions are observed, and as the stressful condition Diagnosis Nursing Diagnoses
continues, the ulcers spread. When the patient recovers, the lesions are ● Acute pain related to the effect of gastric acid secretion on damaged
reversed; this pattern is typical of stress ulceration. tissue
Clinical Manifestations ● Anxiety related to coping with an acute disease
● Symptoms of an ulcer may last days, weeks, or months and may subside ● Imbalanced nutrition related to changes in diet
only to reappear without cause. Many patients have asymptomatic ● Deficient knowledge about preventing symptoms and managing the
ulcers. condition
● Dull, gnawing pain and a burning sensation in the midepigastrium or in Collaborative Problems/Potential Complications
the back are characteristic. ● Hemorrhage: upper GI
● Pain is relieved by eating or taking alkali; once the stomach has emptied ● Perforation
or the alkali wears off, thepain returns. ● Penetration
● Sharply localized tenderness is elicited by gentle pressure on the ● Pyloric obstruction (gastric outlet obstruction)
epigastrium or slightly right of the midline. Planning and Goals
● Other symptoms include pyrosis (heartburn) and a burning sensation in ● The major goals of the patient may include relief of pain, reduced
the esophagus and stomach, which moves up to the mouth, occasionally anxiety, maintenance of nutritional requirements, knowledge about the
with sour eructation (burping). management and prevention of ulcer recurrence, and absence of
● Vomiting is rare in uncomplicated duodenal ulcer; it may or may not be complications.
preceded by nausea and usually follows a bout of severe pain and Nursing Interventions
bloating; it is relieved by ejection of the acid gastric contents. ● Relieving Pain and Improving Nutrition
● Constipation or diarrhea may result from diet and medications. ○ Administer prescribed medications.
● Bleeding (15% of patients with gastric ulcers) and tarry stools may occur; ○ Avoid aspirin, which is an anticoagulant, and foods and beverages
a small portion of patients who bleed from an acute ulcer have only very that contain acid-enhancing caffeine (colas, tea, coffee, chocolate),
mild symptoms or none at all. along with decaffeinated coffee.
Assessment and Diagnostic Methods ○ Encourage patient to eat regularly spaced meals in a relaxed
● Physical examination (epigastric tenderness, abdominal distention). atmosphere; obtain regular weights and encourage dietary
● Endoscopy (preferred, but upper gastrointestinal [GI] barium study may modifications.
be done). ○ Encourage relaxation techniques.
● Diagnostic tests include analysis of stool specimens for occult blood, ● Reducing Anxiety
gastric secretory studies, and biopsy and histology with culture to detect ○ Assess what patient wants to know about the disease, and evaluate
H. pylori (serologic testing, stool antigen tests, or a breath test may also level of anxiety; encourage patient to express fears openly and
detect H. pylori) without criticism.
Medical Management ○ Explain diagnostic tests and administering medications on
● The goals of treatment are to eradicate H. pylori and manage gastric schedule.
acidity. ○ Interact in a relaxing manner, help in identifying stressors, and
Pharmacologic Therapy explain effective coping techniques and relaxation methods.
● Antibiotics combined with proton pump inhibitors and bismuth salts to ○ Encourage family to participate in care, and give emotional
suppress H. pylori. support.
● H2-receptor antagonists (in high doses in patients with Zollinger–Ellison ● Monitoring and Managing Complications
syndrome) to decrease stomach acid secretion; maintenance doses of ○ If hemorrhage is a concern
H2-receptor antagonists are usually recommended for 1 year. Proton ■ Assess for faintness or dizziness and nausea, before or with
pump inhibitors may also be prescribed. bleeding; test stool for occult or gross blood; monitor vital
● Cytoprotective agents (protect mucosal cells from acid or NSAIDs). signs frequently (tachycardia, hypotension, and tachypnea).
● Antacids in combination with cimetidine (Tagamet) or ranitidine (Zantac) ■ Insert an indwelling urinary catheter and monitor intake and
for treatment of stress ulcer and for prophylactic use. Lifestyle Changes output; insert and maintain an IV line for infusing fluid and
● Stress reduction and rest are priority interventions. The patient needs to blood.
identify situations that are stressful or exhausting (eg, rushed lifestyle ■ Monitor laboratory values (hemoglobin and hematocrit).
and irregular schedules) and implement changes, such as establishing ■ Insert and maintain a nasogastric tube and monitor drainage;
regular rest periods during the day in the acute phase of the disease. provide lavage as ordered.
Biofeedback, hypnosis, behavior modification, massage, or acupuncture ■ Monitor oxygen saturation and administering oxygen
may also be useful. therapy.
● Smoking cessation is strongly encouraged because smoking raises ■ Place the patient in the recumbent position with the legs
duodenal acidity and significantly inhibits ulcer repair. Support groups elevated to prevent hypotension, or place the patient on the
may be helpful. left side to prevent aspiration from vomiting.
● Dietary modification may be helpful. Patients should eat whatever ■ Treat hypovolemic shock as indicated.
agrees with them; small, frequent meals are not necessary if antacids or ○ If perforation and penetration are concerns
histamine blockers are part of therapy. Oversecretion and hypermotility ■ Note and report symptoms of penetration (back and
of the GI tract can be minimized by avoiding extremes of temperature epigastric pain not relieved by medications that were
and overstimulation by meat extracts. Alcohol and caffeinated beverages effective in the past).
such as coffee (including decaffeinated coffee, which stimulates acid ■ Note and report symptoms of perforation (sudden abdominal
secretion) should be avoided. Diets rich in milk and cream should be pain, referred pain to shoulders, vomiting and collapse,
avoided also because they are potent acid stimulators. The patient is extremely tender and rigid abdomen, hypotension and
encouraged to eat three regular meals a day tachycardia, or other signs of shock).
Surgical Management
● With the advent of H2-receptor antagonists, surgical intervention is less VII. Health History and Clinical Manifestations
common.
● If recommended, surgery is usually for intractable ulcers (particularly A. SUBJECTIVE DATA
with Zollinger–Ellison syndrome), life threatening hemorrhage,
perforation, or obstruction. Surgical procedures include vagotomy, 1. GENERAL DATA
vagotomy with pyloroplasty, or Billroth I or II. A. presence of dental prosthesis, comfort of usage
NURSING PROCESS THE PATIENT WITH PEPTIC ULCER B. difficulty eating or digesting food
Assessment C. nausea or vomiting
● Assess pain and methods used to relieve it; take a thorough history, D. weight loss
including a 72-hour food intake history. E. pain
● If patient has vomited, determine whether emesis is bright red or coffee
ground in appearance. This helps identify source of the blood.
● Ask patient about usual food habits, alcohol, smoking, medication use
(NSAIDs), and level of tension or nervousness.
● Ask how patient expresses anger (especially at work and with family),
and determine whether patient is experiencing occupational stress or
family problems.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 11
● The nurse assesses bowel sounds in all four quadrants using the
diaphragm of the stethoscope; the high-pitched and gurgling sounds can
be heard best in this manner.
● It is important to document the frequency of the sounds, using the terms
2. SPECIFIC DATA normal (sounds heard about every 5 to 20 seconds), hypoactive (one or
A. situations or events that effect symptoms two sounds in 2 minutes), hyperactive (5 to 6 sounds heard in less than
B. onset, possible cause, location, duration, character 30 seconds), or absent (no sounds in 3 to 5 minutes).
of symptoms ● The nurse notes tympani or dullness during percussion. Use of light
C. relationship of specific foods, smoking or alcohol to severity of palpation is appropriate for identifying areas of tenderness or swelling;
symptoms the nurse may use deep palpation to identify masses in any of the four
D. how the symptoms was managed before quadrants.
seeking medical help ● The final part of the examination is inspection of the anal and perineal
3. NORMAL PATTERN OF BOWEL ELIMINATION area. The nurse should inspect and palpate areas of excoriation or rash,
A. frequency and character of stool fissures or fistula openings, or external hemorrhoids.
B. use of laxatives, enemas
4. RECENT CHANGES IN NORMAL PATTERNS
A. changes in character of stool (constipation, diarrhea, or alternating
constipation and diarrhea)
B. changes in color of stool
a. melena
b. hematochezia
C. drugs /medications being taken
D. measures taken to relieve symptoms
INDIGESTION
● Indigestion can result from disturbed nervous system control of the IX. Diagnostic Evaluation
stomach or from a disorder in the GI tract or elsewhere in the body.
● Common blood tests include complete blood count (CBC),
INTESTINAL GAS carcinoembryonic antigen (CEA), liver function tests, serum cholesterol,
and triglycerides.
● The accumulation of gas in the GI tract may result in belching or ● General nursing interventions for the patient who is having GI diagnostic
flatulence. assessment include the following:
NAUSEA AND VOMITING ● Providing general information about a healthy diet and the nutritional
factors that can cause GI disturbances; after a diagnosis has been
● Vomiting is usually preceded by nausea, which can be triggered by odors, confirmed, the nurse provides information about specific nutrients that
activity, or food intake. should be included in the diet.
● When vomiting occurs soon after hemorrhage, the emesis is bright red. ● Providing needed information about the test and the activities required
● If blood has been retained in the stomach, it takes on a coffee-ground of the patient
appearance because of the action of the digestive enzymes. ● Providing instructions about post procedure care and activity restrictions
● Alleviating anxiety
BOWEL HABITS AND STOOL CHARACTERISTIC ● Helping the patient cope with discomfort
● Encouraging family members or others to offer emotional support to the
● Diarrhea commonly occurs when the contents move so rapidly through patient during the diagnostic testing
the intestine and colon that there is inadequate time for the GI secretions ● Assessing for adequate hydration before, during, and immediately after
to be absorbed. the procedure
● Constipation may be associated with anal discomfort and rectal
bleeding. STOOL TEST
● Blood in the stool can present in various ways and must be investigated.
● Blood entering the lower portion of the GI tract or passing rapidly
through it will appear bright or dark red. ● Basic examination of the stool includes:
● Lower rectal or anal bleeding is suspected if there is streaking of ○ inspecting the specimen for consistency
blood on the surface of the stool. and color and testing for occult blood
● Other common abnormalities in stool characteristics include the ○ tests for fecal urobilinogen, fat, nitrogen,
following: ○ parasites, pathogens, food residues, and
○ Bulky, greasy, foamy stools that are foul in odor; stool color is gray, other substances
with a silvery sheen ● The most widely used occult blood test is the Hematest. False-positive
○ Light gray or clay-colored stool, caused by the absence of urobilin results may occur if the patient has eaten rare meat, liver, poultry,
○ Stool with mucus threads or pus that may be visible on gross turnips, broccoli, cauliflower, melons, salmon, sardines, or horseradish
inspection of the stool within 7 days before testing.
○ Small, dry, rock-hard masses called scybala; sometimes streaked ● Medications that can cause gastric irritation, such as aspirin, ibuprofen,
with blood from rectal trauma as they pass through the rectum indomethacin, colchicine, corticosteroids, cancer chemotherapeutic
○ Loose, watery stool that may or may not be streaked with blood agents, and anticoagulants, may also cause false-positive results.
VIII. Physical Assessment BREATH TEST
● The patient lies supine with knees flexed slightly for inspection, ● The hydrogen breath test was developed to evaluate carbohydrate
auscultation, palpation, and percussion of the abdomen. absorption. It also is used to aid in the diagnosis of bacterial overgrowth
● The nurse performs inspection first, noting skin changes and scars from in the intestine and short bowel syndrome.
previous surgery. It also is important to note the contour and symmetry ● Urea breath tests detect the presence of Helicobacter pylori. The patient
of the abdomen, to identify any localized bulging, distention, or takes a capsule of carbon labeled urea and then provides a breath sample
peristaltic waves. 10 to 20 minutes later.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 12
● The patient is instructed to avoid antibiotics or loperamide for 1 month Contraindications For Barium Enema
before the test; sucralfate and omeprazole for 1 week before the test; ● patient has active inflammatory disease of the colon
and cimetidine, famotidine, ranitidine, and nizatidine for 24 hours before ● patients with signs of perforation or obstruction
urea breath testing. ● active GI bleeding may prohibit the use of laxatives and enemas
● In patients with perforation or obstruction; a water-soluble contrast
ABDOMINAL ULTRASONOGRAPHY study may be performed in these situations.
After the Procedure
● During abdominal ultrasonography, an image of the abdominal organs ● The nurse administers an enema or laxative after these
and structures is produced on the oscilloscope. This procedure is ● tests to facilitate barium removal.
generally used to indicate the size and configuration of abdominal ● Increasing fluid intake also will assist in eliminating the barium.
structures. ● As with any barium study, the nurse monitors the patient for complete
● Endoscopic ultrasonography (EUS) is a specialized enteroscopic elimination of the barium.
procedure that aids in the diagnosis of GI disorders by providing direct
imaging of a target area. A small high-frequency ultrasonic transducer is COMPUTED TOMOGRAPHY
mounted at the tip of the fiberoptic scope so that a transintestinal study
can be completed.
● CT provides cross-sectional images of abdominal organs and
X. Nursing Interventions structures.
● Multiple x-ray images are taken from many different angles, digitized in
● The patient fasts for 8 to 12 hours before the test to decrease the amount the computer, reconstructed, and then viewed on a computer monitor.
of gas in the bowel. ● Indications for abdominal CT scanning are diseases of the liver, spleen,
● If gallbladder studies are being performed, the patient should eat a fat- kidney, pancreas, and pelvic organs.
free meal the evening before the test. ● CT is a valuable tool for detecting and localizing many inflammatory
● If barium studies are to be performed, the nurse should make sure they conditions in the colon, such as appendicitis, diverticulitis, regional
are scheduled after this test; otherwise, the barium will interfere with enteritis, and ulcerative colitis.
the transmission of the sound waves. Nursing Interventions
● The patient should not eat or drink for 6 to 8 hours before the test.
DNA TESTING ● The practitioner may prescribe an intravenous or oral contrast agent.
Therefore, the nurse should question the patient about contrast dye
● DNA testing allows practitioners to prevent (or minimize) disease, by allergies.
intervening before its onset, and to improve therapy. ● If barium studies are to be performed, it is important to schedule them
● Persons at risk for colon cancer often are targeted for DNA testing after CT scanning, so as not to interfere with imaging.
because it can provide a head start on this preventable cancer.
MAGNETIC RESONANCE IMAGING
IMAGING STUDIES
● MRI is used in gastroenterology supplement ultrasonography and CT
● Imaging studies include: scanning.
○ x-ray and contrast studies ● It is a noninvasive technique that uses magnetic fields and radio waves
○ computed tomography (CT) scans to produce an image of the area being studied.
○ magnetic resonance imaging (MRI) ● It is useful in evaluating abdominal soft tissues as well as blood vessels,
○ and scintigraphy (radionuclide imaging) abscesses, fistulas, neoplasms, and other sources of bleeding.
Contraindications For MRI
UPPER GI TRACT STUDY ● patients with permanent pacemakers, artificial heart valves and
defibrillators, implanted insulin pumps, or implanted transcutaneous
● X-rays can delineate the entire GI tract after the introduction of a electrical nerve stimulation devices
contrast agent. ● patients with internal metal devices (e.g., aneurysm clips) or intraocular
● Variations of the upper GI study include double-contrast studies and metallic fragments
enteroclysis. Nursing Interventions
● The double-contrast method of examining the upper GI tract involves ● The patient should not eat or drink for 6 to 8 hours before the test.
administration of a thick barium suspension to outline the stomach and ● Patient must remove all jewelry and other metals.
esophageal wall, after which tablets that release carbon dioxide in the ● It is important to warn patients that the close-fitting scanners used in
presence of water are given. many MRI facilities may induce feelings of claustrophobia and that the
Before the Procedure machine will make a knocking sound during the procedure.
● maintain a low-residue diet several days before the test ● Open MRIs that are less close-fitting eliminate the claustrophobia that
● receive nothing by mouth after midnight before the test many patients experience.
● physician may prescribe a laxative to clean out the intestinal tract
SCINTIGRAPHY
● discourage the patient from smoking on the morning before the
examination ● Scintigraphy relies on the use of radioactive isotopes (i.e., technetium,
● withhold all medications as ordered by the physician iodine, and indium) to reveal displaced anatomic structures, changes in
After the Procedure organ size, and the presence of neoplasms or other focal lesions, such
● Follow-up care is needed after any of the upper GI procedures to ensure as cysts or abscesses.
that the patient has completely eliminated the ingested barium. ● Scintigraphic scanning is also used to measure the
● Fluids must be increased to facilitate evacuation of stool and barium. ● uptake of tagged red blood cells and leukocytes.
● The nurse monitors the patient’s stools until they return to their normal ● A sample of blood is removed, mixed with a radioactive substance, and
color. reinjected into the patient.
● A laxative or enema may be needed as ordered by the physician. ● Abnormal concentrations of blood cells are then detected at 24- and 48-
hour intervals.
LOWER GI TRACT STUDY
GASTROINTESTINAL MOTILITY STUDIES
● When barium is instilled rectally to visualize the lower GI tract, the
● Radionuclide testing also is used to assess gastric emptying and colonic
procedure is called a barium enema.
transit time.
● The purpose of a barium enema is to detect the presence of
● For gastric emptying studies, the liquid and solid components of a meal
polyps, tumors, and other lesions of the large intestine
are tagged with radionuclide markers.
and to demonstrate any abnormal anatomy or malfunction
● After the patient ingests the meal, the patient is positioned under a
of the bowel.
scintiscanner, which measures the rate of passage of the radioactive
● The procedure usually takes about 15 to 30 minutes, during which time
substance out of the stomach.
x-ray images are taken.
● Abdominal x-rays are taken every 24 hours until all markers are passed.
Before the Procedure
This process usually takes 4 to 5 days.
● a low-residue diet 1 to 2 days before the test
● a clear liquid diet and a laxative the evening before ENDOSCOPIC PROCEDURES
● nothing by mouth after midnight
● cleansing enemas until returns are clear the following morning ● Endoscopic procedures in GI tract assessment include:
● The nurse should make sure that barium enemas are scheduled before ○ fibroscopy / esophagogastroduodenoscopy
any upper GI studies. ○ anoscopy
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 13
○ proctoscopy
○ sigmoidoscopy
○ colonoscopy
○ small-bowel enteroscopy
○ endoscopy through ostomy
UPPER GI FIBROSCOPY/ ESOPHAGOGASTRODUODENOSCOPY
● Fibroscopy of the upper GI tract allows direct visualization of the
esophageal, gastric, and duodenal mucosa through a lighted endoscope
(gastroscope).
● Esophagogastroduodenoscopy (EGD), is valuable when esophageal,
gastric, or duodenal abnormalities or inflammatory, neoplastic, or
infectious processes are suspected.
● This procedure also can be used to evaluate esophageal and gastric
Nursing Interventions
motility and to collect secretions and tissue specimens.
● These examinations require only limited bowel preparation, including a
warm tap water or Fleet’s enema until returns are clear.
● During the procedure, the nurse monitors vital signs, skin color and
temperature, pain tolerance, and vagal response.
● After the procedure, the nurse monitors the patient for rectal bleeding
and signs of intestinal perforation (ie, fever, rectal drainage, abdominal
distention, and pain).
ANOSCOPY, PROCTOSCOPY, AND SIGMOIDOSCOPY
● Fiberoptic colonoscope are larger in diameter and longer
● It is most frequently used for cancer screening and for surveillance in
patients with previous colon cancer or polyps.
● Tissue biopsies can be obtained as needed, and polyps can be removed
and evaluated.
Before the Procedure
● Therapeutically, the procedure can be used to remove
● The patient should not eat or drink for 6 to 12 hours before the
● all visible polyps, areas of bleeding or stricture.
examination.
● Help the patient spray or gargle with a local anesthetic, and administer ENDOSCOPIC PROCEDURES
midazolam (Versed) intravenously just before the scope is introduced.
● The nurse also may administer atropine to reduce secretions, and may ● Colonoscopy is performed while the patient is lying on the left side with
give glucagon, if needed and prescribed, to relax smooth muscle. the legs drawn up toward the chest.
● The nurse positions the patient on the left side to facilitate saliva ● The procedure usually takes about 1 hour. Discomfort may result from
drainage and to provide easy access for the endoscope. instillation of air to expand the colon or from insertion and moving of the
After the Procedure scope.
● After the procedure, the nurse instructs the patient not to eat or drink ● Potential complications of colonoscopy include cardiac dysrhythmias and
until the gag reflex returns (in 1 to 2 hours), to prevent aspiration of food respiratory depression resulting from the medications administered,
or fluids into the lungs. vasovagal reactions, and circulatory overload or hypotension resulting
● The nurse places the patient in the Simms position until he or she is from overhydration or underhydration during bowel preparation.
awake and then places the patient in the semi-Fowler’s position until
ready for discharge.
● After gastroscopy, assessment by the nurse includes observing for signs
of perforation, such as pain, bleeding, unusual difficulty swallowing, and
an elevated temperature.
● The nurse monitors the pulse and blood pressure for changes that can
occur with sedation.
● After the patient’s gag reflex has returned, the nurse can offer lozenges,
saline gargle, and oral analgesics to relieve minor throat discomfort.
● Patients who were sedated for the procedure must stay on bed rest until
fully alert.
ANOSCOPY, PROCTOSCOPY, AND SIGMOIDOSCOPY
● The lower portion of the colon also can be viewed directly to evaluate
rectal bleeding, acute or chronic diarrhea, or change in bowel patterns Before the Procedure
and to observe for ulceration, fissures, abscesses, tumors, polyps, or ● Patient should limit the intake of liquids for 24 to 72 hours before the
other pathologic processes. examination.
● The anoscope is a rigid scope that is used to examine the anus and lower ● The physician may prescribe a laxative for two nights before the
rectum. examination and a Fleet’s or saline enema until the return runs clear the
● Proctoscopes and sigmoidoscopes are rigid scopes that are used to morning of the test.
inspect the rectum and the sigmoid colon. ● Polyethylene glycol electrolyte lavage solutions (Golytely, Colyte,
NuLytely) are used as lavages for effective cleansing of the bowel.
ENDOSCOPIC PROCEDURES ● The patient maintains a clear liquid diet starting at noon the day before
● For rigid scope procedures, the patient assumes the knee-chest position the procedure. Then the patient ingests lavage solutions orally at
at the edge of the bed or the examining table. With the back inclined at intervals over 3 to 4 hours.
about a 45- degree angle, the patient is properly positioned for the Nursing Interventions
introduction of an anoscope, proctoscope, or sigmoidoscope. ● Instructing the patient not to take routine medications when the lavage
● For flexible scope procedures, the patient assumes a comfortable solution is ingested; the medications will not be digested and therefore
position on the left side with the right leg bent and placed anteriorly. will be ineffective
● Biopsy is performed with small biting forceps introduced through the ● Advising the diabetic patient to consult with his or her physician about
endoscope; one or more small pieces of tissue may be removed. medication adjustment to prevent hyperglycemia or hypoglycemia
resulting from dietary modifications required in preparation for the test
● Instructing all patients, especially the elderly, to maintain adequate fluid,
electrolyte, and caloric intake while undergoing bowel cleansing
During the Procedure
● Informed consent is obtained before the test.
● Before the examination, the nurse may administer intravenously an
opioid analgesic or a sedative (eg, midazolam) to provide moderate
sedation and relieve anxiety during the procedure.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 14
● Glucagon may be used, if needed, to relax the colonic musculature and ● Analysis of the gastric juice yields information about the secretory
to reduce spasm during the test. activity of the gastric mucosa and the presence or degree of gastric
● Elderly or debilitated patients may require a reduced dosage of these retention in patients thought to have pyloric or duodenal obstruction.
medications to decrease the risks of oversedation and cardiopulmonary ● Important diagnostic information to be gained from gastric analysis
complications. includes the ability of the mucosa to secrete HCl.
● The nurse monitors for changes in oxygen saturation, vital signs, color Nursing Interventions
and temperature of the skin, level of consciousness, abdominal ● The patient is kept NPO for 8 to 12 hours before the procedure
distention, vagal response, and pain intensity. ● any medications that affect gastric secretion are withheld for 24 to 48
Nursing Interventions hours before the test
● The nurse monitors for changes in oxygen saturation, vital signs, color ● smoking is not allowed on the morning before the test, because it
and temperature of the skin, level of consciousness, abdominal increases gastric secretions
distention, vagal response, and pain intensity.
After the Procedure GASTRIC SIMULATION TEST
● Patients who were sedated are maintained on bed rest
● The gastric acid stimulation test usually is performed in conjunction with
● until fully alert.
gastric analysis.
● Some will have abdominal cramps caused by increased peristalsis
● Histamine is administered subcutaneously to stimulate gastric
stimulated by the air insufflated into the bowel during the procedure.
secretions. It is important to inform the patient that this injection may
● The nurse observes the patient for signs and symptoms of bowel
produce a flushed feeling.
perforation (eg, rectal bleeding, abdominal pain or distention, fever,
● Gastric specimens are collected after the injection every 15 minutes for
focal peritoneal signs).
1 hour and are labeled to indicate the time of specimen collection after
● If midazolam was used, the nurse explains its amnesic effects.
histamine injection.
Nursing Interventions
● The volume and pH of the specimen are measured.
● It is important to provide written instructions, because the patient may
Nursing Interventions
be unable to recall verbal information.
● Inform the patient that this injection may produce a flushed
● If the procedure is performed on an outpatient basis, someone must
feeling.
accompany and transport the patient home.
● The nurse monitors blood pressure and pulse frequently to detect
● After a therapeutic procedure, the nurse instructs the patient to report
hypotension.
any bleeding to the physician.
● Side effects of the electrolyte solutions include: LAPAROSCOPY
○ nausea
○ bloating ● This procedure is performed through a small incision in the abdominal
○ cramps or abdominal fullness wall. Special fiberoptic laparoscopes allow direct visualization of the
○ fluid and electrolyte imbalance organs and structures within the abdomen, permitting visualization and
○ hypothermia (patients are often told to drink the preparation as identification of any growths, anomalies, and inflammatory processes.
cold as possible to make it more palatable) ● Biopsy samples can be taken from the structures and organs as
Contraindications necessary.
● Patients with intestinal obstruction or inflammatory bowel disease. ● This procedure can be used to evaluate peritoneal disease, chronic
● Implantable defibrillators and pacemakers are at high risk for malfunction abdominal pain, abdominal masses, and gallbladder and liver disease.
if electrosurgical procedures (ie,polypectomy) are performed in
conjunction with colonoscopy XI. Terminologies
● COlonoscopy cannot be performed if there is a suspected or documented
● Dyspepsia: Difficult digestion
colon perforation, acute severe diverticulitis, or fulminant colitis.
● Emesis (vomiting): Stomach contents expelled through the mouth
● Therapeutic colonoscopy may be contraindicated in patients with
● Eructation: Act of belching or raising gas from stomach
coagulopathies and in those receiving anticoagulation therapy, because
● Gastric ulcer: Lesion on wall of stomach; also known as peptic ulcer
of the high risk for excessive bleeding during and after the procedure.
● Gastritis: Inflammation of the stomach
● Nonsteroidal anti-inflammatory agents (NSAIDs), aspirin, ticlopidine, and
● Gastrodynia: Pain in the stomach
pentoxifylline must be discontinued before the test and for 2 weeks after
● Hematemesis: Vomiting of blood
the procedure. Patients taking coumadin or heparin must consult the
● Hiatal hernia: Protrusion of part of the stomach through the esophageal
physician for specific instructions.
opening into diaphragm
● Those with prosthetic heart valves or a history of endocarditis require
● Hyperemesis: Excessive vomiting
prophylactic antibiotics before the procedure.
● Nasogastric: Pertaining to nose and stomach
● Nausea: Urge to vomit
● Regurgitation: Return of solids and fluids to mouth from stomach
ENDOSCOPY THROUGH OSTOMY ● Ulcer: Sore or lesion of mucous membrane or skin
● The liver, pancreas, and gallbladder all experience their own specific
● Endoscopy using a flexible endoscope through an ostomy stoma is useful conditions, the most common of which is good, old-fashioned, often-
for visualizing a segment of the small or large intestine. painful gallstones.
● It may be indicated to evaluate an anastomosis, to screen for recurrent ● Calculus (plural is calculi): Stones
disease, or to visualize and treat bleeding in a segment of the bowel. ● Cholelithiasis: Condition of having gallstones
● Duodenal ulcer: Erosion or ulceration in the lining of the duodenum (first
MANOMETRY AND ELECTROPHYSIOLOGIC STUDIES portion of the small intestine)
● Gallstones: Hard collections of bile that form in gallbladder and bile
● The manometry test measures changes in intraluminal pressures and the
ducts
coordination of muscle activity in the GI tract. The pressures can be
● Hepatomegaly: Enlargement of liver
recorded manually, on a physiograph, or on a computer.
● Hepatoma: Tumor of liver
● Electrogastrography, an electrophysiologic study, is performed to assess
gastric motility disturbances. Electrodes are placed over the abdomen, XII. PRACTICE
and gastric electrical activity is recorded for up to 24 hours.
Electrogastrography can be useful in detecting motor or nerve ● 1. As a student nurse assigned at the emergency room, you are in charge
dysfunction in the stomach. of a 24-year-old male patient who was admitted for acute abdominal
pain. He is being scheduled for tests this afternoon. What laboratory
DEFECOGRAPHY tests would you expect to be ordered? What preparation is needed for
these tests? What preprocedure education is needed?
● Defecography measures anorectal function. Very thick barium paste is
● 2. A 58-year-old patient assigned to you this morning has just left to go
instilled into the rectum, and then fluoroscopy is performed to assess the
to the Endoscopy Suite, where she will undergo a colonoscopy. You
function of the rectum and anal sphincter while the patient attempts to
know that your patient will receive moderate sedation during the
expel the barium.
procedure and that she will be returned to your care once she is fully
● Electromyographic (EMG) studies can supplement anorectal manometry
alert. What should you anticipate in the course of recovery for your
to measure the integrity and function of the anal sphincters in an effort
patient after the colonoscopy? What medications might be used for the
to treat functional bowel incontinence and constipation.
moderate sedation, and what effects of those medications would you
GASTRIC ANALYSIS expect to see during the recovery period? Describe the potential
complications that could occur and what you will monitor. What are the
goals for care during this period?
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 15
blood clotting factors, specific transport proteins, and most of
WEEK 3: DISORDERS OF THE LIVER, PANCREAS, AND the plasma lipoproteins.
GALLBLADDER ● Fat Metabolism
○ The liver is also active in fat metabolism. Fatty acids can be
broken down for the production of energy and ketone bodies
LIVER (acetoacetic acid, beta-hydroxybutyric acid, and acetone).
Ketone bodies are small compounds hat can enter the
Liver function is complex, and liver dysfunction affects all body systems. For bloodstream and provide a source of energy for muscles and
this reason, the nurse must understand how the liver functions and must have other tissues.
expert clinical assessment and management skills to care for patients ● Vitamin and Iron Storage
undergoing complex diagnostic and treatment procedures. The nurse also must ○ Vitamins A, B, and D and several of the B-complex vitamins are
understand technologic advances in the management of liver disorders. Liver stored in large amounts in the liver.
disorders are common and may result from a virus, exposure to toxic ○ Certain substances, such as iron and copper, are also stored in
substances such as alcohol, or tumors. the liver.
ASSESSMENT OF THE LIVER ● Bile Formation
○ Bile is continuously formed by the hepatocytes and collected in
the canaliculi and bile ducts. It is composed mainly of water and
ANATOMIC & PHYSIOLOGIC OVERVIEW electrolytes such as sodium, potassium, calcium, chloride, and
bicarbonate, and it also contains significant amounts of lecithin,
fatty acids, cholesterol, bilirubin, and bile salts. Bile is collected
and stored in the gallbladder and is emptied into the intestine
when needed for digestion.
● Bilirubin Excretion
○ Bilirubin is a pigment derived from the breakdown of
hemoglobin by cells of the reticuloendothelial system, including
the Kupffer cells of the liver. Hepatocytes remove bilirubin from
the blood and chemically modify it through conjugation to
glucuronic acid, which makes the bilirubin more soluble in
aqueous solutions.
● Drug Metabolism
○ The liver metabolizes many medications, such as barbiturates,
opioids, sedatives, anesthetics, and amphetamines.
○ Metabolism generally results in drug inactivation, although
activation may also occur. One of the important pathways for
medication metabolism involves conjugation (binding of the
medication with a variety of compounds, such as glucuronic acid
or acetic acid, to form more soluble substances.
I. HEPATITIS. VIRAL: TYPES A. B, C, D. E, & G
● The liver, the largest gland of the body, can be considered a chemical
factory that manufactures, stores, alters, and excretes a large number of
substances involved in metabolism. The location of the liver is essential
in this function because it receives nutrient-rich blood directly from the HEPATITIS A
gastrointestinal (GI) tract and then either stores or transforms these ● Hepatitis A is caused by an RNA virus of the genus Enterovirus. This form
nutrients into chemicals that are used elsewhere in the body for of hepatitis is transmitted primarily through the fecal-oral route, by the
metabolic needs. The liver is especially important in the regulation of ingestion of food or liquids infected by the virus.
glucose and protein metabolism. ● The virus is found in the stool of infected patients before the onset of
● The liver manufactures and secretes bile, which has a major role in the symptoms and during the first few days of illness. The incubation period
digestion and absorption of fats in the GI tract. The liver removes waste is estimated to be 2 to 6 weeks, with a mean of approximately 4 weeks.
products from the bloodstream and secretes them into the bile. The bile ● The course of illness may last 4 to 8 weeks. The virus is present
produced by the liver is stored temporarily in the gallbladder until it is only briefly in the serum; by the time jaundice appears, the patient is
needed for digestion, at which time the gallbladder empties and bile likely to be noninfectious. A person who is immune to hepatitis A may
enters the intestine (Fig. 39-1). contract other forms of hepatitis. Recovery from hepatitis A is usual; it
rarely progresses to acute liver necrosis and fulminant hepatitis. No
ANATOMY OF THE LIVER carrier state exists, and no chronic hepatitis is associated with hepatitis
● The liver is a large, highly vascular organ located behind the ribs in the A.
upper right portion of the abdominal cavity. It weighs between 1200 and ● ssRNA virus transmitted via fecal-oral route.
1500 g and is divided into four lobes. A thin layer of connective tissue ● Poor hygiene or contaminated food and shellfish
surrounds each lobe, extending into the lobe itself and dividing the liver ● increase risk of transmission
mass into small, functional units called lobules. The circulation of the ● Incubation period: 15 – 45 days
blood into and out of the liver is of major importance to liver function. CLINICAL MANIFESTATIONS
The blood that perfuses the liver comes from two sources. ● Many patients are anicteric (without jaundice) and symptomless.
Approximately 80% of the blood supply comes from the portal vein, ● When symptoms appear, they are of a mild, flu like, upper respiratory
which drains the GI tract and is rich in nutrients but lacks oxygen. infection, with low-grade fever.
● AnorexIa Is an early symptom and is often severe
FUNCTIONS OF THE LIVER ● Later, jaundice and dark urine may be apparent.
● Glucose Metabolism
○ The liver plays a major role in the metabolism of glucose
and the regulation of blood glucose concentration. After a
meal, glucose is taken up from the portal venous blood by
the liver and converted into glycogen, which is stored in the
hepatocytes.
● Ammonia Conversion
○ Use of amino acids from protein for gluconeogenesis
results in the formation of ammonia as a byproduct. The
liver converts this metabolically generated ammonia into ● Indigestion is present in varying degrees.
urea. Ammonia produced by bacteria in the intestines is ● Liver and spleen are often moderately enlarged for a few days after onset.
also removed from portal blood for urea synthesis. ● Patient may have an aversion to cigarette smoke and strong odors;
symptoms tend to clear when jaundice reaches its peak.
● Protein Metabolism ● Symptoms may be mild in children; in adults, they may be more severe,
○ The liver also plays an important role in protein metabolism. It and the course of the disease prolonged.
synthesizes almost all of the plasma proteins (except gamma- ASSESSMENT & DIAGNOSTIC METHODS
globulin), including albumin, alpha-globulins and beta-globulins, ● Stool analysis for hepatitis A antigen
● Serum hepatitis A virus antibodies; immunoglobulin
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 16
PREVENTION ● Convalescence may be prolonged and recovery may take 3 to 4 months;
● Scrupulous hand washing, safe water supply, proper control of sewage encourage gradual activity after complete clearing of jaundice.
disposal. ● Identifies psychosocial issues and concerns, particularly the effects of
● Hepatitis vaccine. separation from family and friends if the patient is hospitalized; if not
● Administration of immune globulin, if not previously vaccinated, to hospitalized, the patient will be unable to work and must avoid sexual
prevent hepatitis A if given within 2 weeks of exposure. contact
● Immune globulin is recommended for household members and for those ● Include family in planning to help reduce their fears and anxieties about
who are in sexual contact with people with hepatitis A. the spread of the disease.
● Preexposure prophylaxis is recommended for those traveling to ● Educate patient and family in home care and convalescence.
developing countries or settings with poor or uncertain sanitation ● Instruct patient and family to provide adequate rest and nutrition.
conditions who do not have sufficient time to acquire protection by ● Inform family and intimate friends about risks of contracting hepatitis B
administration of hepatitis A vaccine ● Arrange for family and intimate friends to receive hepatitis B vaccine or
MANAGEMENT hepatitis B immune globulin as prescribed.
● Bed rest during the acute stage; encourage a nutritious diet. ● Caution patient to avoid drinking alcohol and eating raw shellfish.
● Give small, frequent feedings supplemented by IV glucose if necessary ● Inform family that follow-up home visits by home care nurse are indicated
during period of anorexia. to assess progress and understanding, reinforce teaching, and answer
● Promote gradual but progressive ambulation to hasten recovery. Patient questions.
is usually managed at home unless symptoms are severe ● Encourage patient to use strategies to prevent exchange of body fluids,
● Assist patient and family to cope with the temporary disability and fatigue such as avoiding sexual intercourse or using condoms.
that are common problems in hepatitis ● Emphasize importance of keeping follow-up appointments and
● Teach patient and family the indications to seek additional health care if participating in other health promotion activities and recommended
the symptoms persist or worsen. health screenings.
● Instruct patient and family regarding diet, rest, follow-up blood work,
avoidance of alcohol, and sanitation and hygiene measures (hand HEPATITIS C
washing) to prevent spread of disease to other family members.
● A significant portion of cases of viral hepatitis are not A, B, or D; they are
● Teach patient and family about reducing risk for contracting hepatitis A:
classified as hepatitis C. It is the primary form of hepatitis associated with
good personal hygiene with careful hand washing; environmental
parenteral means (sharing contaminated needles, needlesticks or injuries
sanitation with safe food and water supply and sewage disposal.
to health care workers, blood transfusions) or sexual contact.
HEPATITIS B ● The incubation period is variable and may range from 15 to 160 days. The
clinical course of hepatitis C is similar to that of hepatitis B; symptoms are
● Hepatitis B virus (HBV) is a DNA virus transmitted primarily through blood. usually mild.
The virus has been found in saliva, semen, and vaginal secretions and can ● A chronic carrier state occurs frequently.
be transmitted through mucous membranes and breaks in the skin. ● There is an increased risk for cirrhosis and liver cancer after hepatitis C. A
Hepatitis B has a long incubation period (1 to 6 months). It replicates in combination therapy using ribavirin (Rebetol) and interferon (Intron-A) is
the liver and remains in the serum for long periods, allowing transmission effective for treating patients with hepatitis C and in treating relapses.
of the virus. Those at risk include all health care workers, patients in ● ssRNA virus generally transmitted predominantly by blood products
hemodialysis and oncology units, sexually active homosexual and bisexual ● Currently the most common hepatitis among IV drug abusers and in
men, and IV drug users. About 10% of patients progress to a carrier state prisons
or develop chronic hepatitis. ● Before 1990 it accounted for 90% of transfusion hepatitis
● Hepatitis B remains a major worldwide cause of cirrhosis and ● Incubation: 2 weeks - 6 months high risk of progression to chronic form
hepatocellular carcinoma. (70 – 80%)
● DNA virus, identified in all body fluids: blood, saliva, synovial fluid, breast ● associated with extrahepatic manifestations
milk, ascites, cerebral spinal fluid, etc. ● commonly: mixed cryoglobulinemia and polyarteritis nodosa
● Transmitted by blood and body fluids (saliva, semen, vaginal secretions):
often from contaminated needles among IV drug abusers;
intimate/sexual contact accounts for 50% of cases of fulminant hepatitis
● In an adult who develops acute hepatitis B, there is approximately 10%
chance that it will progress into chronic hepatitis; in the neonate the
chance is 90% for chronic hepatitis.
● Incubation period is very long: 1 - 6 months
CLINICAL MANIFESTATIONS
● Symptoms may be insidious and variable; subclinical episodes frequently
occur, fever and respiratory symptoms are rare; some patients have
arthralgias and rashes
● Loss of appetite, dyspepsia, abdominal pain, general aching, malaise, and
weakness may occur.
● Jaundice may or may not be evident. With jaundice, there are light
colored stools and dark urine.
● Liver may be tender and enlarged; spleen is enlarged and palpable in a
few patients. Posterior cervical lymph nodes may also be enlarged.
RISK FACTORS
● people who share needles
● health workers who are exposed to infected blood
ASSESSMENT & DIAGNOSTIC METHODS
● Hepatitis B surface antigen appears in blood of up to 90% of patients.
Additional antigens help to confirm diagnosis.
PREVENTION
● Screening of blood donors
● Good personal hygiene
● Education HEPATITIS D
● Hepatitis B vaccine
MEDICAL MANAGEMENT ● Hepatitis D (delta agent) occurs in some cases of hepatitis B. Because the
● Alpha-interferon has shown promising results. virus requires hepatitis B surface antigen for its replication, only patients
● Lamivudine (Epivir) and adefovir (Hepsera). with hepatitis B are at risk.
● Bed rest and restriction of activities until hepatic enlargement and ● It is common in IV drug users, hemodialysis patients, and recipients of
elevation of serum bilirubin and liver enzymes have disappeared. multiple blood transfusions.
● Maintain adequate nutrition; restrict proteins when the ability of the liver ● Sexual contact is an important mode of transmission of hepatitis B and D.
to metabolize protein byproducts is impaired. Incubation varies between 30 and 150 days.
● Administer antacids and antiemetics for dyspepsia and general malaise; ● The symptoms are similar to those of hepatitis B except that patients are
avoid all medications if patient is vomiting. more likely to have fulminant hepatitis and progress to chronic active
● Provide hospitalization and fluid therapy if vomiting persists. hepatitis and cirrhosis. Treatment is similar to that for other forms of
NURSING MANAGEMENT hepatitis.
● RNA virus that infects either simultaneously with hepatitis B or as a super-
infection in a person with chronic hepatitis B
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 17
● Hepatitis D infection cannot occur unless there is current and ongoing ● Maintenance of food and fluid intake
replication of the hepatitis B virus ● 3,000 ml/day of fluids for fever and vomiting; monitor I and O, weight
● Overall, this infection carries the highest risk among acute viral hepatitis ● Well – balanced diet; encourage fruit juices and carbonated beverages
for fulminant disease; the risk is even greater in super-infection ● Fats may need to be restricted
● Predominantly seen in patients exposed to blood products (drug addicts ● Alcoholic beverages should be avoided
and hemophiliacs). If anti-HBs antibodies are present, then that person is ● Prevention of injury
immune to hepatitis B and D ● Monitor PT (bleeding tendencies): plan so that all blood samples are
collected at one time to avoid several punctures
- avoid parenteral injections, if possible
- apply pressure to injection sites and venipuncture sites for 5
minutes
● Monitor Hgb/Hct, urine and stools for fresh or old blood; the skin for
petechiae
● advise client to use soft toothbrush or swabs
● administer Vitamin K as ordered
● Provision of comfort measures
● Relaxing baths, backrubs, fresh linens and quiet dark environment
● Relieve pruritus through the following measures:
- Use of cool, light, non-restrictive clothing
- Use of soft, dry, clean bedding, use of warm baths
- Application of emollient creams and lotions to dry skin.
- Maintenance of a cool environment
- Administration of antihistamines as ordered
- Use of diversional activities, e.g. reading, TV and radio
HEPATITIS TERMS AND ABBREVIATIONS
Hepatitis A
HEPATITIS E
HAV HepatItIs A virus; etiologic agent of hepatitis A formerly
● The hepatitis E virus is transmitted by the fecal-oral route, principally infectious hepatitis)
through contaminated water and poor sanitation.
● Incubation is variable and is estimated to range between 15 and 65 days.
In general, hepatitis E resembles hepatitis A. AntI-HAV Anybody to hepatitis A virus; appears in serum soon
● It has a self-limited course with an abrupt onset. Jaundice is almost always after onset of symptoms; disappears after 3-12 months
present. Chronic forms do not develop.
● The major method of prevention is avoiding contact with the virus IgM anti-HAV IgM antibody to HAV; indicates recent infection with
through hygiene (hand washing). The effectiveness of immune globulin in HAV; positive up to 6 months after infection
protecting against hepatitis E virus is uncertain.
HEPATITIS G Hepatitis B
● Hepatitis G (the latest form) is a posttransfusion hepatitis with an
incubation period of 14 to 145 days. HBV Hepatitis B virus; etiologic agent of hepatitis B (formerly
● Autoantibodies are absent.
serum hepatitis)
HBsAG Hepatitis B surface antigen (Australian antigen);
indicates acute or chronic hepatitis B or carrier state;
Indicates infectious state
Anti-HBs Antibody to hepatitis B surface antigen; indicates
prior exposure and immunity to hepatitis; may
indicate passive antibody from HBIG or immune
response from hepatitis B vaccine
HBeAg Hepatitis B e-antigen; present in serum early in
course; indicates highly infectious stage of
hepatitis B;persistence in serum indicates
progression to chronic hepatitis
Anti-HBe Antibody to hepatitis B A-antigen: suggests low
titer of HBV
ASSESSMENT FINDINGS: HBcAg Hepatitis B core antigen: found in liver cells: not
Preicteric stage (prodromal phase) = 1 week
- Anorexia (major manifestation), N&V, fatigue, constipation or easily detected in serum
diarrhea, weight loss
- RUQ discomfort, hepatomegaly, splenomegaly, lymphadenopathy Anti-HBc Antibody to hepatitis B core antigen; most sensitive
Icteric stage indicator of hepatitis B; appears late in the acute phase
- Fatigue, weight loss, light-colored stools, dark urine of the diseasel indicates infection of HBV at some time in
- Continued hepatomegaly with tenderness, lymphadenopathy, the past
splenomegaly
- Jaundice, pruritus
Posticteric stage IgM anti-HBc IgM antibody to HBcAg; present for up to 6 months after
- Fatigue, but an increased sense of well-being, hepatomegaly HBV infection
gradually decreasing
COLLABORATIVE MANAGEMENT
● Promotion of rest to relieve fatigue
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 18
Hepatitis C LIVER CIRRHOSIS
Destroyed liver cells are replaced by scar tissue, resulting in architectural
changes & malfunction of the liver
HCV Hepatitis C virus (formerly non-A, non-B virus); may be
more than one virus
Hepatitis D
HDV Hepatitis D virus (delta agents); etiologic agent to
hepatitis D; HBV required for replication
HDAg Hepatitis delta antigen; detectable in early acute HDV
infection
Anti-HDV Antibody to HDV; indicates past or present infection with
HDV
Hepatitis E
Types
● Laênnec’s cirrhosis - associated with alcohol abuse and malnutrition;
HEV Hepatitis E virus; etiologic agent of hepatitis E characterized by an accumulation of fat in the liver cells, progressing to
widespread scar formation.
Hepatitis G ● Postnecrotic cirrhosis - results in severe inflammation with massive
necrosis as a complication of viral hepatitis.
● Cardiac cirrhosis - occurs as a consequence of RSHF; manifested by
hepatomegaly with some fibrosis.
HGV Hepatitis G virus; also known as GB virus C or GB-C ● Biliary cirrhosis - associated with biliary obstruction, usually in the
common bile duct; results in chronic impairment of bile excretion
II. CIRRHOSIS. HEPATIC
● Cirrhosis is a chronic disease characterized by replacement of normal liver
tissue with diffuse fibrosis that disrupts the structure and function of the
liver. Cirrhosis, or scarring of the liver, is divided into three types:
alcoholic, most frequently due to chronic alcoholism and the most
common type of cirrhosis; postnecrotic, a late result of a previous acute
viral hepatitis; and biliary, a result of chronic biliary obstruction and
infection (least common type of cirrhosis).
ASSESSMENT:
● Anorexia, weakness, weight loss (liver is unable to metabolize nutrients
and store fat-soluble vitamins)
● Fever (in response to tissue injury)
● Jaundice, pruritus, tea colored urine (due to bilirubin in the blood)
- remember!!! bilirubin is conjugated initially before excretion
● Increased Bleeding tendencies. (liver is unable to store Vit. K.) There is
also impaired production of clotting factors)
● Portal HPN
PATHOLOGY
● In portal hypertension
Chronic, progressive disease characterized by inflammation, fibrosis, and - plasma shift into interstitial spaces within the liver due to the
degeneration of the liver parenchymal cells increase pressure. The collection of fluids shifts out of the Glisson’s
capsule and accumulate in the peritoneal cavity
● The liver is unable to metabolize protein, thereby hypoalbuminemia
occurs
- result to decreased oncotic pressure, fluids shift out of the IVC, and
accumulate in the peritoneal cavity.
● The liver is unable to excrete adrenal cortex hormone, one of which is
aldosterone
- Hyperaldosteronism leads to retention of sodium and water
● Esophageal varices = 2° to backpressure
● Internal hemorrhoids, leg varicosities, and dependent edema
- due to venous stasis, increasing hydrostatic pressure. This leads to
shifting of plasma into interstitial space
● Consequences of Portal HPN:
- Hepatomegaly= initially, then the liver shrinks in size as fibrosis
replaces the liver parenchyma
- Splenomegaly= due to increased backpressure of the blood
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 19
- Caput medusae (dilated veins over the abdomen) - Keep nails short to avoid skin excoriation from scratching.
- Spider angioma (telangiectasia / dilated capillaries over the face - Apply cool, moist compresses to pruritic areas.
and anterior trunk)= due to increased estroge Promote nutritional intake
- Palmar erythema. This is also due to elevated estrogen level in - Encourage small frequent feedings.
males. - Promote a high-calorie, low- to moderate- protein, high CHO, low-
- Ascites fat diet, with supplemental vitamin therapy (vitamins A, B- complex,
C, D, K, and folic acid)
Prevent infection
- Prevent skin breakdown by frequent turning and skin care.
- Provide reverse isolation for clients with severe leukopenia; pay
special attention to hand-washing technique.
- Monitor WBC
Monitor/prevent bleeding.
Administer diuretics as ordered
Provide client teaching & D/C planning concerning:
- Avoidance of agents that may be hepatotoxic (sedatives, opiates, or
OTC drugs detoxified by the liver)
- How to assess for weight gain and increased abdominal girth
- Avoidance of persons with upper respiratory infections
- Recognition and reporting of signs of recurring illness (liver
tenderness, increased jaundice, increased fatigue, anorexia)
- Avoidance of all alcohol
- Avoidance of straining at stool, vigorous blowing of nose and
coughing, to decrease the incidence of bleeding
CLINICAL MANIFESTATIONS
● Compensated cirrhosis: usually found secondary to routine physical
examination; vague symptoms
● Decompensated cirrhosis: symptoms of decreased proteins, clotting
factors, and other substances and manifestations of portal hypertension.
● Liver enlargement early in the course (fatty liver); later in course, liver size
decreases from scar tissue.
● Portal obstruction and ascites: Organs become the seat of chronic passive
congestion; indigestion and altered bowel function result.
● Infection and peritonitis: Clinical signs may be absent, necessitating
paracentesis for diagnosis.
● Gastrointestinal varices: prominent, distended abdominal blood vessels;
distended blood vessels throughout the GI tract; varices or hemorrhoids;
hemorrhage from the stomach.
● Edema.
● Vitamin deficiency (A, C, and K) and anemia.
● Mental deterioration with impending hepatic encephalopathy and
hepatic coma.
● Males (high estrogen) will result to: ASSESSMENT & DIAGNOSTIC METHODS
- Decreased libido, Impotence, Fall of body hair, Atrophy of testicles, ● Liver function tests (eg, serum alkaline phosphatase, aspartate
gynecomastia aminotransferase [AST] [serum glutamic oxaloacetic transaminase
● Females (high androgen) (SGOT)I, alanine aminotransferase [ALT] [serum glutamic pyruvic
- Hirsutism transaminase (SGPT)], GGT, serum cholinesterase, and bilirubin),
- acne prothrombin time, ABGs, biopsy
- deepening of voice ● Ultrasound scanning
- Virilism (development or premature development of male ● CT scan
secondary sexual characteristics) ● MRI
HEPATIC ENCEPHALOPATHY ● Radioisotopic liver scans
● Accumulation of AMMONIA because the liver cannot convert ammonia MEDICAL MANAGEMENT
into urea that can lead to hepatic coma (Ammonia is by product of CHON Medical management is based on presenting symptoms
metabolism) ● Treatment includes antacids, vitamins and nutritional supplements,
● initial manifestations: BEHAVIORAL changes and MENTAL changes balanced diet; potassium-sparing diuretics (for ascites); avoidance of
● Other findings in advanced stages are: alcohol.
- asterixis – flapping tremors of the hands ● Colchicine may increase the length of survival in patients with mild to
- confusion / disorientation moderate cirrhosis.
- delirium / hallucination NURSING MANAGEMENT
- fetor hepaticus - disagreeable odor from the mouth Promoting Rest
- coma ● Position bed for maximal respiratory efficiency; provide oxygen if needed.
DIAGNOSTIC TESTS ● Initiate efforts to prevent respiratory, circulatory, and vascular
● SGOT or AST, SGPT, LDH, alkaline phosphatase increased disturbances.
● Serum bilirubin increased ● Encourage patient to increase activity gradually and plan rest with activity
● PT prolonged and mild exercise.
● Serum albumin decreased Improving Nutritional Status
● Hgb/Hct decreased ● Provide a nutritious, high-protein diet supplemented by B Complex
● BSP increased vitamins and others, including A, C, and K.
NURSING INTERVENTIONS ● Encourage patient to eat: Provide small, frequent meals, consider patient
Provide sufficient rest and comfort• Provide bed rest with bathroom privileges. preferences, and provide protein supplements, if indicated.
- Encourage gradual, progressive, increasing activity with planned ● Provide nutrients by feeding tube or total PN if needed.
rest periods. ● Provide patients who have fatty stools (steatorrhea) with water-soluble
- Institute measures to relieve pruritus. forms of fat-soluble vitamins
- Do not use soaps and detergents ● A, D, and E, and give folic acid and iron to prevent anemia.
- Bathe in tepid water followed by application of an emollient lotion. ● Provide a low-protein diet temporarily if patient shows signs of
- Provide cool, light, nonrestrictive clothing. impending or advancing coma; restrict sodium if needed.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 20
Providing Skin Care
● Change patient's position frequently.
● Avoid using irritating soaps and adhesive tape.
● Provide lotion to soothe irritated skin; take measures to prevent patient
from scratching the skin.
Reducing Risk of Injury
● Use padded side rails if patient becomes agitated or restless.
● Orient to time, place, and procedures to minimize agitation.
● Instruct patient to ask for assistance to get out of bed.
● Carefully evaluate any injury because of the possibility of internal
bleeding.
● Provide safety measures to prevent injury or cuts (electric razor, soft
toothbrush). NURSING INTERVENTIONS
● Apply pressure to venipuncture sites to minimize bleeding. ● Assess respiratory status for possible distress.
Monitoring and Managing Complications ● Assess characteristics of abdominal pain and changes over time.
● Monitor for bleeding and hemorrhage. ● Administer medications as ordered.
● Monitor the patient's mental status closely and report changes so that ● Perform frequent abdominal assessment
treatment of encephalopathy can be initiated promptly. ● Monitor and maintain F&E balance; monitor for signs of septic shock.
● Carefully monitor serum electrolyte levels are and correct if abnormal. ● Maintain patency of NG or intestinal tubes
● Administer oxygen if oxygen desaturation occurs; monitor for fever or ● Encourage deep breathing exercises
abdominal pain, which may signal the onset of bacterial peritonitis or ● Place client in Fowler’s position to localize peritoneal contents
other infection. ● Provide routine pre- and post-op care if surgery ordered
● Assess cardiovascular and respiratory status; administer diuretics,
implement fluid restrictions, and enhance patient positioning, if needed. III. ESOPHAGEAL VARICES. BLEEDING
● Monitor intake and output, daily weight changes, changes in abdominal
girth, and edema formation. ● Bleeding or hemorrhage from esophageal varices is one of the major
● Monitor for nocturia and, later, for oliguria, because these states indicate causes of death in patients with cirrhosis.
increasing severity of liver dysfunction. ● Esophageal varices are dilated tortuous veins usually found in the
submucosa of the lower esophagus; they may develop higher in the
PERITONITIS esophagus or extend into the stomach.
● The condition is nearly always caused by portal hypertension.
PERITONITIS ● Risk factors for hemorrhage include muscular strain from heavy lifting;
Local or generalized inflammation of part or all of the parietal and visceral straining at stool; sneezing, coughing, or vomiting; esophagitis or
surfaces of the abdominal cavity irritation of vessels (rough food or irritating fluids); reflux of stomach
PATHOLOGY: contents (especially alcohol); and salicylates or any drug that erodes the
Initial response esophageal mucosa.
- edema, vascular congestion, hypermotility of the bowel and
outpouring of plasma-like fluid from the extracellular, vascular, and
interstitial compartments into the peritoneal space
Later response
- abdominal distension leading to respiratory compromise,
hypovolemia results in decreased urinary output
Intestinal motility gradually decreases and progresses to paralytic ileus
CAUSES
● Caused by trauma (blunt or penetrating)
● Inflammatory conditions
- ulcerative colitis, diverticulitis, pelvic inflammatory disease
● Ischemia
● Ruptured appendix
● Perforated peptic ulcer
● UTI
● Bowel obstruction (volvulus, intestinal obstruction)
● Bacteria invasion
ASSESSMENT FINDINGS
CLINICAL MANIFESTATIONS
● Severe abdominal PAIN, rebound tenderness, muscle
● Hematemesis, melena, or general deterioration in mental or physical
● rigidity, absent bowel sounds, abdominal distension
status; often a history of alcohol abuse.
● Anorexia, N&V
● Signs and symptoms of shock (cool clammy skin, hypotension,
● Shallow respirations; decreased urinary output; weak, rapid
tachycardia) may be present
● pulse; fever
ASSESSMENT & DIAGNOSTIC METHODS
● Signs of shock
● Endoscopy, barium swallow, ultrasonography, CT, and angiography
- Tachycardia, Tachypnea, Oliguria, Restlessness, Weakness, Pallor,
● Neurologic and portal hypertension assessment
Diaphoresis
● Liver function tests (serum aminotransferases, bilirubin, alkaline
● Diagnostic tests
phosphatase, and serum proteins)
- WBC elevated WBC (20,000/cu. mm. or higher)
● Splenoportography, hepatoportography, and celiac angiography
- Hct elevated (if hemoconcentration)
MEDICAL MANAGEMENT
MANAGEMENT
● Aggressive medical care includes evaluation of extent of bleeding and
● NPO with fluid replacement
continuous monitoring of vital
● Drug therapy: antibiotics to combat infection, analgesics for pain
● SIgnS when hematemesis and melena are present.
● NGT is inserted to relieve abdominal distention
● Signs of potential hypovolemia are noted; blood volume is monitored
● Peritoneal lavage with warm saline
with a central venous catheter or pulmonary artery catheter.
● Insertion of drainage tubes
● Oxygen is administered to prevent hypoxia and to maintain adequate
● Fluid, electrolyte and colloid replacement, TPN solutions
blood oxygenation, and IV fluids and volume expanders are administered
SURGERY
to restore fluid volume and replace electrolytes.
● Laparotomy: opening made through the abdominal wall into the
● Transfusion of blood components may also be required.
peritoneal cavity to determine the cause of peritonitis
● Nonsurgical treatment is preferred because of the high mortality
● Depending on cause, bowel resection may be necessary
associated with emergency surgery to control bleeding from esophageal
varices and because of the poor physical condition of most of these
patients. Nonsurgical measures include:
● Pharmacologic therapy: vasopressin (Pitressin), vasopressin with
nitroglycerin, somatostatin and octreotide (Sandostatin), beta-blocking
agents, and nitrates
● Balloon tamponade, saline lavage, and endoscopic sclerotherapy
● Esophageal banding therapy and variceal band ligation
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 21
● Transjugular intrahepatic portosystemic shunting (TIPS)
SURGICAL MANAGEMENT THE EXOCRINE PANCREAS
If necessary, surgery may involve the following:
● The secretions of the exocrine portion of the pancreas are collected in
● Direct surgical ligation of varices
the pancreatic duct, which joins the common bile duct and enters the
● Splenorenal, mesocaval, and portacaval venous shunts
duodenum at the ampulla of Vater.
● Esophageal transection with devascularization.
● Surrounding the ampulla is the sphincter of Oddi, which partially controls
NURSING MANAGEMENT
the rate at which secretions from the pancreas and the gallbladder enter
Provide postoperative care similar to that for any thoracic or abdominal
the duodenum. The secretions of the exocrine pancreas are digestive
operation.
enzymes high in protein content and an electrolyte-rich fluid.
● Monitor patient's physical condition and evaluate emotional responses
● The secretions, which are very alkaline because of their high
and cognitive status.
concentration of sodium bicarbonate, are capable of neutralizing the
● Monitor and record vital signs. Assess nutritional status.
highly acid gastric juice that enters the duodenum.
● Perform a neurologic assessment, monitoring for signs of hepatic
● The enzyme secretions include amylase, which aids in the digestion of
encephalopathy (findings may range from drowsiness to encephalopathy
carbohydrates; trypsin, which aids in the digestion of proteins; and
and coma).
lipase, which aids in the digestion of fats. Other enzymes that promote
● Treat bleeding by complete rest of the esophagus. Initiate parenteral
the breakdown of more complex foodstuffs are also secreted.
nutrition (P) as ordered.
● Hormones originating in the GI tract stimulate the secretion of these
● Assist patient to avoid straining and vomiting. Maintain gastric suction to
exocrine pancreatic juices. The hormone secretin is the major stimulus
keep the stomach as empty as possible.
for increased bicarbonate secretion from the pancreas, and the major
● Provide frequent oral hygiene and moist sponges to the lips to relieve
stimulus for digestive enzyme secretion is the hormone CCK-PZ. The
thirst.
vagus nerve also influences exocrine pancreatic secretion.
● Closely monitor blood pressure.
● Provide vitamin K therapy and multiple blood transfusions as ordered for THE ENDOCRINE PANCREAS
blood loss.
● Provide a quiet environment and calm reassurance to reduce anxiety and ● The islets of Langerhans, the endocrine part of the pancreas, are
agitation. Provide emotional support and pertinent explanations collections of cells embedded in the pancreatic tissue. They are
regarding medical and nursing interventions. composed of alpha, beta, and delta cells. The hormone produced by the
● Monitor closely to detect and manage complications, including beta cells is called insulin; the alpha cells secrete glucagon, and the delta
hypovolemic or hemorrhagic shock, hepatic encephalopathy, electrolyte cells secrete somatostatin.
imbalance, metabolic and respiratory alkalosis, alcohol withdrawal
syndrome, and seizures. INSULIN
GALLBLADDER ● A major action of insulin is to lower blood glucose by permitting entry of
● The gallbladder, a pear-shaped, hollow, saclike organ, 7.5 to 10 cm (3 to glucose into the cells of the liver, muscle, and other tissues, where it is
4 in) long, lies in a shallow depression on the inferior surface of the liver, either stored as glycogen or used for energy. Insulin also promotes the
to which it is attached by loose connective tissue. The capacity of the storage of fat in adipose tissue and the synthesis of proteins in various
gallbladder is 30 to 50 mL of bile. Its wall is composed largely of smooth body tissues.
muscle. The gallbladder is connected to the common bile duct by the ● In the absence of insulin, glucose cannot enter the cells and is excreted in
cystic duct (Fig. 40-1). the urine. This condition, called diabetes mellitus, can be diagnosed by
● The gallbladder functions as a storage depot for bile. Between meals, high levels of glucose in the blood. In diabetes mellitus, stored fats and
when the sphincter of Oddl is closed, bile produced by the hepatocytes protein are used for energy instead of glucose, causing loss of body mass.
enters the gallbladder. (Diabetes mellitus is discussed in detail in Chapter 41.)
● During storage, a large portion of the water in bile is absorbed through ● The level of glucose in the blood normally regulates the rate of insulin
the walls of the gallbladder, so that bile in the gallbladder is five to 10 secretion from the pancreas.
times more concentrated than that originally secreted by the liver.
● When food enters the duodenum, the gallbladder contracts and the GLUCAGON
sphincter of Oddi (located at the junction of the common bile duct with
the duodenum) relaxes. ● The effect of glucagon (opposite to that of insulin) is chiefly to raise the
● Relaxation of this sphincter allows the bile to enter the intestine. This blood glucose by converting glycogen to glucose in the liver. Glucagon is
response is mediated by secretion of the hormone cholecystokinin- secreted by the pancreas in response to a decrease in the level of blood
pancreozymin (CCK-PZ) from the intestinal wall. Bile is composed of glucose.
water and electrolytes (sodium, potassium, calcium, chloride, and
bicarbonate) along with significant amounts of lecithin, fatty acids, SOMATOSTATIN
cholesterol, bilirubin, and bile salts.
● The bile salts, together with cholesterol, assist in emulsification of fats in ● Somatostatin exerts a hypoglycemic effect by interfering with release of
the distal ileum. They are then reabsorbed into the portal blood for return growth hormone from the pituitary and glucagon from the pancreas, both
to the liver, after which they are once again excreted into the bile. of which tend to raise blood glucose levels.
● This pathway from hepatocytes to bile to intestine and back to the
hepatocytes is called the enterohepatic circulation. Because of this
circulation, only a small fraction of the bile salts that enter the intestine ENDOCRINE CONTROL OF CARBOHYDRATE METABOLISM
are excreted in the feces. This decreases the need for active synthesis of
bile salts by the liver cells. ● Glucose required for energy is derived by metabolism of ingested
● Approximately half of the bilirubin, a pigment derived from the carbohydrates and also from proteins by the process of gluconeogenesis.
breakdown of red blood cells, is a component of bile. It is converted by Glucose can be stored temporarily in the form of glycogen in the liver,
the intestinal flora into urobilinogen, a highly soluble substance. muscles, and other tissues. The endocrine system controls the level of
● Urobilinogen is either excreted in the feces or returned to the portal blood glucose by regulating the rate at which glucose is synthesized,
circulation, where it is reexcreted into the bile. About 5% is normally stored, and moved to and from the bloodstream.
absorbed into the general circulation and then excreted by the kidneys. ● Through the action of hormones, blood glucose is normally maintained
● If the flow of bile is impeded (eg, by gallstones in the bile ducts), bilirubin at less than 100 mg/dL (5.5 mmol/L).
does not enter the intestine. As a result. blood levels of bilirubin increase. ● Insulin is the primary hormone that lowers the blood glucose level.
● This causes increased renal excretion of urobilinogen, which results from Hormones that raise the blood glucose level are glucagon, epinephrine,
conversion of bilirubin in the small intestine, and decreased excretion in adrenocorticosteroids, growth hormone, and thyroid hormone.
the stool. These changes produce many of the signs and symptoms seen ● The endocrine and exocrine functions of the pancreas are interrelated.
in gallbladder disorders. The major exocrine function is to facilitate digestion through secretion
of enzymes into the proximal duodenum. Secretin and CCK-PZ are
PANCREAS hormones from the Gl tract that aid in the digestion of food substances
by controlling the secretions of the pancreas.
● Neural factors also influence pancreatic enzyme secretion. Considerable
● The pancreas, located in the upper abdomen, has endocrine as well as dysfunction of the pancreas must occur before enzyme secretion
exocrine functions (see Fig. 40-1). The exocrine functions include decreases and protein and fat digestion becomes impaired. Pancreatic
secretion of pancreatic enzymes into the gastrointestinal (Gl) tract enzyme secretion is normally 1500 to 2500 mL/day.
through the pancreatic duct. The endocrine functions include secretion
of insulin, glucagon, and somatostatin directly into the bloodstream. IV. CHOLELITHIASIS & CHOLECYSTITIS
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 22
● In cholelithiasis, calculi (gallstones) usually form in the gallbladder from
solid constituents of bile and vary greatly in size, shape, and composition.
● There are two major types of gallstones: pigment stones, which contain
an excess of unconjugated pigments in the bile, and cholesterol stones
(the more common form), which result from bile supersaturated with
cholesterol due to increased synthesis of cholesterol and decreased
synthesis of bile acids that dissolve cholesterol.
● Risk factors for pigment stones include cirrhosis, hemolysis, and
infections of the biliary tract. These stones cannot be dissolved and must
be removed surgically.
● Risk factors for cholesterol stones include gender (women are two to
three times more likely to develop cholesterol stones); use of oral
contraceptives, estrogens, and clofibrate; age (usually older than 40
years); multiparous status; and obesity. There is also an increased risk
related to diabetes, Gl tract disease, T-tube fistula, and ileal resection or
bypass.
● FAT, FEMALE, FORTY, FERTILE: More common in women after age 40
(estrogen therapy), women taking oral contraceptives, and in the obese
● Cholecystitis: acute or chronic inflammation of the gallbladder
CLINICAL MANIFESTATIONS
● May be silent, producing no pain and only mild GI symptoms
● May be acute or chronic with epigastric distress (fullness, abdominal
distention, and vague upper right quadrant pain); may follow a meal rich
in fried or fatty foods
● If the cystic duct is obstructed, the gallbladder becomes distended,
inflamed, and eventually infected; fever and palpable abdominal mass;
biliary colic with excruciating upper right abdominal pain, radiating to
back or right shoulder with nausea and vomiting several hours after a
heavy meal; restlessness and constant or colicky pain
● Jaundice, accompanied by marked itching, with obstruction of the
common bile duct, in a small percentage of patients
● Very dark urine; grayish or clay-colored stool
● Deficiencies of vitamins A, D, E, and K (fat-soluble vitamins)
ASSESSMENT FINDINGS
● Cholecystitis, an acute complication of cholelithiasis, is an acute infection ● Most patients are asymptomatic.
of the gallbladder. Most patients with cholecystitis have gallstones ● When symptomatic; PAIN in RUQ and epigastric pain lasting
(calculous cholecystitis). A gallstone obstructs bile outflow and bile in the approximately 30 min.
gallbladder initiates a chemical reaction, resulting in edema, compromise ● Fever & leukocytosis (WBC)
of the vascular supply, and gangrene. In the absence of gallstones, ● Charcot triad
cholecystitis (acalculous) may occur after surgery, severe trauma, or - fever, jaundice, pain in RUQ pain (ascending cholangitis)
burns, or with torsion, cystic duct obstruction, multiple blood ● Intolerance for fatty foods (steatorrhea, N&V, sensation of fullness)
transfusions, and primary bacterial infections of the gallbladder. ● Pruritus, easy bruising, dark amber urine
● Infection causes pain, tenderness, and rigidity of the upper right DIAGNOSTIC TESTS
abdomen and is associated with nausea and vomiting and the usual signs ● Direct bilirubin transaminase, alkaline phosphatase, WBC, amylase,
of inflammation. lipase: all increased
● Purulent fluid inside the gallbladder indicates an empyema of the ● Oral cholecystogram (gallbladder series): positive for gallstone
gallbladder. ASSESSMENT & DIAGNOSTIC METHODS
● Cholecystogram, cholangiogram; celiac axis arteriography
● Laparoscopy
● Ultrasonography; EUS
● Helical CT scans and MRI; ERCP
● Serum alkaline phosphatase; gamma-glutamyl (GGT), gamma-glutamyl
transpeptidase (GGTP), LDH
● Cholesterol levels
GERONTOLOGIC CONSIDERATIONS
● Surgical intervention for disease of the biliary tract is the most common
operation performed in the elderly.
● Biliary disease may be accompanied or preceded by symptoms of septic
shock: oliguria, hypotension, mental changes, tachycardia, and
tachypnea.
● Cholecystectomy is usually well tolerated and carries a low risk if expert
assessment and care are provided before, during, and after surgery.
● Mortality from serious complications is high. Risk of complications and
shorter hospital stays make it essential that older patients and their
family members receive specific information about signs and symptoms
of complications and measures to prevent them.
NURSING INTERVENTION
● Administer pain medications as ordered and monitor for effects.
● Administer IV fluids as ordered.
● Provide small, frequent meals of modified diet, low fat (if oral intake
allowed)
● Provide care to relieve pruritus
● Provide care for the client with a cholecystectomy or choledochostomy
MEDICAL MANAGEMENT
● Major objectives of medical therapy are to reduce the incidence of acute
episodes of gallbladder pain and cholecystitis by supportive and dietary
management and, if possible, to remove the cause by pharmacotherapy,
endoscopic procedures, or surgical intervention
● Supportive treatment: NPO with NG intubation and IV fluids
● Diet modification with administration of fat- soluble vitamins
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 23
Drug therapy
● Narcotic analgesics (Demerol is the drug of choice) for pain
● Morphine sulfate is contraindicated because it causes spasms of the
sphincter of Oddi
● Anticholinergics (atropine) may be used for pain
● Antiemetics
Surgery
● Cholecystectomy
● Choledochostomy
● Choledochotomy
❖ Cholecystectomy - removal of the gallbladder with insertion of a T-tube
into the common bile duct if common bile duct exploration is ● Achieve remission with rest, IV fluids, nasogastric suction. analgesia, and
❖ performed antibiotics.
❖ Choledochotomy - opening of common duct, removal of stone, and ● Diet immediately after an episode is usually low-fat liquids with high
insertion of a T-tube protein and carbohydrates followed by solid soft foods as tolerated,
❖ Laparoscopic Cholecystectomy - performed via laparoscopy for avoiding eggs, cream, pork, fried foods, cheese, rich dressings, gas-
uncomplicated cases when client has not had previous abdominal surgery forming vegetables, and alcohol.
PHARMACOLOGIC THERAPY
❖ Cholecystostomy - opening of the gallbladder to remove stones
● Ursodeoxycholic acid (UDCA [Urso, Actigall]) and chenodeoxycholic acid
(chenodiol or CDCA [Chenix]) are effective in dissolving primarily
cholesterol stones.
● Patients with significant, frequent symptoms; cystic duct occlusion; or
pigment stones are not candidates for therapy with UDCA.
NON-SURGICAL REMOVAL OF GALLSTONES
● In addition to dissolving gallstones, they can be removed by other
instrumentation (eg, catheter and instrument with a basket attached are
threaded through the T-tube tract or fistula formed at the time of T-tube
insertion, ERCP endoscope), intracorporeal lithotripsy (laser pulse), or
extracorporeal shock wave therapy (lithotripsy or extracorporeal shock
wave lithotripsy [ESWL]).
SURGICAL REMOVAL OF GALLSTONES
Goal of surgery is to relieve persistent symptoms, to remove the cause of biliary
colic, and to treat acute cholecystitis.
● Laparoscopic cholecystectomy: performed through a small incision or
puncture made through the abdominal wall in the umbilicus.
● Cholecystectomy: Gallbladder is removed through an abdominal incision
(usually right subcostal) after ligation of the cystic duct and artery.
● Mini Cholecystectomy: Gallbladder is removed through a small incision.
● Choledochostomy: incision into the common duct for stone removal.
● Cholecystostomy (surgical or percutaneous): Gallbladder is opened, and
NURSING INTERVENTIONS IN SURGERY: the stone, bile, or purulent drainage is removed.
● Provide routine pre-op care
● Provide routine post-op care PANCREATITIS
● Position client in semi-Fowler’s or side-lying positions; reposition
frequently.
● Splint incision when turning, coughing, and deep breathing
● Maintain/monitor functioning of T-tube
- Ensure that T-tube is connected to closed gravity drainage.
- Avoid kinks, clamping, or pulling of the tube.
Maintain/monitor functioning of T-tube
● Measure and record drainage every shift
● Expect 300 – 500 ml bile-colored drainage for the 1st 24° then 200 ml/24°
for 3 - 4 days
● Assess for signs of peritonitis
● Monitor color of urine and stools (stools will be light colored if bile is
flowing through T tube but normal color should reappear as drainage
diminishes)
● Assess skin around T-tube; cleanse frequently and keep dry ● An inflammatory process with varying degrees of pancreatic edema, fat
NUTRITIONAL & SUPPORTIVE THERAPY necrosis, or hemorrhage
● Proteolytic and lipolytic pancreatic enzymes are activated in the pancreas
rather than in the duodenum, resulting in tissue damage and
autodigestion of the pancreas
● Occurs most often in the middle aged
CAUSES
● Alcoholism/ alcohol abuse
● Biliary tract disease/ biliary obstruction
● Trauma, viral infection, penetrating duodenal ulcer, abscesses
● Drugs (antihypertensives, steroids, thiazide diuretics, antimicrobials,
immunosuppressives, oral contraceptives)
● Metabolic disorders (hyperparathyroidism, hyperlipidemia)
● Unknown/ autoimmune
ASSESSMENT FINDINGS
● Pain (LUQ radiating to back, flank, or substernal area) accompanied by
DOB (shallow respiration with pain), aggravated by eating
● N&V, decreased/absent bowel sounds,
● Abdominal tenderness w/ muscle-guarding
● (+) Grey Turner’s spots (ecchymoses on flanks)
● (+) Cullen’s sign (ecchymoses of periumbilical area)
● Tachycardia
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 24
DIAGNOSTIC TESTS
● High serum amylase (>300 somogyi units) & lipase
● High urinary amylase
● High blood sugar
● High lipid levels
● Low Serum calcium
● CT scan: enlargement of the pancreas
NURSING INTERVENTIONS
● Administer analgesics, antacids, and anticholinergics as ordered, monitor
effects
● Withhold food/fluid and eliminate odor and sight of food from
environment to decrease pancreatic stimulations
● Maintain NGT and assess for drainage.
● Institute Non-pharmacologic measures to decrease pain.
● Assist client to positions of comfort (knee chest, fetal position)
● Teach relaxation techniques and provide a quiet, restful environment.
Provide client teaching and discharge planning concerning
● Dietary regimen when oral intake permitted
● High CHO, high CHON, low-fat diet
● Eating small, frequent meals instead of three large ones
● Avoiding caffeine products
● Eliminating alcohol consumption
● Maintaining relaxed atmosphere after meals
● Recognition/reporting of signs of complications
● Continued N&V
V. PANCREATITIS, ACUTE
● Abdominal distension with increasing fullness
● Persistent weight loss
● Severe epigastric or back pain
● Frothy/foul-smelling bowel movements
● Irritability, confusion, persistent elevation of temperature (2 days)
MEDICAL MANAGEMENT
Drug Therapy
● Analgesics (Demerol) to relieve pain.
- MORPHINE is avoided because it can cause spasm of the sphincter
aggravating pain
● Smooth-muscle relaxants to relieve pain
- papaverine, nitroglycerin
● Anticholinergics to decrease pancreatic stimulation
- atropine, propantheline bromide
● Antacids to decrease pancreatic stimulation
● H2-antagonists, vasodilators, calcium gluconate
Diet modification
● NPO usually for a few days to promote GIT rest
● Pancreatitis (inflammation of the pancreas) is a serious disorder that can
● Peritoneal lavage
range in severity from a relatively mild, self limiting disorder to a rapidly
● Dialysis if the condition is severe
fatal disease that does not respond to any treatment.
● Acute pancreatitis is commonly described as an autodigestion of the
pancreas by the exocrine enzymes it produces, principally trypsin. Eighty
percent of patients with acute pancreatitis have biliary tract disease or a
history of long-term alcohol abuse. Other less common causes of
pancreatitis include bacterial or viral infection, with pancreatitis
occasionally developing as a complication of mumps virus. Many disease
processes and conditions have been associated with an increased
incidence of pancreatitis, including surgery on or near the pancreas,
medications, hypercalcemia, and hyperlipidemia
● Up to 10% of cases are idiopathic, and there is a small incidence of
hereditary pancreatitis. Mortality is high because of shock, anoxia,
hypotension, or fluid and electrolyte imbalances. Attacks of acute
pancreatitis may result in complete recovery, may recur without
permanent damage, or may progress to chronic pancreatitis.
CLINICAL MANIFESTATION
Severe abdominal pain is the major symptom.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 25
● Pain in the midepigastrium may be accompanied by abdominal ● Change position frequently to prevent atelectasis and pooling of
distention; a poorly defined, palpable abdominal mass; decreased respiratory secretions.
peristalsis; and vomiting that fails to relieve the pain or nausea. ● Assess respiratory status frequently (pulse oximetry, arterial blood
● Pain is frequently acute in onset (24 to 48 hours after a heavy meal gas [ABG] values), and teach patient techniques of coughing and deep
or alcohol ingestion); may be more severe after meals and unrelieved breathing and the use of incentive spirometry.
by antacids. Improving Nutritional Status
● Patient appears acutely ill. ● Assess nutritional status and note factors that alter the patient’s
● Abdominal guarding; rigid or boardlike abdomen (generally an ominous nutritional requirements (eg, temperature elevation, surgery, drainage).
sign, usually indicating peritonitis). ● Monitor laboratory test results and daily weights.
● Ecchymosis in the flank or around the umbilicus, which may indicate ● Provide enteral nutrition or PN as prescribed.
severe hemorrhagic pancreatitis. ● Monitor serum glucose level every 4 to 6 hours.
● Nausea and vomiting, fever, jaundice, mental confusion, agitation. ● Introduce oral feedings gradually as symptoms subside.
● Hypotension related to hypovolemia and shock. ● Avoid heavy meals and alcoholic beverages.
● May develop tachycardia, cyanosis, and cold, clammy skin. Maintaining Skin Integrity
● Acute renal failure common. ● Assess the wound, drainage sites, and skin carefully for signs of
● Respiratory distress and hypoxia. infection, inflammation, and breakdown.
● May develop diffuse pulmonary infiltrates, dyspnea, tachypnea, and ● Carry out wound care as prescribed, and take precautions to protect
abnormal blood gas values. intact skin from contact with drainage; consult with a wound–
● Myocardial depression, hypocalcemia, hyperglycemia, and disseminated ostomy–continence nurse as needed to identify appropriate skin care
intravascular coagulation (DIC). devices and protocols.
ASSESSMENT AND DIAGNOSTIC FINDINGS ● Turn patient every 2 hours; use of specialty beds may be indicated to
● Diagnosis is based on history of abdominal pain, the presence of prevent skin breakdown.
known risk factors, physical examination findings, and diagnostic MONITORING AND MANAGING COMPLICATIONS
findings (increased urine amylase level and white blood cell [WBC] Fluid and Electrolyte Disturbances
count; hypocalcemia; transient hyperglycemia; glucosuria and increased ● Assess fluid and electrolyte status by noting skin turgor and moistness of
serum bilirubin levels in mucous membranes.
● some patients). X-rays of abdomen and chest, ultrasound, and contrast- ● Weigh daily; measure all fluid intake and output.
enhanced computed tomography (CT) scan may be performed. ● Assess for other factors that may affect fluid and electrolyte status,
Hematocrit and hemoglobin levels are used to monitor the patient including increased body temperature and wound drainage.
for bleeding. ● Observe for ascites, and measure abdominal girth.
● Serum amylase and lipase levels are most indicative (elevated within ● Administer intravenous (IV) fluids and blood or blood products to
24 hours; amylase returns to normal within 48 to 72 hours; lipase maintain volume and prevent or treat shock.
remains elevated for longer period). Peritoneal fluid is evaluated for ● Report decreased blood pressure, reduced urine output, and low serum
increase in pancreatic enzymes. calcium and magnesium.
MEDICAL MANAGEMENT: ACUTE PHASE Pancreatic Necrosis
During the acute phase, management is symptomatic and directed toward ● Transfer patient to intensive care unit for close monitoring.
preventing or treating complications. ● Administer prescribed fluids, medications, and blood products.
● Oral intake is withheld to inhibit pancreatic stimulation and secretion of ● Assist with supportive management, such as mechanical ventilation.
pancreatic enzymes. Shock and Multiple Organ Failure
● Parenteral nutrition (PN) is administered to the debilitated patient. ● Monitor patient closely for early signs of neurologic, cardiovascular,
● Nasogastric suction is used to relieve nausea and vomiting and to renal, and respiratory dysfunction.
decrease painful abdominal distention and paralytic ileus. ● Prepare for rapid changes in patient status, treatment, and therapies;
● Histamine-2 (H2) receptor antagonists (cimetidine, ranitidine) or, respond quickly.
sometimes, proton pump inhibitors are given to decrease hydrochloric ● Inform family of status and progress of patient; allow time with patient.
acid secretion.
● Adequate pain medication, such as morphine, is administered. VI. PANCREATITIS, CHRONIC
Antiemetic agents may be prescribed to prevent vomiting.
● Correction of fluid, blood loss, and low albumin levels is necessary. ● Chronic pancreatitis is an inflammatory disorder characterized by
● Antibiotics are administered if infection is present. progressive anatomic and functional destruction of the pancreas. Cells
● Insulin is necessary if significant hyperglycemia occurs. are replaced by fibrous tissue with repeated attacks of pancreatitis.
● Aggressive respiratory care is provided for pulmonary infiltrates, effusion, The end result is obstruction of the pancreatic and common bile ducts
and atelectasis. and duodenum.
● Biliary drainage (drains and stents) results in decreased pain and ● In addition, there is atrophy of the epithelium of the ducts,
increased weight gain. inflammation, and destruction of the secreting cells of the pancreas.
● Surgical intervention may be performed for diagnosis, drainage, Alcohol consumption in Western societies and malnutrition worldwide
resection, or debridement. are the major causes. The incidence of pancreatitis among alcoholics is
MEDICAL MANAGEMENT: POST-ACUTE PHASE 50 times the rate in the non-drinking population.
● Antacids are given when the acute episode begins to resolve.
● Oral feedings low in fat and protein are initiated gradually.
● Caffeine and alcohol are eliminated. PATHOPHYSIOLOGY
● Medications (eg, thiazide diuretics, glucocorticoids, or oral ● Long-term alcohol consumption causes hypersecretion of protein in
contraceptives) are discontinued. pancreatic secretions, resulting in protein plugs and calculi within the
NURSING MANAGEMENT pancreatic ducts. Alcohol has a direct toxic effect on the cells of the
Relieving Pain and Discomfort pancreas. Damage is more severe in patients with diets low in protein and
● Administer analgesics as prescribed. Current recommendation for pain very high or very low in fat. Smoking is another factor in the
management is parenteral opioids, including morphine, hydromorphone, development of chronic pancreatitis. Because heavy drinkers usually
or fentanyl via patient controlled analgesia or bolus. smoke, it is difficult to separate the effects of the alcohol abuse and
● Frequently assess pain and the effectiveness of the pharmacologic smoking.
interventions. CLINICAL MANIFESTATIONS
● Withhold oral fluids to decrease formation and secretion of secretin. ● Recurring attacks of severe upper abdominal and back pain, accompanied
● Use nasogastric suctioning to remove gastric secretions and relieve by vomiting; opioids may not provide relief.
abdominal distention; provides frequent oral hygiene and care to ● Risk of addiction to opiates is high because of the severe pain.
decrease discomfort from the nasogastric tube and relieve dryness of ● There may be continuous severe pain or dull, nagging, constant pain.
the mouth. ● Weight loss is a major problem.
● Maintain patient on bed rest to decrease metabolic rate and to ● Altered digestion (malabsorption) of foods (proteins and fats) results in
reduce secretion of pancreatic enzymes; report increased pain (may be frequent, frothy, and foul- smelling stools with a high fat content
pancreatic hemorrhage or inadequate analgesic dosage). (steatorrhea).
● Provide frequent and repeated but simple explanations about treatment; ● As disease progresses, calcification of the gland may occur and calcium
patient may have clouded sensorium from pain, fluid imbalances, and stones may form within the ducts.
hypoxemia. ASSESSMENT AND DIAGNOSTIC METHODS
Improving Breathing Pattern ● Endoscopic retrograde cholangiopancreatography (ERCP) is the most
● Maintain patient in semi-Fowler’s position to decrease pressure on useful study.
diaphragm. ● Various imaging procedures, including magnetic resonance imaging
(MRI), CT scans, and ultrasound.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 26
● A glucose tolerance test evaluates pancreatic islet cell function. ● Hepatology - Hepatology is the medical specialty focusing on treatment
● Steatorrhea is best confirmed by laboratory analysis of fecal fat content. of diseases, disorders, and conditions of the liver. Hepatology is a
MEDICAL MANAGEMENT subspecialty of internal medicine, and is often practiced in conjunction
Treatment is directed toward preventing and managing acute attacks, with gastroenterology, another subspecialty of internal medicine.
relieving pain and discomfort, and managing exocrine and endocrine Hepatologists treat liver diseases such as all types of hepatitis, and
insufficiency of pancreatitis. cirrhosis of the liver.
● Endoscopy to remove pancreatic duct stones, correct strictures, and drain ● Liquid Chromatography-Mass Spectrometry (LC-MS) - An analytical
cysts may be effective in selected patients to manage pain and relieve chemistry technique that combines the physical separation capabilities of
obstruction. liquid chromatography (or HPLC) with the mass analysis capabilities of
● Pain and discomfort are relieved with analgesics; yoga may be an mass spectrometry. LC-MS is a powerful technique with has very high
effective nonpharmacologic method for pain reduction and for relief of sensitivity and specificity. Generally its application is oriented towards
other coexisting symptoms. the specific detection and potential identification of chemicals in the
● Patient should avoid alcohol and foods that produce abdominal pain presence of other chemicals (in a complex mixture).
and discomfort. No other treatment will relieve pain if patient continues ● Liver Biopsy - The removal of a small piece of tissue from the liver using
to consume alcohol. a special needle. The tissue is examined under a microscope to look for
● Diabetes mellitus resulting from dysfunction of pancreatic islet cells the presence of inflammation or liver damage.
is treated with diet, insulin, or oral hypoglycemic agents. Patient and ● Portal Circulation - Portal Circulation refers to the circulation of the blood
family are taught the hazard of severe hypoglycemia related to alcohol from the small intestine to the liver, via the portal vein.
use. ● Portal Vein - The hepatic portal vein is a vein in the abdominal cavity that
● Pancreatic enzyme replacement therapy is instituted for malabsorption drains blood from the gastrointestinal tract and spleen to the liver.
and steatorrhea. ● Varices - Enlarged veins within the gastrointestinal tract that form as a
● Surgery is done to relieve abdominal pain and discomfort, restore result of cirrhosis
drainage of pancreatic secretions, and reduce frequency of attacks
(pancreaticojejunostomy).
● Morbidity and mortality after surgical procedures are high because WEEK 4: DIABETES MELLITUS AND PITUITARY DISORDERS
of patient’s poor physical condition before surgery and concomitant
occurrence of cirrhosis
TERMINOLOGIES ANATOMY AND PHYSIOLOGY OF THE ENDOCRINE SYSTEM
● Albumin - A protein made in the liver that assists in maintaining blood Functions of the Endocrine System .
volume in the arteries and veins. If the liver is damaged, then the albumin Despite the huge variety of hormones, there are really only two mechanisms
can drop to very low levels, which may cause fluid to leak into the tissues by which hormones trigger changes in cells.
from the blood vessels, resulting in edema or swelling. In acute liver 1. Water equilibrium. The endocrine system controls water equilibrium
failure, there is an accumulation of fluid in the abdomen that is known as by regulating the solute concentration of the blood.
“ascites”. 2. Growth, metabolism, and tissue maturation. The endocrine system
● Ascites - A large, abnormal accumulation of fluid in the abdomen that can controls the growth of many tissues, like the bone and muscle, and
occur due to liver failure, cirrhosis and liver cancer. This condition the degree of metabolism of various tissues, which aids in the
requires immediate medical attention. maintenance of the normal body temperature and normal mental
● Cholate - The major primary bile acid produced in the liver that facilitates functions. Maturation of tissues, which appears in the development of
fat absorption and cholesterol excretion. adult features and adult behavior, are also determined by the endocrine
● Cirrhosis - A serious liver condition characterized by irreversible scarring system.
of the liver that can lead to liver failure and death. Alcohol and chronic 3. Heart rate and blood pressure management. The endocrine system
viral hepatitis (such as chronic hepatitis B and C) can cause continuous assists in managing the heart rate and blood pressure and aids in
inflammation of the liver, which can lead excess scar formation or fibrosis. preparing the body for physical motion.
Scarring results in the loss of liver cells and impairs liver function. 4. Immune system control. The endocrine system helps regulate the
● Decompensation - Term for describing the development of measurable production and functions of immune cells.
deterioration or clinical complication in patients with chronic liver 5. Reproductive function controls. The endocrine system regulates the
disease. development and the functions of the reproductive systems in males
● Encephalopathy - Serious brain function abnormalities experienced by and females.
some patients with advanced liver disease. Symptoms most commonly 6. Uterine contractions and milk release. The endocrine system controls
include confusion, disorientation, insomnia, and may progress to a coma. uterine contractions throughout the delivery of the newborn and
● Endoscopy - A medical procedure where a doctor puts a tube-like stimulates milk release from the breasts in lactating females.
instrument into the body to look inside. Unlike most other medical 7. Ion management. The endocrine system regulates Na+, K+, and Ca2+
imaging devices, endoscopes are inserted directly into the organ. There concentrations in the blood.
are many types of endoscopy, each of which is designed for looking at a 8. Blood glucose regulator. The endocrine system controls blood
certain part of the body. glucose levels and other nutrient levels in the blood.
● Enzymes - Naturally occurring chemical substances in the human body 9. Direct gene activation. Being lipid-soluble molecules, the steroid
that help a chemical reaction take place. hormones can diffuse through plasma membranes of their target
● Fibrosis - Growth of fibrous tissue in the liver where there is usually liver cells; once inside, the steroid hormone enters the nucleus and binds
cell damage or destruction. Fibrosis can lead to cirrhosis, an even more to a specific receptor protein there; then, the hormone-receptor
serious liver disease. complex binds to specific sites on the cell’s DNA, activating certain
● Gastroenterology - The field of medicine that focuses on the function and genes to transcribe messenger RNA; the mRNA then is translated in
disorders of the GI system, which includes the esophagus, stomach, the cytoplasm, resulting in the synthesis of new proteins.
pancreas, intestines, and liver. 10. Second messenger system. Water-soluble, nonsteroidal hormones-
● Hemochromatosis - Hemochromatosis is a disorder that interferes with protein, and peptide hormones- are unable to enter the target cells,
the body’s ability to breakdown iron, and results in too much iron being so instead, they bind to receptors situated on the target cell’s plasma
absorbed from the gastrointestinal tract. membrane and utilize a second messenger system.
● Hepatic Impairment - Liver failure is the inability of the liver to perform
its normal synthetic and metabolic function as part of normal physiology.
● Hepatic Venous Pressure Gradient (HVPG) - Currently, the most
commonly used parameter to directly measure portal pressure is the
Hepatic Venous Pressure Gradient (HVPG). HVPG represents the gradient
between pressures in the portal vein and the intra-abdominal portion of
inferior vena cava.
● Hepatitis B - Formerly called “serum hepatitis”, it is caused by the
hepatitis B virus (HBV). It is spread primarily through blood, unprotected
sex, shared needles, and from an infected mother to her newborn during
the delivery process. There is a safe vaccine for HBV.
● Hepatitis C - Formerly known as “non-A, non-B hepatitis”, it is caused by
the hepatitis C virus (HCV). It is spread through infected blood, primarily
in those who use illicit street drugs and those who received blood
transfusions prior to 1992 (the first year that a blood test for HCV became
available for screening the blood supply). There is no vaccine.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 27
● Thyroid-stimulating hormone (TSH). TSH, also called thyrotropin
hormone influences the growth and activity of the thyroid gland.
● Gonadotropic hormones. The gonadotropic hormones regulate the
hormonal activity of gonads (ovaries and testes).
● Follicles-stimulating hormone (FSH). FSH stimulates follicle
development in the ovaries; as the follicles mature, they produce
estrogen and eggs that are readied for ovulation; in men, FSH
stimulates sperm development by the testes.
● Luteinizing hormone (LH). LH triggers ovulation of an egg from the ovary
and causes the ruptured follicle to produce progesterone and some
estrogen; in men, LH stimulates testosterone production by the
interstitial cells of the testes.
Hormones of the Posterior Pituitary
The posterior pituitary is not an endocrine gland in the strict sense
because it does not make the peptide hormones it releases, but it simply
acts as a storage area for hormones made by hypothalamic neurons
● Oxytocin. Oxytocin is released in significant amount only during
childbirth and in nursing women; it stimulates powerful contractions
of the uterine muscle during labor, during sexual relations, and
during breastfeeding and also causes milk ejection (let-down reflex) in a
nursing woman.
● Antidiuretic hormone (ADH). ADH causes the kidneys to reabsorb more
water from the forming of urine; as a result, urine volume decreases
and blood volume increases; in larger amounts, ADH also increases
blood pressure by causing constriction of the arterioles, so it is
Anatomy of the Endocrine System sometimes referred to as vasopressin.
● Compared to other organs of the body, the organs of the endocrine
system are small and unimpressive, however, functionally the endocrine III. Thyroid Gland
organs are very impressive, and when their role in maintaining body
homeostasis is considered, they are true giants. - The thyroid gland is a hormone-producing gland that is familiar to most
people primarily because many obese individuals blame their
I. Hypothalamus overweight condition on their “glands” (thyroid).
● Location. The thyroid gland is located at the base of the throat,
- The major endocrine organs of the body include the pituitary, just inferior to the Adam’s apple, where it is easily palpated during
thyroid, parathyroid, adrenal, pineal and thymus glands, the pancreas, a physical examination.
and the gonads. ● Lobes. It is a fairly large gland consisting of two lobes joined by
● Hypothalamus. The hypothalamus, which is part of the nervous a central mass, or isthmus.
system, is also considered as a major endocrine organ because it ● Composition. Internally, the thyroid gland is composed of hollow
produces several hormones. It is an important autonomic nervous structures called follicles, which store a sticky colloidal material.
system and endocrine control center of the brain located inferior to ● Types of thyroid hormones. Thyroid hormone often referred to as the
the thalamus. body’s major metabolic hormone, is actually two active, iodine-
● Mixed functions. Although the function of some hormone-producing containing hormones, thyroxine or T4, and triiodothyronine or T3.
glands is purely endocrine, the function of others (pancreas and gonads) ● Thyroxine. Thyroxine is the major hormone secreted by the thyroid
is mixed- both endocrine and exocrine. follicles
● Triiodothyronine. Most triiodothyronine is formed at the target tissues
II. Pituitary Gland by conversion of the thyroxine to triiodothyronine.
- The pituitary gland is approximately the size of a pea. ● Function. Thyroid hormone controls the rate at which glucose is
“burned” oxidized, and converted to body heat and chemical energy; it
● Location. The pituitary gland hangs by a stalk from the inferior
is also important for normal tissue growth and development.
surface of the hypothalamus of the brain, where it is snugly
● Calcitonin. Calcitonin decreases blood calcium levels by causing
surrounded by the “Turk’s saddle” of the sphenoid bone.
calcium to be deposited in the bones; calcitonin is made by the so-
● Lobes. It has two functional lobes- the anterior pituitary glandular called parafollicular cells found in the connective tissues between
tissue) and the posterior pituitary (nervous tissue). the follicles.
IV. Parathyroid Gland
- The parathyroid glands are mostly tiny masses of glandular tissue.
● Location. The parathyroid glands are located on the posterior surface of
the thyroid gland.
● Parathormone. The parathyroids secrete parathyroid hormone (PTH) or
parathormone, which is the most important regulator of calcium
ion homeostasis of the blood; PTH is a hypercalcemic hormone
(that is, it acts to increase blood levels of calcium), whereas calcitonin is
a hypocalcemic hormone.; PTH also stimulates the kidneys and intestines
to absorb more calcium.
V. Adrenal Glands
- Although the adrenal gland looks like a single organ, it is structurally
and functionally two endocrine organs in one.
Hormones of the Anterior Pituitary Hormones of the Adrenal Cortex
There are several hormones of the anterior pituitary hormones that affect - The adrenal cortex produces three major groups of steroid
many body organs hormones, which are collectively called corticosteroids–
● Growth hormone (GH). Growth hormone is a general metabolic mineralocorticoids, glucocorticoids, and sex hormones.
hormone, however, its major effects are directed to the growth of ● Mineralocorticoids. The mineralocorticoids, primarily aldosterone, are
skeletal muscles and long bones of the body; it is a protein- sparing produced by the outermost adrenal cortex cell layer; mineralocorticoids
and anabolic hormone that causes amino acids to be built into proteins are important in regulating the mineral (or salt) content of the blood,
and stimulates most target cells to grow in size and divide. particularly the concentrations of sodium and potassium ions and
● Prolactin (PRL). Prolactin is a protein hormone structurally similar they also help in regulating the water and electrolyte balance in the
to growth hormone; its only known target in humans is the breast body.
because, after childbirth, it stimulates and maintains milk production ● Renin. Renin, am enzyme produced by the kidneys when the blood
by the mother’s breast. pressure drops, also cause the release of aldosterone by triggering a
● Adrenocorticotropic hormone (ACTH). ACTH regulates the endocrine series of reactions that form angiotensin II, a potent stimulator of
activity of the cortex portion of the adrenal gland. aldosterone release.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 28
● Atrial natriuretic peptide (ANP). ANP prevents aldosterone release, its ● Estrogen. Alone, the estrogens are responsible for the development
goal being to reduce blood volume and blood pressure. of sex characteristics in women at puberty; acting with progesterone,
● Glucocorticoids. The middle cortical layer mainly produces estrogens promote breast development and cyclic changes in the
glucocorticoids, which include cortisone and cortisol; glucocorticoids uterine lining (menstrual cycle).
promote normal cell metabolism and help the body to resist long-term ● Progesterone. Progesterone acts with estrogen to bring about
stressors, primarily by increasing blood glucose levels, thus it is the menstrual cycle; during pregnancy, it quiets the muscles of
said to be a hyperglycemic hormone; it also reduce pain and the uterus so that an implanted embryo will not be aborted and
inflammation by inhibiting some pain-causing molecules called helps prepare breast tissue for lactation.
prostaglandins. Hormones of the Testes
● Sex hormones. Both male and female sex hormones are produced by - The testes of the male are paired oval organs in a sac.
the adrenal cortex throughout life in relatively small amounts; ● Location. The testes are suspended in a sac, the scrotum, outside the
although the bulk of sex hormones produced by the innermost cortex pelvic cavity.
layer are androgens (male sex hormones), some estrogens (female sex ● Male sex hormones. In addition to male sex cells, or sperm, the
hormones), are also formed. testes also produce male sex hormones, or androgens, of which
Hormones of the Adrenal Medulla testosterone is the most important.
- The adrenal medulla, like the posterior pituitary, develops from a knot of ● Testosterone. At puberty, testosterone promotes the growth and
nervous tissue. maturation of the reproductive system organs to prepare the young
● Catecholamines. When the medulla is stimulated by sympathetic nervous man for reproduction; it also causes the male’s secondary sex
system neurons, its cells release two similar hormones, epinephrine, also characteristics to appear and stimulates male sex drive; Testosterone
called adrenaline, and norepinephrine (noradrenaline), into the is also necessary for the continuous production of sperm.
bloodstream; collectively, these hormones are referred to as Other Hormone-Producing Tissues and Organs
catecholamines. - Besides the major endocrine organs, pockets of hormone-producing cells
● Function. Basically, the Catecholamines increase heart rate, blood are found in fatty tissue and in the walls of the small intestine, stomach,
pressure, and blood glucose levels and dilate the small passageways kidneys, and heart- organs whose chief functions have little to do with
of the lungs; the catecholamines of the adrenal medulla prepare the hormone production.
body to cope with a brief or short-term stressful situation and cause the
so-called alarm stage of the stress response.
Placenta
VI. Pancreatic Islets - The placenta is a remarkable organ formed temporarily in the uterus of
pregnant women.
- The pancreas, located close to the stomach in the abdominal cavity, ● Function. In addition to its roles as the respiratory, excretory, and
is a mixed gland. nutrition delivery systems for the fetus, it also produces several
● Islets of Langerhans.The islets of Langerhans also called pancreatic islets, proteins and steroid hormones that help to maintain the pregnancy
are little masses of hormone-producing tissue that are scattered among and pave the way for delivery of the baby.
the enzyme-producing acinar tissue of the pancreas. ● Human chorionic gonadotropin. During very early pregnancy, a hormone
● Hormones. Two important hormones produced by the islet cells are called human chorionic gonadotropin (hCG) is produced by the
insulin and glucagon. developing embryo and then by the fetal part of the placenta; hCG
● Islet cells. Islet cells act as fuel sensors, secreting insulin and glucagon stimulates the ovaries to continue producing estrogen and progesterone
appropriately during fed and fasting states. so that the lining of the uterus is not sloughed off in the menses.
● Beta cells. High levels of glucose in the blood stimulate the release ● Human placental lactogen (hPL). hPL works cooperatively with
of insulin from the beta cells of the islets. estrogen and progesterone in preparing the breasts for lactation.
● Alpha cells. Glucagon’s release by the alpha cells of the islets is ● Relaxin. Relaxin, another placental hormone, causes the mother’s pelvic
stimulated by low blood glucose levels. ligaments and the pubic symphysis to relax and become more flexible,
● Insulin. Insulin acts on just about all the body cells and increases which eases birth passage.
their ability to transport glucose across their plasma membranes;
because insulin sweeps glucose out of the blood, its effect is said to PHYSIOLOGY OF THE ENDOCRINE SYSTEM
be hypoglycemic.
● Glucagon. Glucagon acts as an antagonist of insulin; that is, it helps - Although hormones have widespread effects, the major processes
to regulate blood glucose levels but in a way opposite that of insulin; they control are reproduction, growth, and development; mobilizing
its action is basically hyperglycemic and its primary target organ is the the body’s defenses against stressors; maintaining electrolyte, water,
liver, which it stimulates to break down stored glycogen into glucose and and nutrient balance of the blood; and regulating cellular metabolism
release the glucose into the blood. and energy balance.
The Chemistry of Hormones
VII. Pineal Gland - The key to the incredible power of the endocrine glands is the hormones
they produce and secrete.
- The pineal gland, also called the pineal body, is a small cone-shaped ● Hormones. Hormones may be defined as chemical substances that
gland. are secreted by endocrine cells into the extracellular fluids and regulate
● Location. The pineal gland hangs from the roof of the third ventricle of the metabolic activity of other cells in the body.
the brain. ● Classification. Although many different hormones are produced,
● Melatonin. Melatonin is the only hormone that appears to be secreted in nearly all of them can be classified chemically as either amino
substantial amounts by the pineal gland; the levels of melatonin rise and acid-based molecules (including proteins, peptides, and amines)
fall during the course of the day and night; peak levels occur at night and or steroids.
make us drowsy as melatonin is believed to be the “sleep trigger” that ● Steroid hormones. Steroid hormones (made from cholesterol) include
plays an important role in establishing the body’s day-night cycle. the sex hormones made by the gonads and hormones produced by the
adrenal cortex.
VIII. Thymus ● Amino acid-based hormones. All the others are nonsteroidal amino acid
- The thymus gland is large in infants and children and decreases in size derivatives.
throughout adulthood Mechanisms of Hormone Action
● Location. The thymus gland is located in the upper thorax, posterior to - Although the blood-borne hormones circulate to all the organs of
the sternum. the body, a given hormone affects only certain tissue cells or organs.
● Thymosin. The thymus produces a hormone called thymosin and ● Target cells. For a target cell to respond to the hormone, specific
others that appear to be essential for normal development of a special protein receptors must be present on its plasma membrane or in its
group of white blood cells (T-lymphocytes, or T cells) and the immune interior to which that hormone can attach; only when this binding occurs
response. can the hormone influence the workings of cells.
● Function of hormones. The hormones bring about their effects on,
IX. Gonads the body cells primarily by altering cellular activity- that is, by increasing
or decreasing the rate of a normal, or usual, metabolic process rather
- The female and male gonads produce sex hormones that are identical to than stimulating a new one.
those produced by adrenal cortex cells; the major difference are the ● Changes in hormone binding. The precise changes that follow
source and relative amount produced hormone binding depend on the specific hormone and the target cell
Hormones of the Ovaries type, but typically one or more of the following occurs:
- The female gonads or ovaries are a pair of almond-sized organs. 1) Changes in plasma membrane permeability or electrical state.
● Location. The female gonads are located in the pelvic cavity. 2) Synthesis of protein or certain regulatory molecules (such as
● Steroid hormones. Besides producing female sex cells, ovaries enzymes) in the cell.’
produce two groups of steroid hormones, estrogen, and progesterone. 3) Activation or inactivation of enzymes.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 29
4) Stimulation of mitosis. Prevention
5) Promotion of secretory activity. ● For patients who are obese (especially those with type 2 diabetes), weight
Control of Hormone Release loss is the key to treatment and the major preventive factor for the
- What prompts the endocrine glands to release or not release their development of diabetes.
hormones?
● Negative feedback mechanisms. Negative feedback mechanisms are the
chief means of regulating blood levels of nearly all hormones.
● Endocrine gland stimuli. The stimuli that activate the endocrine Complications of Diabetes
organs fall into three major categories- hormonal, humoral, and neural. ● Complications associated with diabetes are classified as acute and
● Hormonal stimuli. The most common stimulus is a hormonal chronic. Acute complications occur from short-term imbalances in blood
stimulus, in which the endocrine organs are prodded into action by glucose and include the following:
other hormones; for example, hypothalamic hormones stimulate the ● Hypoglycemia
anterior pituitary gland to secrete its hormones, and many anterior ● DKA
pituitary hormones stimulate other endocrine organs to release their ● HHNS
hormones into the blood. ● Chronic complications generally occur 10 to 15 years after the onset of
● Humoral stimuli. Changing blood levels of certain ions and nutrients may diabetes mellitus. The complications include the following:
also stimulate hormone release, and this is referred to as humoral ● Macrovascular (large vessel) disease: affects coronary, peripheral
stimuli; for example, the release of parathyroid hormone (PTH) by cells vascular, and cerebral vascular
of the parathyroid glands is prompted by decreasing blood calcium levels. ● Microvascular (small vessel) disease: affects the eyes (retinopathy)
● Neural stimuli. In isolated cases, nerve fibers stimulate hormone release, and kidneys (nephropathy); control blood glucose levels to delay
and the target cells are said to respond to neural stimuli; a classic or avoid onset of both microvascular and macrovascular
example is sympathetic nervous system stimulation of the adrenal complications
medulla to release norepinephrine and epinephrine during periods of ● Neuropathic disease: affects sensory motor and autonomic nerves
stress. and contributes to such problems as impotence and foot ulcers
Gerontologic Considerations
DIABETES MELLITUS ● Because the incidence of elevated blood glucose levels increases with
advancing age, elderly adults should be advised that physical activity that
● Diabetes mellitus is a group of metabolic disorders characterized by
is consistent and realistic is beneficial to those with diabetes. Advantages
elevated levels of blood glucose (hyperglycemia) resulting from defects
of exercise include a decrease in hyperglycemia, a general sense of well-
in insulin secretion, insulin action, or both. Three major acute
being, and better use of ingested calories, resulting in weight reduction.
complications of diabetes related to short-term imbalances in blood
Consider physical impairment from other chronic diseases when planning
glucose levels are hypoglycemia, diabetic ketoacidosis (DKA), and
an exercise regimen for elderly patients with diabetes.
hyperglycemic hyperosmolar nonketotic syndrome (HHNS).
Medical Management
● Long- term hyperglycemia may contribute to chronic microvascular
● The main goal of treatment is to normalize insulin activity and blood
complications (kidney and eye disease) and neuropathic complications.
glucose levels to reduce the development of vascular and neuropathic
Diabetes is also associated with an increased occurrence of
complications. The therapeutic goal within each type of diabetes is to
macrovascular diseases, including coronary artery disease (myocardial
achieve normal blood glucose levels (euglycemia) without hypoglycemia
infarction), cerebrovascular disease (stroke), and peripheral vascular
and without seriously disrupting the patient’s usual activities. There are
disease.
five components of management for diabetes: nutrition, exercise,
Types of Diabetes
monitoring, pharmacologic therapy, and education.
Type 1 (Formerly Insulin-Dependent Diabetes Mellitus)
● Primary treatment of type 1 diabetes is insulin.
- About 5% to 10% of patients with diabetes have type 1 diabetes. It is
● Primary treatment of type 2 diabetes is weight reduction.
characterized by destruction of the pancreatic beta-cells due to genetic,
● Exercise is important in enhancing the effectiveness of insulin.
immunologic, and possibly environmental (eg, viral) factors. Insulin
● Use oral hypoglycemic agents if diet and exercise are not
injections are needed to control the blood glucose levels.
successful in controlling blood glucose levels. Insulin injections
- Type 1 diabetes has a sudden onset, usually before the age of 30 years.
may be used in acute situations.
Type 2 (Formerly Non–Insulin-Dependent Diabetes Mellitus)
● Because treatment varies throughout the course because of
- About 90% to 95% of patients with diabetes have type 2 diabetes. It
changes in lifestyle and physical and emotional status as well as
results from a decreased sensitivity to insulin (insulin resistance) or from
advances in therapy, continuously assess and modify treatment
a decreased amount of insulin production.
plan as well as daily adjustments in therapy. Education is needed
- Type 2 diabetes is first treated with diet and exercise, and then with oral
for both patient and family.
hypoglycemic agents as needed.
Nutritional Management
- Type 2 diabetes occurs most frequently in patients older than 30 years
● Goals are to achieve and maintain blood glucose and blood pressure
and in patients with obesity
levels in the normal range (or as close to normal as safely possible) and
Gestational Diabetes Mellitus a lipid and lipoprotein profile that reduces the risk for vascular disease;
to prevent, or at least slow, the rate of development of chronic
● Gestational diabetes is characterized by any degree of glucose complications; to address individual nutrition needs; and to maintain the
intolerance with onset during pregnancy (second or third trimester). pleasure of eating by only limiting food choices when indicated by
● Risks for gestational diabetes include marked obesity, a personal history scientific evidence.
of gestational diabetes, glycosuria, or a strong family history of diabetes. ● Meal plan should consider the patient’s food preferences, lifestyle, usual
High-risk ethnic groups include Hispanic eating times, and ethnic and cultural background.
● Americans, Native Americans, Asian Americans, African Americans, and ● For patients who require insulin to help control blood glucose levels,
Pacific Islanders. It increases their risk for hypertensive disorders of consistency is required in maintaining calories and carbohydrates
pregnancy. consumed at different meals.
Clinical Manifestations ● Initial education addresses the importance of consistent eating habits,
● Polyuria, polydipsia, and polyphagia. the relationship of food and insulin, and the provision of an individualized
● Fatigue and weakness, sudden vision changes, tingling or numbness in meal plan. In-depth follow-up education then focuses on management
hands or feet, dry skin, skin lesions or wounds that are slow to heal, and skills, such as eating at restaurants; reading food labels; and adjusting the
recurrent infections. meal plan for exercise, illness, and special occasions.
● Onset of type 1 diabetes may be associated with sudden weight loss or Nursing Management
nausea, vomiting, or stomach pains. ● Nursing management of patients with diabetes can involve treatment of
● Type 2 diabetes results from a slow (over years), progressive glucose a wide variety of physiologic disorders, depending on the patient’s health
intolerance and results in long-term complications if diabetes goes status and whether the patient is newly diagnosed or seeking care for an
undetected for many years (eg, eye disease, peripheral neuropathy, unrelated health problem. Because all patients with diabetes must
peripheral vascular disease). Complications may have developed before master the concepts and skills necessary for long-term management and
the actual diagnosis is made. avoidance of potential complications of diabetes, a solid educational
● Signs and symptoms of DKA include abdominal pain, nausea, vomiting, foundation is necessary for competent self-care and is an ongoing focus
hyperventilation, and a fruity breath odor. Untreated DKA may result in of nursing care.
altered level of consciousness, coma, and death.
Assessment and Diagnostic Methods
● High blood glucose levels: fasting plasma glucose levels 126 mg/dL or
more, or random plasma glucose or 2-hour postload glucose levels more
than 200 mg/dL Hyperpituitarism
● Evaluation for complications
Definition
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 30
● Acromegaly is a rare disorder of excessive bone and soft tissue growth ● If these tests confirm acromegaly, the following may be done to locate
due to elevated levels of growth hormone. In young children, prior to the the tumor that is causing the disorder:
completed fusion and growth of bones, excessive growth hormone can ● Head CT Scan—a type of x-ray that uses a computer to make pictures of
cause a similar condition called gigantism. the inside of the brain and surrounding structures
● MRI Scan
Nursing Diagnosis
● Disturbed Body Image related to anxiety over thickened skin and
enlargement of face, hands, and feet.
● Ineffective Coping related to change in appearance.
● Disturbed Sensory Perception
● Disturbed Sleeping Pattern related to soft tissue swelling
● Fluid Volume Deficit
● Anxiety related to change in appearance
● Knowledge Deficit
Treatment
● Reduce production of GH to normal levels
● Stop and reverse the symptoms caused by over-secretion of GH
● Correct other endocrine abnormalities (thyroid, adrenal, sex organs)
● Reduce the tumor size
Surgery
● Surgical removal of the pituitary tumor, or other tumor, that is believed
to be causing acromegaly may be done. In most cases, this is the
preferred treatment.
Radiosurgery
● Radiosurgery is the use of highly focused external beams of radiation to
shrink the tumor. It is used most often in patients who do not respond to
conventional surgery or medications.
Radiation Therapy
Causes ● Radiation therapy is used in combination with either medical and/or
● In most cases, acromegaly is caused by over-secretion of growth hormone surgical treatment.
(GH) produced by a benign tumor of the pituitary gland. The pituitary Medication
gland is a small gland located at the base of the brain that produces many - Drugs may be given to reduce the level of GH secretion from the pituitary
hormones. In a small number of cases, malignant tumors of other organs gland. These include:
(pancreas, adrenal, lung) may be the source of excess GH ● Cabergoline (Dostinex)—given orally
Risk Factors ● Pergolide (Permax)—given orally
● Some rare cases of acromegaly are hereditary. ● Bromocriptine (Parlodel)—may be given before surgery to shrink tumor
● The average age of diagnosis is 40-45 years old. ● Octreotide (Sandostatin)—given by injections
Symptoms ● Pegvisomant—given by injections for patients not responding to other
● Symptoms usually develop very slowly over time. forms of treatment
● Acromegaly can cause serious complications and premature death if not - Medications must often be combined with other therapies to treat larger
treated. tumors affecting surrounding structures.
● In children, excess GH production causes elongation of the bones and Prevention
associated soft tissue swelling. If not treated, children with this disorder ● There are guidelines for preventing acromegaly.
can grow the height of 7-8 feet. ● Early diagnosis and treatment, however, will help prevent serious
● Symptoms and complications in adults may include the following: complications, some of which are irreversible.
○ Abnormally large growth and deformity of the:
■ Hands (rings longer fit) Hypopituitarism
■ Feet (need a bigger size shoe)
Definition
■ Face (protrusion of brow and lower jaw)
● Hypofunction of the pituitary gland (hypopituitarism) can occur due to
■ Jaw (teeth don't line up correctly when the mouth is
diseases of the gland or the hypothalamus.
closed)
● Hypopituitarism refers to the state of the anterior pituitary secretion of
■ Lips
several hormones, which is very low.
■ Tongue
● Hypopituitarism is hypersecretion of one or more anterior pituitary
○ Carpal tunnel syndrome
hormones
○ Skin changes, such as:
● Hypopituitarism is a condition that arises as a result of pituitary
■ Thickened, oily, and sometimes darkened skin
hypofunction. Definition of anterior pituitary hormones may occur from
■ Severe acne
3 pathways:
■ Excessive sweating and offensive body order due
1) Abnormalities in the gland that can damage the secretory cells.
enlargement of the sweat glands
2) Abnormalities within or adjacent to the pituitary stalk which can lead to
○ Deepening voice due enlarged sinuses, vocal cords, and soft
termination of the spread of the factors that originate from the
tissues of the throat
hypothalamus.
○ Fatigue and weakness in legs and arms
3) Abnormalities in the hypothalamus which may impair the release of the
○ Sleep apnea
regulator on the front hypofyse.
○ Arthritis and other joint problems especially in the jaw
Etiology
○ Hypothyroidism
- Hypopituitarism may occur due to a malfunction of the pituitary gland or
○ Enlargement of the liver, kidneys, spleen, heart, and/or other
hypothalamus. Cause concerns:
internal organs, which can lead to:
● Infection or inflammation by: fungal, pyogenic bacteria.
■ Diabetes
● Autoimmune diseases (autoimmune lymphoid pituitary)
■ High blood pressure
● Tumors, for example of a type of hormone-producing cells that can
■ Cardiovascular disease
interfere with the formation of one or another hormone arbitrarily.
● In women:
● Feedback from the target organ experiencing malfunctions. For example,
○ Irregular menstrual cycles
there will be a decrease in the secretion of TSH from the pituitary gland
○ Galactorrhea (abnormal production of breast milk) in 50% of
when the thyroid is diseased secrete excessive levels of HT.
cases
● Hypoxic necrotic (death due to lack of O2) pituitary or oxygenation can
● In men:
damage some or all of the hormone-producing cells. One of them
○ In about 50% of cases, impotence
sheehan syndrome, which occurs after maternal hemorrhage.
Clinical Manifestations
Diagnosis
● Headache and visual disturbances or signs of increased intracranial
● Blood tests will be done tmeasure the level of insulin-like growth factor
pressure.
(IGF-I), growth hormone releasing hormone (GHRH) , and other pituitary
● Overview of the production of growth hormone excess include
hormones.
acromegaly (large hands and feet as well as the tongue and jaw), profuse
● A glucose tolerance test may alsbe given tsee if the GH level drops—it will
sweating, hypertension and arthralgia (joint pain).
not drop in cases of acromegaly.
● Hyperprolactinemia : amenorrhea or oligomenorrhea, galactorrhea
(30 %), infertility in women, impotence in men.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 31
● Cushing syndrome : central obesity, hirsutism, striae, hypertension, ● Fasting plasma glucose test — a lab test that measures a person’s blood
diabetes mellitus, osteoporosis. glucose level after fasting or not eating anything for 10 to 12 hours.
● Growth hormone deficiency : (growt hormone = GH) growth disorders in Normal fasting blood glucose is less than 100 mg/dl for people who do
children. not have diabetes. A diagnosis of diabetes is made when two blood tests
● Gonadotropin deficiency : impotence, decreased libido, body hair loss in show that your fasting blood glucose level is greater than or equal to 126
men, amenorrhea in women. mg/dl.
● TSH deficiency : fatigue, constipation, dry skin laboratory picture of ● Fats —substances that help the body use some vitamins and keep the skin
hyperthyroidism. healthy. They are also the major way the body stores energy. In food,
● Corticotropin Deficiency : malaise, anorexia, fatigue is real, pale, the there are two types of fats; saturated and unsaturated.
symptoms are very severe for ordinary mild systemic disease, laboratory ● Gestational diabetes mellitus— a high blood glucose level that is
overview of the decline in adrenal function. discovered during pregnancy. As pregnancy progresses, there is an
● Vasopressin deficiency : polyuria, polydipsia, dehydration, unable to increased need for glucose for the developing baby. Additionally,
concentrate urine. hormone changes during pregnancy affect the action of insulin, resulting
Physical Examination in high blood glucose levels. Usually, blood glucose levels return to
1) Physical examination normal after childbirth. However, women who have had gestational
● Inspection : Observe the shape and size of the body, measuring diabetes are at increased risk of developing type 2 diabetes later in life.
weight and height, observe the shape and size of the breast, ● Glaucoma — an eye disease associated with increased pressure within
axillary and pubic hair growth in male clients, observe also the the eye. Glaucoma can damage the optic nerve and cause impaired vision
growth of facial hair (beard and mustache). and blindness.
● Palpation : Palpation of the skin, the woman usually becomes dry ● Glucagon — a hormone that raises the level of glucose (sugar) in the
and rough.Depending on the cause hypopituitary, other data blood. Glucagon is sometimes injected when a person has lost
should also be assessed as a concomitant of data as if the cause is consciousness (passed out) from a low blood sugar reaction. The injected
a tumor it is necessary to check the function of the cerebrum and glucagon helps raise the level of glucose in the blood.
cranial nerve function and the presence of headaches. ● Glucose — a simple sugar found in the blood. It is the body’s main source
2) Assess the physical changes also impact on the ability of clients to meet of energy; also known as dextrose.
their basic needs. ● Glucose tolerance test — a test that can be used to determine if a person
3) Supporting data of the diagnostic workup such as : has diabetes. The test is done in a lab or doctor’s office in the morning
● X-ray of cranium to see the dilation and erosion of the sella turcica before the person has eaten. First a sample of blood is taken. Then the
or . person drinks a liquid that has glucose (sugar) in it. Periodically, another
● Examination of blood serum : LH and FSH GH, prolactin, sample of blood is taken to see how the body processes the glucose in
aldosterone, testosterone, cortisol, androgens, which include test the blood.
stimulation of insulin tolerance test and thyroid releasing ● Human insulin — bio-engineered insulin that is very similar to insulin
hormone stimulation. made by your own body.
Complication ● Hyperglycemia — high blood sugar. Many things can cause
1) Cardiovascular. hyperglycemia. It occurs when the body does not have enough insulin or
● Hypertension. cannot use the insulin it does have.
● Thrombophlebitis. ● Hypoglycemia — low blood glucose. Hypoglycemia in people with
● Thromboembolism. diabetes is often caused by an imbalance in diabetes medications, food
● Acceleration aterosklerosis. intake, and/or activity levels.
2) Immunology ● Injection site rotation — changing the areas on the body where a person
● Increased risk of infection and disguise any signs of infection. injects insulin. If the same injection site is used over and over again,
3) Changes in the eye. hardened areas, lumps or indentations can develop under the skin which
● Glaucoma. keep the insulin from being used properly. These lumps or indentations
● Corneal lesions. are called lipodystrophies.
4) Musculoskeletal ● Injection sites — recommended places on the body where people can
● Muscle wasting. inject insulin. These sites include the back of the upper arm, the
● Poor wound healing. abdomen, the thighs and the buttocks.
● Osteoporosis with vertebral compression fractures, long bone ● Insulin — a hormone that helps the body use glucose for energy. The beta
pathologic fractures, aseptic necrosis of the femoral head. cells of the pancreas make insulin.
5) Metabolic. Changes in glucose metabolism of steroid withdrawal ● Insulin dependent diabetes — former term used for type 1 diabetes, also
syndrome. formerly called juvenile diabetes. .
6) Changes in appearance. ● Insulin pump — a small, computerized device that is worn on a belt , in a
● Such as the moon face (moon face). pocket, or under clothes. Most insulin pumps delivers insulin through a
● Weight gain. small, flexible tube inserted under the skin. It delivers a steady flow of
● Acne. insulin 24 hours a day, and on-demand doses programmed by the user
Nursing Diagnosis for Hypopituitarism for food or high blood sugar
1) Disturbed Body Image lated to changes in body structure and function ● Insulin receptors — areas on the outer part of a cell that allow insulin in
of the body due to deficiency of gonadotropin and growth hormone the blood to join or bind with the cell. When the cell and insulin bind
deficiency. together, the cell can take glucose from the blood and use it for energy.
2) Ineffective individual coping related to the chronicity of the disease ● Insulin resistance — when a person’s body will not allow insulin to work
condition. properly in the body. This condition can occur when a person is
3) Low Self-Esteem related to changes in body appearance. overweight, and it often improves when the person loses weight.
4) Disturbed Sensory perception (visual) related to impaired transmission ● Insulin shock — loss of consciousness as a result of severe hypoglycemia
of impulses as a result of suppression of tumor on the optic nerve. (low blood sugar).
5) Anxiety related to threat or change in health status. ● Lancet — a fine, sharp pointed needle for pricking the skin. Used in blood
6) Self care deficit related to the decrease in muscle strength. glucose monitoring.
7) Risk for impaired skin integrity (drought) related to declining hormonal ● Polydipsia — excessive thirst that lasts for long periods of time; may be a
levels. sign of diabetes.
● Polyphagia —excessive hunger and eating; may be a sign of diabetes.
TERMINOLOGIES People with polyphagia as a result of diabetes often lose weight even
● Acidosis — too much acid in the body. For a person with diabetes, though they are eating more than normal.
ketoacidosis is a type of acidosis. ● Polyunsaturated fat — a type of fat that comes from vegetables. used is
● Adult-onset diabetes — former term for type 2 diabetes, also formerly either not enough or doesn’t work properly in the body. As a result,
called noninsulin-dependent diabetes. glucose cannot get into the body’s cells for use as energy. This causes
● Albuminuria — more than normal amounts of a protein called albumin in blood glucose to rise.
the urine. Albuminuria may be a sign of kidney disease. ● Unit of insulin — the basic measure of insulin. U-100 is the most common
● Blood urea nitrogen (BUN) — waste product of the kidneys. Increased concentration of insulin. U-100 means that there are 100 units of insulin
BUN levels may indicate early kidney damage. per milliliter (ml) of liquid.
● Dawn phenomenon — a sudden rise in blood glucose levels in the early
morning hours. This is more common in people with type 1 diabetes than
type 2 diabetes.
● Diabetic ketoacidosis (DKA) — severe, untreated hyperglycemia (high
blood sugar) that needs emergency treatment. DKA happens when there
is not enough insulin. Ketoacidosis can lead to coma and even death.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 32
administer in the evening; rotate injection sites to prevent
WEEK 5: SYNDROME OF INAPPROPRIATE ANTIDIURETIC lipodystrophy).
HORMONE SECRETION, DIABETES INSIPIDUS & THYROID ● Clofibrate (Atromid-S), a hypolipidemic agent, has been found to have an
DISORDERS antidiuretic effect on patients who have some residual hypothalamic
vasopressin; chlorpropamide (Diabinese) and thiazide diuretics are also
used in mild forms of the disease because they potentiate the action of
vasopressin.
SYNDROME OF INAPPROPRIATE ANTIDIURETIC HORMONE ● Thiazide diuretics, mild salt depletion, and prostaglandin inhibitors
(ibuprofen [Advil, Motrin], indomethacin [Indocin], and aspirin) are used
SECRETION to treat the nephrogenic form of diabetes insipidus.
NURSING MANAGEMENT
● The syndrome of inappropriate antidiuretic hormone (SIADH) secretion
● Instruct patient and family members about follow-up care and
refers to excessive antidiuretic hormone (ADH) secretion from the
emergency measures.
pituitary gland even in the face of subnormal serum osmolality.
● Provide specific verbal and written instructions, including the actions and
● Patients with this disorder cannot excrete dilute urine. They retain fluids
adverse effects of all medications; demonstrate correct medication
and develop sodium deficiency (dilutional hyponatremia). SIADH is often
administration and observe return demonstrations.
of nonendocrine origin. The syndrome may occur in patients with
● Advise patient to wear a medical identification bracelet and to carry
bronchogenic carcinoma (malignant lung cells synthesize and release
medication information about this disorder at all times.
ADH).
● Other causes include severe pneumonia, pneumothorax, other disorders ANATOMY AND PHYSIOLOGY OF THE THYROID GLAND
of the lungs, and malignant tumors that affect other organs. Disorders of
the central nervous system (head injury, brain surgery or tumor, or
infection) are thought to produce SIADH by direct stimulation of the
pituitary gland. Some medications (vincristine, diuretics, phenothiazines,
tricyclic antidepressants) and nicotine have been implicated in SIADH.
MEDICAL MANAGEMENT
● SIADH is generally managed by eliminating the underlying cause if
possible and restricting fluid intake.
● Diuretics are used with fluid restriction to treat severe hyponatremia.
NURSING MANAGEMENT
● Monitor fluid intake and output, daily weight, urine and blood
chemistries, and neurologic status.
● Provide supportive measures and explanations of procedures and
treatments to assist patient to deal with this disorder.
DIABETES INSIPIDUS
● Diabetes insipidus is a disorder of the posterior lobe of the pituitary gland
that is characterized by a deficiency of antidiuretic hormone (ADH)
(vasopressin). Excessive thirst (polydipsia) and large volumes of dilute
urine characterize the disorder.
● It may occur secondary to head trauma, brain tumor, or surgical ablation
or irradiation of the pituitary gland. It may also occur with infections of
the central nervous system (meningitis, encephalitis, tuberculosis) or
with tumors (eg, metastatic disease, lymphoma of the breast or lung).
● Another cause of diabetes insipidus is failure of the renal tubules to
respond to ADH; this nephrogenic form may be related to hypokalemia,
hypercalcemia, and a variety of medications (eg, lithium, demeclocycline
[Declomycin]).
● The disease cannot be controlled by limiting fluid intake, because the
high-volume loss of urine continues even without fluid replacement.
Attempts to restrict fluids cause the patient to experience an insatiable
craving for fluid and to develop hypernatremia and severe dehydration.
CLINICAL MANIFESTATIONS
● Polyuria: Enormous daily output of very dilute urine (specific gravity 1.001
to 1.005). Primary diabetes insipidus may have an abrupt onset or an
insidious onset in adults.
● Polydipsia: Patient experiences intense thirst, drinking 2 to 20 L of fluid
daily, with a special craving for cold water.
Polyuria continues even without fluid replacement.
● If diabetes insipidus is inherited, the primary symptoms may begin at
birth; in adults, onset may be insidious or abrupt.
ASSESSMENT & DIAGNOSTIC FINDINGS
● Fluid deprivation test: Fluids are withheld for 8 to 12 hours until 3% to 5%
of the body weight is lost.
● Inability to increase specific gravity and osmolality of the urine during test
is characteristic of diabetes insipidus. ● A butterfly-shaped organ, the thyroid gland is located anterior to the
● Other diagnostic procedures include concurrent measurements of trachea, just inferior to the larynx. The medial region, called the isthmus,
plasma levels of ADH and plasma and urine osmolality as well as a trial of is flanked by wing-shaped left and right lobes. Each of the thyroid lobes
desmopressin (synthetic vasopressin) therapy and intravenous (IV) are embedded with parathyroid glands, primarily on their posterior
infusion of hypertonic saline solution. surfaces.
MEDICAL MANAGEMENT ● The tissue of the thyroid gland is composed mostly of thyroid follicles.
● The objectives of therapy are (1) to replace ADH (which is usually a long- The follicles are made up of a central cavity filled with a sticky fluid called
term therapeutic program), (2) to ensure adequate fluid replacement, colloid. Surrounded by a wall of epithelial follicle cells, the colloid is the
and (3) to identify and correct the underlying intracranial pathology. center of thyroid hormone production, and that production is dependent
Nephrogenic causes require different management approaches on the hormones' essential and unique component: iodine.
PHARMACOLOGIC THERAPY ● The thyroid gland is located in the neck where it wraps around the
● Desmopressin (DDAVP), administered intranasally, one or two trachea. (a) Anterior view of the thyroid gland. (b) Posterior view of the
administrations daily to control symptoms. thyroid gland. (c) The glandular tissue is composed primarily of thyroid
● Intramuscular administration of ADH (vasopressin tannate in oil) every 24 follicles. The larger parafollicular cells often appear within the matrix of
to 96 hours to reduce urinary volume (shake vigorously or warm; follicle cells.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 33
in nutrient breakdown and the use of oxygen to produce ATP. In addition,
SYNTHESIS AND RELEASE OF THYROID HORMONES Ta and T4 initiate the transcription of genes involved in glucose oxidation.
Although these mechanisms prompt cells to produce more ATP, the process
is Inefficient, and an abnormally increased level of heat is released as a
byproduct of these reactions. This so called calorigenic effect (calor- =
"heat") raises body temperature.
● Adequate levels of thyroid hormones are also required for protein synthesis
and for fetal and childhood tissue development and growth. They are
especially critical for normal development of the nervous system both in
utero and in early childhood, and they continue to support neurological
function in adults. As noted earlier, these thyroid hormones have a complex
● Hormones are produced in the colloid when atoms of the mineral iodine
attach to a glycoprotein, called thyroglobulin, that is secreted into the
colloid by the follicle cells. The following steps outline the hormones'
assembly:
1. Binding of TSH to its receptors in the follicle Left inferior thyroid
cells of the thyroid gland causes the cells to artery actively
transport iodide ions (I-) across their cell membrane. from the
bloodstream into the Fromleftsubclaviar cytosol. As a result, the
concentration of iodide ions "trapped" in the follicular cells is many
times higher than the concentration in the bloodstream.
2. Iodide ions then move to the lumen of the follicle cells that border
the colloid. There, the ions undergo oxidation (their negatively
charged electrons are removed). The oxidation of two iodide ions
(2 I-) results in iodine (12), which passes through the follicle cell
membrane into the colloid.
3. In the colloid, peroxidase enzymes link the iodine to the tyrosine
amino acids in thyroglobulin to produce two intermediaries: a
tyrosine attached to one iodine and a tyrosine attached to two
iodines. When one of each of these intermediaries is linked by
covalent bonds, the resulting compound is triiodothyronine (T3), a
thyroid hormone with three iodines. Much more commonly, two
copies of the second intermediary bond, forming
tetraiodothyronine, also known as thyroxine (T4), a thyroid
hormone with four iodines.
● These hormones remain in the colloid center of the thyroid follicles until
TSH stimulates endocytosis of colloid back into the follicle cells. There,
lysosomal enzymes break apart the thyroglobulin colloid, releasing free
T3 and Ta, which diffuse across the follicle cell membrane and enter the
bloodstream.
● In the bloodstream, less than one percent of the circulating T3 and Ta
remains unbound. This free Ts and T4 can cross the lipid bilayer of cell
membranes and be taken up by cells. The remaining 99 percent of
circulating T3 and T4 is bound to specialized transport proteins called ● Interrelationship with reproductive hormones, and deficiencies can
thyroxine-binding globulins (TBGs), to albumin, or to other plasma
proteins. This "packaging" prevents their free diffusion into body cells. influence libido, fertility, and other aspects of reproductive function. Finally,
When blood levels of T3 and T4 begin to decline, bound T3 and T4 are thyroid hormones increase the body's sensitivity to catecholamines
released from these plasma proteins and readily cross the membrane of (epinephrine and norepinephrine) from the adrenal medulla by
target cells. T is more potent than T4, and many cells convert T4 to T3
upregulation of receptors in the blood vessels. When levels of T3 and T4
through the removal of an iodine atom.
hormones are excessive, this effect accelerates the heart rate, strengthens
REGULATION OF TH SYNTHESIS the heartbeat, and increases blood pressure. Because thyroid hormones
regulate metabolism, heat production, protein synthesis, and many other
● The release of T3 and T4 from the thyroid gland is regulated by thyroid-
body functions, thyroid disorders can have severe and widespread
stimulating hormone (TSH). As shown in Figure 2, low blood levels of T3 and
consequences.
T4 stimulate the release of thyrotropin-releasing hormone (TRH) from the
hypothalamus, which triggers secretion of TSH from the anterior pituitary. HYPERTHYROIDISM
In turn, TSH stimulates the thyroid gland to secrete T3 and T4. The levels of
TRH, TSH, T, and T4 are regulated by a negative feedback system in which
increasing levels of Ts and T4 decrease the production and secretion of TSH.
FUNCTIONS OF THYROID HORMONES
● The thyroid hormones, Ta and Ta, are often referred to as metabolic
hormones because their levels influence the body's basal metabolic rate,
the amount of energy used by the body at rest. When Ta and T4 bind to
intracellular receptors located on the mitochondria, they cause an increase
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 34
9. Smooth, soft skin and hair
10. Nervousness and fine tremors of hands
11. Personality changes
12. Irritability and agitation
13. Mood swings
14. Oligomenorrhea (Irregular menstrual periods in women)
COMPLICATIONS
● Thyroid crisis (storm), also called thyrotoxicosis, is a sudden worsening of
hyperthyroidism symptoms that may occur with infection or stress. Fever,
decreased mental alertness, and abdominal pain may occur.
● Immediate hospitalization is needed.
● Other complications related to hyperthyroidism include:
○ Heart-related complications including:
○ Rapid heart rate
○ Congestive heart failure
○ Atrial fibrillation
○ Increased risk for osteoporosis, if hyperthyroidism is present for
a long time
○ Surgery-related complications, including:
○ Scarring of the neck
○ Hoarseness due to nerve damage to the voice box
● Hyperthyroidism is a hyperthyroid state hypersecretion resulting from ○ Low calcium level due to damage to the parathyroid glands
thyroid hormones (T3 and T4). (located near the thyroid gland)
● Hyperthyroidism is characterized by an increased rate of body ○ Treatments for hypothyroidism, such as radioactive iodine,
metabolism. A common cause is Graves' disease, also known as toxic surgery, and medications to replace thyroid hormones can have
diffuse goiter. Clinical manifestations are referred to as thyrotoxicosis. complications.
CAUSES PRIMARY NURSING DIAGNOSIS
● Graves' disease has an autoimmune derivation and is caused by ● Activity intolerance related to exhaustion and fatigue
circulating anti-TSH autoantibodies that displace TSH from the thyroid ● Diagnostic Evaluation
receptors and mimic TSH by activating the TSH receptor to release ● Thyroid-stimulating hormone (TSH) assay reveals a decrease in result
additional thyroid hormones. (normal TSH: 0.5-1.5 mU/L).
● Graves' disease is also associated with Hashimoto's disease, a chronic ● Elevation of thyroid hormones decreased TSH secretion by negative
inflammation of the thyroid gland that usually causes hypothyroidism but feedback.
can also cause symptoms similar to those of Graves' disease. ● Elevated Thyroxine (T4) radioimmunoassay (normal values: 5.0-12.0
● Thyrotoxicosis has several different pathophysiological causes, including ug/dL). Elevation reflects overproduction of thyroid hormones; monitors
autoimmune disease, functioning thyroid adenoma, and infection. response to therapy.
ASSESSMENT ● Elevated Tri-iodothyronine (T3) radioimmunoassay (normal values: 80-
230 ng/dL). Elevation reflects overproduction of thyroid hormones.
● Other Tests: 24-hr radioactive iodine uptake; thyroid autoantibodies;
antithyroglobulin; electrocardiogram (ECG)
MEDICAL MANAGEMENT
● Treatment is directed toward reducing thyroid hyperactivity for
symptomatic relief and removing the cause of complications.
● Three forms of treatment are available:
● Irradiation involving the administration of 1311 or 123l for destructive
effects on the thyroid gland
● Pharmacotherapy with antithyroid medications
● Surgery with the removal of most of the thyroid gland
RADIOACTIVE IODINE (1311)
● 1311 is given to destroy the overactive thyroid cells (most common
treatment in the elderly).
● 131| is contraindicated in pregnancy and nursing mothers because
radioiodine crosses the placenta and is secreted in breast milk.
PHARMACOTHERAPY
● The objective of pharmacotherapy is to inhibit hormone synthesis or
release and reduce the amount of thyroid tissue.
● The most commonly used medications are propylthiouracil (Propacil,
PTU) and methimazole (Tapazole)
until patient is euthyroid.
● Maintenance dose is establish, followed by gradual withdrawal of the
medication over the next several months.
● Antithyroid drugs are contraindicated in late pregnancy because of a risk
for goiter and cretinism in the fetus.
● Thyroid hormone may be administered to put the thyroid to rest.
ADJUNCTIVE THERAPY
● Potassium iodide, Lugol's solution, and saturated solution of potassium
iodide (SKI) may be added.
● Beta- adrenergic agents may be used to control the sympathetic nervous
system, effects that occur in hyperthyroidism; for example, propranolol
is used for nervousness, tachycardia, tremor, anxiety, and heat
intolerance
SURGERY
● Surgical treatment with thyroidectomy is no longer the preferred choice
of therapy for Graves' disease but is an alternative therapeutic approach
in some situations. In particular, it is used for patients who cannot
1. Enlarged thyroid gland (goiter) tolerate antithyroid drugs, have significant ophthalmopathy, have large
2. Palpatations, cardiac dysrhythmias, such as tachycardia or atrial goiters, or cannot undergo radioiodine therapy.
fibrillation PHARMACOLOGIC HIGHLIGHTS
3. Protruding eyeballs (exophthalmos) possibly present ● Propylthiouracil (PTU) an antithyroid agent is given to return the patient
4. Hypertension to the euthyroid (normal) state.
5. Heat intolerance ● PTU inhibits use of iodine by thyroid gland; blocks oxidation of iodine and
6. Diaphoresis inhibits thyroid hormone synthesis
7. Weight loss
8. Diarrhea
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 35
● Methimazole (Tapazole) an antithyroid agent is given to return the ● Iodine deficiency or excess. Imbalance in the iodine levels in the body
patient to the euthyroid (normal) state by inhibiting use of iodine by also affects the thyroid gland.
thyroid gland. ● Autoimmune or Hashimoto's thyroiditis, in which the immune system
● Other Drugs: Beta-adrenergic blockers, corticosteroids, radioactive iodine attacks the thyroid gland, is the most common example of this.
NURSING INTERVENTIONS ● Some women develop hypothyroidism after pregnancy (often referred to
● Provide adequate rest. as "postpartum thyroiditis").
● Administer sedatives as prescribed
● Provide a cool and quiet environment.
● Obtain weight daily.
● Provide a high-calorie diet.
● Avoid the administration of stimulants.
● Administer antithyroid medications (propylthiouracil [PTU]) that block
thyroid synthesis, as prescribed.
● Administer iodine preparations that inhibit the release of thyroid
hormone as prescribed.
● Administer propranolol (INderal) for tachycardia as prescribed.
● Prepare the client for radioactive iodine therapy, as prescribed, to
destroy thyroid cells.
● Prepare the client for thyroidectomy if prescribed.
DOCUMENTATION GUIDELINES
● Physical findings: Cardiovascular status (resting pulse, blood pressure,
presence of angina or palpitations), bowel activity, edema, condition of
skin, and activity tolerance
● Physical findings: Hypermetabolism, eye status, heat intolerance, activity
level Response to medications, skin care regimen, nutrition, body weight,
comfort
● Psychosocial response to changes in bodily function, including mental
acuity, behavioral patterns, emotional stability
DISCHARGE AND HOME HEALTHCARE GUIDELINES
● DISEASE PROCESS. Provide a clear explanation of the role of the thyroid
gland, the disease process, and the treatment plan. Explain possible side
effects of the treatment.
● MEDICATIONS. Be sure that the patient understands all medications,
including the dosage, route, action, adverse effects, and the need for any
laboratory monitoring of thyroid medications. If patients are taking
propylthiouracil or methimazole, encourage them to take the CLINICAL MANIFESTATIONS
medications with meals to limit gastric irritation. If the patient is taking The signs and symptoms of hypothyroidism include:
an iodine solution, mix it with milk or juice to limit gastric irritation and ● Extreme fatigue. Extreme fatigue makes it difficult for the person to
have the patient use a straw to limit the risk of teeth discoloration. complete a full day's work or participate in usual activities.
● COMPLICATIONS. Have the patient report any signs and symptoms of ● Menstrual disturbances. Menorrhagia or amenorrhea may also occur.
thyrotoxicosis immediately: rapid heart rate, palpitations, perspiration, ● Increase in weight. The patient usually begins to gain weight even
shakiness, tremors, difficulty breathing, nausea, vomiting. Teach the without an increase in the food intake.
patient to report increased neck swelling, difficulty swallowing, or weight ● Cold intolerance. The patient often complains of being cold even in a
loss. warm environment.
● Thick skin. The skin becomes thickened because of an accumulation of
HYPOTHYROIDISM mucopolysaccharides in the subcutaneous tissues.
PREVENTION
● Thyroid deficiency can affect all body functions and can range from mild, Prevention of hypothyroidism can be achieved with the following:
subclinical forms to advanced forms. ● Increase in iodine intake. Iodine intake is the foremost prevention
● Hypothyroidism results from suboptimal levels of thyroid hormone. strategy in hypothyroidism.
● Hypothyroidism also commonly occurs in patients with previous ● Early detection. Undergoing thyroid tests after a thyroid surgery or
hypothyroidism that has been treated with radioiodine or antithyroid therapy could result in early detection and prompt treatment of
medications or thyroidectomy. hypothyroidism.
● The term myxedema refers to the accumulation of mucopolysaccharides COMPLICATIONS
in subcutaneous and other interstitial tissues. Hypothyroidism can be a life-threatening disease if left unchecked.
CLASSIFICATION ● Myxedema coma. This is the decompensated state of severe
The types of hypothyroidism are classified according to their causes: hypothyroidism in which the patient is hypothermic and unconscious.
● Central hypothyroidism. There is a failure of the pituitary gland, the ASSESSMENT AND DIAGNOSTIC FINDINGS
hypothalamus, or both to stimulate production of thyroid hormones. Hypothyroidism can be detected in many ways.
● Secondary or pituitary hypothyroidism. The cause is entirely a pituitary ● Physical examination. The thyroid gland is inspected and palpated
disorder in secondary hypothyroidism. routinely in all patients.
● Tertiary or hypothalamic hypothyroidism. This refers to the cause as a ● Serum thyroid-stimulating tests. Measurement of the serum TSH
disorder of the hypothalamus resulting in inadequate secretion of TSH concentration is the single best screening test of thyroid function because
due to decreased stimulation of TRH. of its high sensitivity.
● The thyroid disorder is already present at birth in cretinism. ● Serum T3 and T4. Measurement of total T3 or T4 includes protein-bound
STATISTICS AND EPIDEMIOLOGY and free hormone levels that occur in response to TSH secretion.
● Hypothyroidism occurs in specific individuals at different instances. ● Thyroid antibodies. Results of testing by immunoassay techniques for
● Hypothyroidism occurs most frequently in older women. antithyroid antibodies are positive in Hashimoto's thyroiditis (100%).
● There is an increased incidence of thyroid cancer in men who have MEDICAL MANAGEMENT
undergone radiation therapy for head and neck cancer. The primary objective in the management of hypothyroidism is to restore a
● More than 95% of patients with hypothyroidism have primary or thyroidal normal metabolic state by replacing the missing hormone
hypothyroidism. ● Pharmacologic therapy. Synthetic levothyroxine is the preferred
CAUSES preparation for treating hypothyroidism and suppressing nontoxic
Several diseases and factors could cause hypothyroidism. goiters.
● The most common CAUSE of hypothyroidism is inflammation of the ● Prevention of cardiac dysfunction. As long as metabolism is subnormal
thyroid gland, which damages the gland's cells. and the tissues require relatively little oxygen, a reduction in the blood
● Autoimmune diseases. The most common cause of hypothyroidism in supply is tolerated without overt symptoms of coronary artery disease.
adults is autoimmune thyroiditis or Hashimoto's disease. ● Supportive therapy. Oxygen saturation levels should be monitored; fluids
● Atrophy of the thyroid gland. The thyroid gland shrinks in size as a result should be administered cautiously; application of external heat must be
of aging. avoided, and oral thyroid hormone therapy should be continued.
● Therapy hyperthyroidism. Therapies for such as radioactive iodine and NURSING MANAGEMENT
thyroidectomy could also cause hypothyroidism. Nursing care for a patient with hypothyroidism includes the following:
● Medications such as lithium, iodine compounds and antithyroid NURSING ASSESSMENT
medications could decrease production of TSH ● Assessment of the patient with hypothyroidism should include:
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 36
● Assessment of the thyroid from an interior or posterior position. ● Calcitonin level: a normal cell produced by the body which helps regulate
● Auscultation of the lobes of the thyroid gland using the diaphragm of the the balance of calcium between the blood and bones. When tc patients
stethoscope if there are abnormalities palpated. prove to be cancer free, it is likely they will not have a 'normal' calcitonin
● Assess thyroid gland for firmness (Hashimoto's) or tenderness level. The docs don't know why this is. The goal, then, is not to get back
(thyroiditis). to the 'norm', but to level out. If you happen to get back to 'norm,' that's
DIAGNOSIS great; it's also very unusual.
Based on the assessment data, the nursing diagnoses appropriate for a patient ● CAT: Abbreviation for computerized axial tomography.
with hypothyroidism are: ● C-cell: have nothing to do with thyroid functions; they just happen to
● Activity intolerance related to fatigue and depressed cognitive process. reside there. Among other things, they produce a normal hormone called
● Risk for imbalanced body temperature related to cold intolerance. "calcitonin," which helps regulate the balance of calcium between your
● Constipation related to depressed gastrointestinal function. blood and bones.
● Ineffective breathing pattern related to depressed ventilation. ● Diffuse toxic goiter: Hyperthyroidism.
● Disturbed thought processes related to depressed metabolism and ● Endo: see endocrinologist.
altered cardiovascular and respiratory status. ● Endocrinologist: One who specializes in endocrinology, A specialist who
PLANNING & GOALS studies the endocrine glands, these include the thyroid gland, parathyroid
To achieve a successful nursing care plan, the following goals should be glands, the pancreas, the adrenal gland, and the pituitary gland.
realized: ● Euthyroid: normal thyroxine level condition, thyroid hormone level in
● Increase in participation in activities. normal balance.
● Increase in independence. ● Follicular thyroid cancer: The normal thyroid gland is made up of sphere-
● Maintenance of normal body temperature. shaped structures called follicles. When a thyroid cancer arises from the
● Return of normal bowel function. cells which normally make up these follicles, the cancer is called follicular
● Improve respiratory status. cancer.
● Maintenance of normal breathing pattern. ● Goiter: a chronic enlargement of the thyroid gland, not due to a
● Improve thought processes. neoplasm, occurring endemically in certain localities, especially
NURSING INTERVENTIONS mountainous regions, and sporadically elsewhere.
Nursing interventions for a patient with hypothyroidism include the following: ● Graves: is the type of hyperthyroidism caused by a generalized
● Promote rest. Space activities to promote rest and exercise as tolerated. overactivity of the entire thyroid gland. It is also called "diffuse toxic
● Protect against coldness. Provide extra layer of clothing or extra blanket. goiter,", diffuse because because the entire thyroid gland is involved in
● Avoid external heat exposure. Discourage and avoid the use of external the disease process; "toxic" because the patient appears hot and flushed,
heat source. as if feverish due to an infection; and "goiter" because the thyroid gland
● Mind the temperature. Monitor patient's body temperature. enlarges in this condition. One potential symptom is that the eyes may
● Increase fluid intake. Encourage increased fluid intake within the limits appear enlarged due to the elevation of the upper eyelids.
of fluid restriction. ● Hashimoto's struma: also referred to as Reidel's struma, chronic
● Provide foods high in fiber. thyroiditis.
● Manage respiratory symptoms. Monitor respiratory depth, rate, pattern, ● Hyperthyroidism: The term used to refer to any condition in which there
pulse oximetry, and ABG. is too much thyroid hormone in the body. This most commonly results
● Pulmonary exercises. Encourage deep breathing, coughing, and use of from a generalized over-activity of the entire thyroid gland, a condition
incentive spirometry. also known as diffuse toxic goiter or Graves' disease. Common symptoms
● Orient to present surroundings. Orient patient to time, place, date, and may include nervousness, irritability, increased perspiration, thinning of
events around him or her. your skin, fine brittle hair, and muscular weakness especially involving the
EVALUATION upper arms and thighs. Your hands may shake and your heart may race.
A successful nursing care plan has achieved the following goals: Your bowel movements may increase in frequency. though diarrhea is
● Increased participation in activities. uncommon.
● Increased independence. ● Hypothyroidism: a condition in which the amount of thyroid hormones
● Maintained normal body temperature. in the body is below normal. This is the most common form of thyroid
● Return of normal bowel function. function abnormality, and is far more common than an overactive
● Improved respiratory status. thyroid. Symptoms include feeling run down, slow, depressed, cold, tired,
● Maintained normal breathing pattern. and you may lose interest in normal daily activities. Other symptoms may
● Improved thought processes. include dryness and brittleness of the hair, dry and itchy skin,
DISCHARGE & HOME CARE GUIDELINES constipation, muscle cramps, and increased menstrual flow in women.
At the completion of the home care instruction, the patient or caregiver will be ● Levothroid: drug; different brands of the thyroid hormone T4 or levo-
able to: thyroxine.
● Medication compliance. State that compliance to medical regimen is life- ● Levoxyl: drug; different brands of the thyroid hormone T4 or levo-
long. thyroxine.
● Cold intolerance. State the need to avoid extreme cold temperature until ● MTC: medullary thyroid cancer.
condition is stable. ● Postpartum thyroiditis: An inflammation of the thyroid gland which
● Follow-up visits. State the importance of regular follow-up visits with normally occurs after the birth of a child, for reasons unknown normally
health care provider. after the second or later birth. It is presumedly cause by antibodies
● Weight reduction. Identify strategies for weight reduction and (proteins) in the body which attack and damage the thyroid gland. This is
prevention of constipation such as high-fiber, low-calorie intake and a common disorder which frequently goes unrecognized.
adequate fluid intake. ● Radioactive iodine: usually administered in the form of a capsule or in
DOCUMENTATION GUIDELINES water (it is odorless and tasteless), the Radioactive iodine is quickly take
● The focus of documentation should include: up by the overactive thyroid cells. The results is that the thyroid shrinks
● Level of activity. in size, the thyroid hormone production falls, and blood levels return to
● Vital signs before, during, and after activity. normal with restoration of good health. Occasionally a second treatment
● Record of core temperature, initially and prn. is given to further control the thyroid hormone output. After
● Results of laboratory and diagnostic studies. administration your Nuclear Medicine technician will usually monitor the
● Usual and current bowel pattern, duration of the problem, and individual amount of intake by the thyroid (scanning), and looking for hot spots or
contributing factors. glows.
● Characteristics of stool. ● Thyroglobulin: (1) iodoglobulin; thyroprotein; a thyroid hormone-
● Respiratory pattern, breath sounds, and use of accessory muscles. containing protein, usually stored in the colloid within the thyroid
● Plan of care. follicles; biosynthesis of thyroid hormone entails iodination of the
● Teaching plan. tyrosine moieties of this protein and the combination of two
● Response to interventions, teaching, and actions performed. iodotyrosines to form thyroxine, the fully iodinated thyronine; secretion
● Attainment or progress toward desired outcomes. of thyroid hormone requires proteolytic degradation of thyroglobulin,
● Modifications to plan of care. with the attendant release of free hormone. (2) A substance obtained by
● Long term needs. the fractionation of thyroid glands from the hog, Sus scrofa, containing
not less than 0.7% of total iodine; used as a thyroid hormone in the
TERMINOLOGIES treatment of hypothyroidism.
● Antithyroid agents: Drugs; methamazole (Tapazole) or Propylthiouracil ● Thyroid: (1) Resembling a shield; denoting a gland (glandula thyroidea)
(PTU), drugs used to make it more difficult for iodine to get into your and a cartilage of the larynx (cartilago thyroidea) having such a shape. (2)
thyroid gland. The cleaned, dried, and powdered thyroid gland obtained from one of the
● Beta adrenergic blocking agents: drugs which block the action of the domesticated animals used for food and containing 0.17 to 0.23% of
thyroid hormone on your body.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 37
iodine; used in the treatment of cretinism and myxedema, in certain cases
of obesity, and in skin disorders.
● Thyroiditis: inflammation of the thyroid gland.
● Thyroid storm: thyrotoxic crisis.
● Thyroidectomy: The surgical removal of part or all of the thyroid gland.
● Thyroxine: The hormone produced by the thyroid gland.
NCMB 315 CU13 THYROID DISORDERS
Thyroid Gland: ● Reflex Testing (Kinemometry)
● Secretes the following hormones: ﹘ Tendon of Achilles Reflex (TAR)
● T3 (Triidothyronine)
- Metabolism and growth
● T4 (Thyroxine, tetra iodothyronine)
- Catabolism and body heat production
● Thyrocalcitonin
- bring down the blood Ca++ level
Diagnostic Tests:
● T3/ T4 levels
- ↑ level: hyperthyroidism
- ↓ level: hypothyroidism
● PBI (Protein-bound Iodine) GOITER
﹘ Preparation:
○ No foods, drugs, test dyes with iodine 7-10 days before the ● Enlargement of the thyroid gland associated with hyperthyroidism,
test hypothyroidism or euthyroidism
● RAIU (Radioactive Iodine Uptake) ● A hyperthyroid goiter is called toxic goiter
﹘ Tracer dose of I131 is used P.O. & at 2°, 6°, and 24° exposure to
scintillation camera is done
﹘ No foods, drugs, test dyes with iodine 7-10 days before the test,
temporarily discontinue contraceptive pills (these may metabolic
rate)
﹘ Result:
○ ↑ iodine uptake: hyperthyroidism
○ ↓ iodine uptake: hypothyroidism
Hyperthyroidism (Thyrotoxicosis)
● Thyroid Scan ﹘ Grave’s Disorder
﹘ Radioisotope Iodine is injected IV ﹘ Parry’s Disorder
﹘ Exposure to scintillation camera ﹘ Basedow’s Disorder
﹘ Exophthalmic Goiter
﹘ Toxic Diffuse Goiter
● common in female, below 40 y/o
● Causes:
- Severe emotional stress
- Autoimmune Disorder
- Thyroid inflammation
● Hyperthyroidism: Assessment Findings
- Restlessness, nervousness, irritability, agitation, fine tremors,
tachycardia, hypertension, voracious appetite to eat, weight loss,
diaphoresis, diarrhea, heat intolerance, amenorrhea, fine silky hair,
● FNB (Fine Needle Biopsy) pliable nails
﹘ Cytology (detection of malignant cells) ● EXOPHTHALMOS
- Due to accumulation of fluids at the fat-pads behind the eyeballs
- It can lead to corneal ulceration, opthalmitis, blindness
● BMR (Basal Metabolic Rate)
﹘ Measures O2 consumption at the lowest cellular activity
﹘ Oxygen uptake is measured as an indirect measurement of
metabolic rate
﹘ increased utilization O2 (hyperthyroid) ● DERMOPATHY
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 38
- Warm, flushed sweaty skin
- Thickened hyper-pigmented skin at the pretibial area
- Dexamethasone
○ inhibit the action of thyroid hormones
○ prevent the conversion of T4 to T3 in the peripheral tissues
● Hyperthyroidism: Management
- Rest (non-stimulating cool environment)
- Diet
○ HIGH Calorie, HIGH protein; vitamin and mineral supplement
○ Increased fluid intake (if with diarrhea)
○ Replace F&E losses
○ Avoid stimulants like coffee, tea and nicotine
- Promote safety
- Protect the eyes - Radiation therapy (Iodine131)
○ Artificial tears at regular intervals ○ Need isolation for few days; body secretions are radioactive
○ Wear dark sunglasses when going out under the sun contaminated
● Pharmacotherapy ○ NOT recommended in pregnant women because of potential
- ß-blockers: Propranolol teratogenic effects. Pregnancy should be delayed for 6
- Ca++ channel blockers months after therapy
○ These drugs are given to control tachycardia and HPN - Surgery
○ Subtotal Thyroidectomy- Usually about 5/6 of the gland is
removed
- Iodides : Lugol’s solution
○ SSKI (Saturated Solution of Potassium Iodide) ● Pre-op Care
○ Are given to inhibit release of thyroid hormone ○ Promote euthyroid state
○ Mix with fruit juice with ice or glass of water to improve its - Control of thyroid disturbance
palatability - Stable VS
○ Provide drinking straw to prevent permanent staining of teeth ○ Administer Iodides as ordered
- Side effects: - To reduce the size & vascularity of thyroid gland, thereby
○ Allergic reaction, Increased salivation, colds prevent post-op hemorrhage and thyroid crisis
○ ECG
- Heart failure/ cardiac damage results from HPN/ tachycardia
● Position: Semi-fowler’s with head, neck & shoulder erect
● Prevent Hemorrhage: ice collar over the neck
● Keep tracheostomy set available for the first 48° post-op
● Ask the patient to speak every hour (to assess for recurrent
laryngeal nerve damage)
● Keep Ca++ gluconate readily available
- Tetany occurs if hypocalcemia is present. This may be
secondary to the removal of the parathyroid gland
- Thioamides ● Monitor Body Temperature: hyperthermia is an initial sign of
○ PTU (Propylthiouracil) & Tapazole (Methimazole) thyroid crisis
- inhibit synthesis of thyroid hormones ● Monitor BP (hypertension may be a manifestation of thyroid storm)
○ Side effects of PTU: ● assess for Trousseau’s sign (hypocalcemia)
- AGRANULOCYTOSIS / NEUTROPENIA ● Steam inhalation to soothe irritate airways
- This is manifested by unexplained Fever, Sore throat, ● Advise to support neck with interlaced fingers when getting up from
Skin rashes bed
● Observe for signs and symptoms of potential complications
○ Hemorrhage
○ Airway obstruction
○ Tetany
○ Recurrent laryngeal nerve damage
○ Thyroid crisis / storm / thyrotoxicosis
○ Myxedema
● Client Teaching
○ ROM exercises of the neck 3 to 4 days after discharge
○ Regular follow – up care
Hypothyroidism
- Paracetamol for fever
○ Aspirin must be avoided because it can displace the T3/T4 - results from deficiency of thyroid hormones
from the albumin in the plasma causing increased
manifestations
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 39
● Myxedema (adult)
● Cretinism (child)
● Causes:
○ Severe emotional stress
- Hashimoto’s disease or chronic lymphocytic thyroiditis - an
autoimmune disorder in which your immune system
inappropriately attacks your thyroid gland causing an
inflammation
○ after surgery (thyroidectomy)
○ after radiation therapy (radioactive iodine)
○ antithyroid drugs
● Assessment:
- Slowed physical, mental reactions, apathy
- Dull, expressionless, mask-like face
- Anorexia
- Obesity
- Bradycardia
- Hyperlipidemia & atherosclerosis
- Cold intolerance, subnormal temperature
- Constipation
- Coarse, dry, sparse hair
- Brittle nails
- Irregular menstruation
● Management:
- Monitor vital signs
- Be alert for signs and symptoms of cardiovascular disorders
- Monitor the weight daily
- Diet:
○ LOW Calorie
○ High fiber (constipation)
- Provide warm environment during cold climate
● Pharmacotheraphy:
- Thyroid hormonal replacement
○ Proloid (Thyroglobulin)
○ Synthroid (Levothyroxine)
○ Dessicated Thyroid Extract
○ Cytomel (Liothyronine)
- Before administration, the nurse should monitor BP & PR
- Start with low dose and gradually increase
WEEK 1: DIGESTIVE SYSTEM (15/15)
1. Which of these is NOT a pair of salivary glands?
a. submucosal
b. parotid
c. submandibular
d. sublingual
2. All of these structures are matched with the correct description EXCEPT:
a. cardiac region: the area closest to the small intestine
b. fundus: the most superior portion of the stomach
c. pyloric opening: opening from the stomach
d. body: the largest portion of the stomach
3. Which statement about the esophagus is TRUE? Select al that apply.
a. it has upper and lower sphincters
b. it extends from the nasal cavity to the stomach
c. it is a cartilaginous tube
d. it lies anterior to the trachea
e. all statements describe the esophagus
4. The saliva does NOT contain:
a. hydrochloric acid
b. amylase
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 40
c. mucin c. decrease daily intake of vegetables and water, and ambulate
d. lysozyme frequently
5. Which of the following produce gastrin? d. avoid over-the-counter drugs that have antacids in them.
a. mucous neck cells 3. The nurse is performing an admission assessment on a client diagnosed
b. surface mucous cells with GERD. Which sign and symptoms would indicate GERD?
c. endocrine cells a. midepigastric pain, positive H. pylori test, and melena
d. parietal cells b. weight loss, dysarthria, and diarrhea
e. chief cells c. decreased abdominal fat, proteinuria, and constipation
6. Which statements best describe mechanical digestion? Select all that d. pyrosis, water brash, and flatulence
apply. 4. Which diagnostic results does NOT support the diagnosis of peptic ulcer
a. it involves the breaking of covalent chemical bonds in organic disease (PUD)?
molecules by digestive enzymes a. low white blood cell (WBC) level
b. it breaks large food particles into smaller ones b. low hemoglobin (Hgb)
c. it begins in the stomach, where some small, lipid-soluble molecules, c. Low hematocrit (Hct)
such as alcohol and aspirin, can diffuse through the stomach d. Positive for H. pylori bacteriae and low potassium of 23.4 mEq/L
epithelium into the circulation 5. What is the nursing priority in the management of a patient with an active
d. it requires carrier molecules and includes facilitated diffusion, upper G.I. bleed?
contransport, and active transport a. apply oxygen by nasal cannula
e. all the statements describe mechanical digestion b. type and crossmatch the patient for blood products
7. The greatest volume of gastric secretion occurs during: c. notify the physician
a. cephalic phase d. obtain vital signs
b. gastric phase 6. The patient who is admitted with a diagnosis of diverticulitis and a history
c. intestinal phase of irritable bowel disease and gastroesophageal reflux disease (GERD) has
d. deglutition received a dose of Mylanta 30ml PO. The nurse should evaluate its
8. Which of the following is not a function of the digestive system? effectiveness by questioning the patient as to whether which symptom
a. thermoregulation has been resolved?
b. mechanical breakdown of large organic compounds a. heartburn
c. absorption of nutrients b. diarrhea
d. mechanical processing c. lower abdominal pain
9. Arrange the correct sequence of the steps involved in the process of d. constipation
Human Digestive System? 7. A patient with a history of peptic ulcer disease has presented to the
a. ingestion, digestion, absorption, assimilation and egestion emergency department reporting severe abdominal pain and has a rigid,
b. digestion, ingestion, assimilation, egestion and absorption boardlike abdomen that prompts the health care team to suspect a
c. egestion, absorption, digestion, assimilation and ingestion perforated ulcer. What intervention should the nurse anticipate?
d. assimilation, absorption, ingestion, digestion and egestion a. Providing IV fluids and inserting a nasogastric (NG) tube
10. In which part of the body digestion of protein begins? b. Administering oral bicarbonate and testing the patient’s gastric pH
a. stomach level
b. large intestine c. Performing a fecal occult blood test and administering IV calcium
c. small intestine gluconate
d. pancreas d. Starting parenteral nutrition and placing the patient in a high-
11. Name the largest part of the Alimentary canal? fowler’s position
a. small intestine 8. The results of a patient’s recent endoscopy indicate the presence of
b. large intestine peptic ulcer disease (PUD). Which teaching point should the nurse
c. liver provide to the patient based on this new diagnosis?
d. stomach a. “your medications should allow you to maintain your present diet
12. Complete digestion of food occurs in: while minimizing symptoms”
a. small intestine b. “it would likely to be beneficial for you to eliminate drinking
b. stomach alcohol”
c. pancreas c. “Many people find that a minced or poured diet eases their
d. large intestine symptoms of PUD.”
13. What is the function of Bile Juice secreted by Liver? d. “You’ll need to drink at least two to three glasses of milk daily.”
a. it makes the food alkaline 9. The patient is having an esophagoenterostomy with anastomosis of a
b. it makes the food acidic segment of the colon to replace the resected portion. What initial
c. it breaks down the food postoperative care should the nurse expect when this patient returns to
d. none of the above the nursing unit?
14. In which part of our body gets absorbed a. NG will have bloody drainage, and it should not be repositioned
a. small intestine b. Turn, deep breathe, cough, and use spirometer every 4 hours
b. large intestine c. Keep in a supine position to prevent movement of the anastomosis
c. stomach d. Maintain an upright position for at least 2 hours after eating
d. liver 10. The patient with chronic gastritis is being put on a combination of
15. The undigested food stored in the liver in the form of carbohydrate is medications to eradicate H. pylori. Which drugs does the nurse know will
called: probably be used for this patient?
a. glycogen a. Antibiotic(s), aspirin, and antiulcer/protectant
b. carbohydrate b. Antibiotic(s), proton pump inhibitor
c. glucose c. Antibiotic(s), and nonsteroidal antiinflammatory drugs (NSAIDs)
d. pulp d. Antibiotic(s), antacid, and corticosteroid
11. The patient is having gastroduodenostomy (Billroth I operation) for
stomach cancer. What long-term complication is occurring when the
WEEK 1: GIT DIAGNOSTIC TESTS & DISEASE (20/20) patient reports generalized weakness, sweating, palpitations, and
1. The male client tells the nurse he has been experiencing “heartburn” at dizziness 15 to 30 minutes after eating?
night that awakens him. Which assessment question should the nurse a. dumping syndrome
ask? b. postprandial hypoglycemia
a. “have you been around anyone with a stomach virus” c. malnutrition
b. “what have you done to alleviate the heartburn” d. bile reflux gastritis
c. “do you consume many milk and dairy products” 12. A 46-year-old female with gastroesophageal reflux disease (GERD) is
d. “how much weight have you gained recently” experiencing increasing discomfort. Which patient statement indicates
2. Gastroesophageal reflux disease (GERD) weakens the lower esophageal that additional teaching about GERD is needed?
sphincter, predisposing older persons to risk for impaired swallowing. In a. “I quit smoking several years ago, but I still chew a lot of gum.”
managing the symptoms associated with GERD, the nurse should assign b. “I sleep with the head of the bed elevated on 4-inch blocks.”
the highest priority to which of the following interventions? c. “I take antacids between meals and at bedtime each night.”
a. drink coffee diluted with milk at each meal, and remain in an upright d. “I eat small meals during the day and have a bedtime snack.”
position for 30 minutes. 13. The nurse will anticipate teaching a patient experiencing frequent
b. eat small, frequent meals, and remain in an upright position for at heartburn about?
least 30 minutes after eating a. endoscopy procedures
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 41
b. barium swallow d. To the exact size of the stoma.
c. radionuclide tests 5. You're performing an abdominal assessment on Brent who is 52 y.o. In
d. proton pump inhibitors which order do you proceed
14. Which information about dietary management should the nurse include a. Observation, percussion, palpation, auscultation
when teaching a patient with peptic ulcer disease (PUD)? b. Palpation, percussion, observation, auscultation
a. “High-protein foods are least likely to cause you pain.” c. Observation, auscultation, percussion, palpation
b. “You will need to need to remain on a bland diet.” d. Percussion, palpation, auscultation, observation
c. “Avoid foods that cause pain after you eat them.” 6. Matt is a 49 y.o. with a hiatal hernia that you are about to counsel. Health
d. “You should avoid eating any raw fruits and vegetables.” care counseling for Matt should include which of the following
15. A client with peptic ulcer disease (PUD) asks the nurse whether licorice instructions?
and slippery elm might be useful in managing the disease. What is the a. Eat three regular meals a day.
nurse’s best response?
a. “Yes, these are known to be effective in managing this disease, but b. Restrict intake of high-carbohydrate foods.
make sure you research the herbs thoroughly before taking them.” c. Increase fat intake.
b. “No, herbs are not useful for managing this disease. You can use any d. Increase fluid intake with meals.
type of over-the-counter drugs through. They have been shown to 7.
be safe.”
8. Your patient is complaining of abdominal pain during assessment. What is
c. “These herbs could be helpful. However, you should talk with your
provider before adding them to your treatment regimen.” your priority?
d. “No, they probably won’t be useful. You should use only a. Auscultate to determine changes in bowel sounds.
prescription medications in your treatment plan.” b. Percuss the abdomen to determine if fluid is present.
16. The nurse is teaching a client how to prevent recurrent chronic gastritis
symptoms before discharge. Which statement by the client demonstrates c. Observe the contour of the abdomen.
a correct understanding of the nurse’s instruction? d. Palpate the abdomen for a mass.
a. “Ibuprophen should be taken” 9. Katrina is diagnosed with lactose intolerance. To avoid complications with
b. “I will need to take vitamin B12 shots for the rest of my life” lack of calcium in the diet, which food should be included in the diet?
c. “It is okay to continue to drink coffee in the morning when I get to a. Dark green, leafy vegetables
work.” b. Milk and cheese products
d. “I should eat small meals about six times a day.” c. Fruit
17. The client is experiencing bleeding related to peptic ulcer disease (PUD). d. Whole grains
Which nursing intervention is the highest priority? 10. Christina is receiving an enteral feeding that requires a concentration of
a. administering intravenous (IV) pain medication 80 ml of supplement mixed with 20 ml of water. How much water do you
b. starting a large-bore intravenous (IV) mix with an 8 oz (240ml) can of feeding?
c. preparing equipment for intubation a. 60 ml
d. monitoring the client’s anxiety level b. 70 ml
18. Which of the following instructions should the nurse include in the
teaching plan for a client who is experiencing gastroesophageal reflux c. 80 ml
disease (GERD)? d. 90 mi
a. limit caffeine intake to two cups of coffee per day
b. do not lie down for 2 hours after eating
c. take medication with milk to decrease irritation WEEK 2: LOWER GI (18/20)
d. follow a low-protein diet 1. Which of the following complications is thought to be the most common
19. The client with gastroesophageal reflux disease (GERD) complains of a cause of appendicitis?
chronic cough. The nurse understands that in a client with GERD this a. Internal bowel occlusion
symptom may be indicative of which of the following conditions? b. Bowel kinking
a. irritation of the esophagus c. Fecalith
b. development of laryngeal cancer d. Abdominal bowel swelling
c. esophageal scar tissue formation 2. Which of the following terms best describes the pain associated with
d. aspiration of gastric contents appendicitis?
20. The client is scheduled to have an upper gastrointestinal tract series of x- a. Aching
rays. Following the x-rays, the nurse should instruct the client to: b. Fleeting
a. follow a clear liquid diet c. Intermittent
b. administer an enema d. Steady
c. take an antiemetic 3. Which of the following nursing interventions should be implemented to
d. take a laxative manage a client with appendicitis?
a. Assessing for symptoms of peritonitis
b. Encouraging oral intake of clear fluids
WEEK 2: GI (9/10) c. Assessing for pain
d. Providing discharge teaching
1. You're assessing the stoma of a patient with a healthy, well-healed 4. Which of the following definitions best describes diverticulosis?
colostomy. You expect the stoma to appear: a. An inflamed outpouching of the intestine
a. Dark or purple colored b. The partial impairment of the forward flow of intestinal contents
b. Dry and black c. An abnormal protrusion of an organ through the structure that
c. Red and moist usually holds it
d. Pale, pink and moist d. A non-inflamed outpouching of the intestine
2. You're caring for a patient with a sigmoid colostomy. The stool from this 5. Which of the following tests should be administered to a client suspected
colostomy is: of having diverticulosis?
a. Semisolid a. Barium swallow
b. Semi liquid b. Gastroscopy
c. Watery c. Abdominal ultrasound
d. Barium enema
d. Formed
6. Medical management of the client with diverticulitis should include which
3. You're advising a 21 y.o. with a colostomy who reports problems with of the following treatments?
flatus. What food should you recommend? a. Administration of antibiotics
a. Yogurt b. Increased fiber in diet
b. Peas c. Reduced fluid intake
c. Cabbage d. Exercises to increase intra-abdominal pressure
d. Broccoli 7. Samantha, a 65 .o. woman with diverticulosis is your patient. Which
4. You have to teach ostomy self-care to a patient with a colostomy. You tell interventions would you expect to include in her care?
the patient to measure and cut the wafer: a. High-fiber diet and administration of psyllium.
a. About 1/4" larger than the stoma. b. Administration of analgesics and antacids.
b. About 1/16" larger than the stoma c. Low-fiber diet and fluid restrictions.
c. About 1/8" larger than the stoma. d. Total parenteral nutrition and bed rest.
8. Ariel is a 63 y.o. man with diverticulitis. Diverticulitis is characterized by:
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 42
a. Crampy and lower left quadrant pain and low-grade fever d. Assess the client for a rigid abdomen.
b. Hypertension and tachycardia. 19. True or False: A patient with Crohn's Disease can experience
c. Periodic rectal hemorrhage. inflammation in the large intestine that affects mainly the mucosa (inner
d. Vomiting and elevated temperature. layer) of the bowel.
9. True or False: The appendix is found on the left lower side of the abdomen a. True
and is connected to the cecum of the large intestine. b. False
a. False 20. A patient with Crohn's Disease is most likely to have the disease is what
b. True part of the GI tract?
10. A 23 year old patient is admitted with suspected appendicitis. The patient a. Duodenum of the small intestine
states he is having pain around the umbilicus that extends into the lower b. Terminal ileum
part of his abdomen. In addition, he says that the pain is worst on the c. Descending colon
right lower quadrant. The patient points to his abdomen at a location d. Rectum
which is about a one-third distance between the anterior superior iliac
spine and umbilicus. This area is known as what?
a. Hamman's Point WEEK 3: LIVER, PANCREAS & GALLBRADDERI (25/25)
b. Rovsing's Point
c. Murphy's Point 1. Allanis, a 22 yo. factory worker is admitted with acute pancreatitis. Which
d. McBurney's Point laboratory findings do you expect to be abnormal for this patient?
11. A patient is scheduled for appendectomy at noon. While performing your a. Cardiac enzymes
morning assessment, you note that the patient has a fever of 103.8 'F and b. Serum creatinine and BUN
rates abdominal pain 9 on 1-10. In addition, the abdomen is distended c. Alanine aminotransferase (ALT) and aspartate aminotransferase
and the patient states, "I was feeling better last night but it seems the (AST)
pain has become worst." The patient is having tachycardia and d. Serum amylase and lipase
tachypnea. Based on the scenario, what do you suspect the patient is 2. Toni has cholelithiasis (gallstones). You expect her to complain of:
experiencing? a. Pain in the right lower quadrant, with rebound tenderness.
a. Colon Fistulae b. Pain in the left upper quadrant, with shortness of breath.
b. Hemorrhage c. Pain in the left lower quadrant, with mild cramping.
c. Peritonitis d. Pain in the right upper quadrant, radiating to the shoulder
d. Pulmonary embolism 3. Tina, a 53-year-old woman, is diagnosed with cholecystitis. Which diet,
12. The major cause of death from peritonitis is: when selected by the client, indicates that the nurse's teaching has been
a. Hypovolemia. successful?
b. Shocks a. 4-6 small meals of low-carbohydrate foods daily
c. Abscess formation. b. High-fat, low protein meals
d. Sepsis. c. High-fat, high-carbohydrate meals
13. Peritonitis occurs in which part of the Gl system? d. Low-fat, high-carbohydrate meals
a. Sigmoid colon 4. Which clinical manifestation would the nurse expect a client diagnosed
b. Peritoneum. with acute cholecystitis to exhibit?
c. Appendix. a. Ecchymosis petechiae, and coffee-ground emesis
d. Duodenum. b. Jaundice, dark urine, and steatorrhea
14. The nurse is interviewing a male client about his past medical history. c. Nausea, vomiting, and anorexia
Which preexisting condition may lead the nurse to suspect that a client d. Acute right lower quadrant (RLQ) pain, diarrhea, and dehydration
has colorectal cancer? 5. Anthony who is diagnosed with acute pancreatitis is under the care of
a. Polyps Nurse Carl. Which intervention should the nurse include in the care plan
b. Hemorrhoids for the client?
c. Duodenal ulcer a. Maintenance of nothing-by-mouth status and insertion of
d. Weight gain nasogastric (NG) with low intermittent suction
15. Client education should include minimizing client discomfort due to b. Dietary plan of a low-fat diet and increased fluid intake to 2,000
ml/day
hemorrhoids. Nursing management should include: c. Preparation for a paracentesis and administration of diuretics
a. Suggest to eat low roughage diet d. Administration of vasopressin and insertion of a balloon tamponade
b. Avoid straining during defecation 6. When teaching a client about pancreatic function, the nurse understands
c. Use of sitz bath for 30 minutes that pancreatic lipase performs which function?
a. Breaks down fat into fatty acids and glycerol
d. Advise to wear silk undergarments
b. Breaks down protein into dipeptides and amino acids
(NOTE: B prevents. C minimizes discomfort.)
c. Triggers cholecystokinin to contract the gallbladder
16. A client is admitted with a bowel obstruction. The client has nausea,
vomiting, and crampy abdominal pain. The physician has written orders d. Transports fatty acids into the brush border
for the client to be up ad lib, to have narcotics for pain, to have a 7. For Monet who has chronic pancreatitis, which nursing intervention
nasogastric tube inserted if needed, and for I.V. Ringer's Lactate and would be most helpful?
hyperalimentation fluids. The nurse should do the following in order of a. Modifying dietary protein
priority from first to last: b. Encouraging daily exercise
1. Assist with ambulation to promote peristalsis c. Counseling to stop alcohol consumption
2. Administer Ringer's Lactate d. Allowing liberalized fluid intake
3. Insert a nasogastric tube. 8. For Gryffin who is taking antacids, which instruction would be included in
4. Start and infusion of hyperalimentation fluids. the teaching plan?
a. 2,1.4,3
b. 3,4,2,1 a. "Continue taking antacids even when pain subsides."
c. 1,3,4,2 b. "Avoid taking other medications within 2 hours of this one."
d. 4,3,2,1 c. "Take the antacids with 8 oz. of water."
e. 1,2,3,4 d. "Weigh yourself daily when taking this medication."
17. The physician orders intestinal decompression with a Cantor tube for a
client with an intestinal obstruction. In order to determine effectiveness 9. The liver receives blood from two sources. The is responsible for pumping
of intestinal decompression the nurse should evaluate the client to blood rich in nutrients to the liver.
determine if: a. hepatic artery
a. Fluid and gas have been removed from the intestine. b. mesenteric artery
b. The client has had a bowel movement c. hepatic portal vein
c. The client's urinary output is adequate.
d. The client can sit up without pain. d. hepatic iliac vein
18. The client with an intestinal obstruction continues to have acute pain 10. A patient is diagnosed with Hepatitis A. The patient asks how a person
even though the nasoenteric tube is patent and draining. Which action by can become infected with this condition. You know the most common
the nurse would be most appropriate? route of transmission is?
a. Administer an opioid as ordered. a. Mucosal
b. Reposition the client on the left side. b. Fecal-oral
c. Reassure the client that the nasoenteric tube is functioning. c. Blood
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 43
d. Percutaneous 21. A patient hospitalized with possible acute pancreatitis has severe
11. A 25-year-old patient was exposed to the Hepatitis A virus at a local abdominal pain and nausea and vomiting. The nurse would expect the
restaurant one week ago. What education is important to provide to this diagnosis to be confirmed with laboratory testing that reveals elevated
patient? serum:
a. Inform the patient it is very important to obtain the Hepatitis A a. potassium.
vaccine immediately to prevent infection. b. amylase
b. Reassure the patient the chance of acquiring the virus is very low. c. calcium.
c. Inform the patient to notify the physician when signs and symptoms d. bilirubin.
of viral Hepatitis start to appear. 22. In planning care for a patient with acute pancreatitis, the nurse assigns
d. Inform the patient to promptly go to the local health department the highest priority to the patient outcome of:
to receive immune globulin. a. having adequate fluid and electrolyte balance.
12. A patient with Hepatitis A asks you about the treatment options for this b. maintenance of normal respiratory function.
condition. Your response is? c. expressing satisfaction with pain control.
a. Supportive care
d. developing no acute complications.
b. Interferon
23. A patient with acute pancreatitis has a nasogastric (NG) tube to suction
c. Antiviral medications and is NPO. The nurse explains to the patient that the major purpose of
d. Hepatitis A vaccine this treatment is:
(Note: There is no current treatment for Hepatitis A but supportive care and rest. a. reduction of pancreatic enzymes.
b. control of fluid and electrolyte imbalance.
Treatments for the other types of Hepatitis such as B, C, and D include antiviral c. removal of the precipitating irritants.
or interferon (mainly the chronic cases) along with rest.) d. relief from nausea and vomiting.
13. What is the MOST common transmission route of Hepatitis C? 24. When obtaining a health history from a patient with acute pancreatitis, the
a. Sharps injury nurse asks the patient specifically about a history of:
b. Blood transfusion a. high-protein diet.
c. IV drug use b. alcohol use.
d. Long-term dialysis c. cigarette smoking.
14. What is the BEST preventive measure to take to help prevent ALL types d. diabetes mellitus.
of viral Hepatitis? 25. A patient who was admitted with acute bleeding from esophageal varices
a. Hand hygiene asks the nurse the purpose for the ordered ranitidine (Zantac). Which
b. Proper disposal of needles response by the nurse is most appropriate?
c. Blood and organ donation screening a. The medication will reduce the risk for aspiration.
d. Vaccination b. The medication will decrease nausea and anorexia.
15. "A patient with hepatitis B is being discharged in 2 days. In the discharge c. The medication will inhibit the development of gastric ulcers.
teaching plan the nurse should include instructions to: d. The medication will prevent irritation to the esophageal varices.
a. Use a condom during sexual intercourse
b. Follow a low-protein, moderate-carbohydrate, moderate-fat diet WEEK 4: ENDOCRINE SYSTEM (10/10)
c. Have family members get an injection of immunoglobin
1. The following are the functions of the endocrine system, except
d. Avoid alcohol for the first 3 weeks a. Water balance
16. A client is suspected of having hepatitis. Which diagnostic test result will b. Regulate heart rate and blood pressure
assist in confirming this diagnosis ? c. Regulates immune system
a. Decreased erythrocyte sedimentation rate d. Direct blood flow
b. Elevated serum bilirubin level e. Controls reproductive function
2. The primary function of T3 and T4 is to:
c. Elevate hemoglobin level a. Release calcitonin
d. Elevated blood urea nitrogen level b. Increase metabolic rate
17. Which type of hepatitis is transmitted by the fecal-oral route via c. Reduce blood glucose levels
d. Regulate bone growth
contaminated food, water, or direct contact with an infected person?
3. Antidiuretic hormone and oxytocin are stored and released by the:
a. Hepatitis B a. Adrenal cortex
b. Hepatitis D b. Thyroid gland
c. Hepatitis A c. Pineal gland
d. Posterior pituitary gland
d. Hepatitis C 4. Which hormone stimulates the male testes to produce sperm and
18. When planning care for a patient with cirrhosis, the nurse will give highest stimulates the development of the follicle in the female on a monthly
priority to which of the following nursing diagnoses? cycle.
a. Impaired skin integrity related to edema, ascites, and pruritus a. Somatostatin
b. Imbalanced nutrition: less than body requirements b. Luteinizing hormone
c. Ineffective breathing pattern related to pressure on diaphragm and c. Thymosin
reduced lung volume d. Follicle-stimulating hormone
5. A client with a history of hypertension is admitted due to primary
d. Excess fluid volume related to portal hypertension and hyperaldosteronism. This diagnosis indicates that the client's
hyperaldosteronism hypertension is caused by excessive hormone secretion from which
19. The nurse is reviewing the lab results for a pt with cirrhosis and notes that gland?
the ammonia level is elevated. Which diet does the nurse anticipate to be a. Adrenal medulla
prescribed for this pt? b. Thymus gland
a. High-protein c. Adrenal cortex
b. Low-protein d. Pancreas
c. Moderate-fat 6. The mineralocorticoids produced by the adrenal glands are produced
d. High-carb within the?
20. The pt with advanced cirrhosis asks why his abdomen is so swollen. The a. Zona glomerulosa
nurse's best response is based on the knowledge that: b. Zona fasciculata
a. a lack of clotting factors promotes the collection of blood in the c. Zona reticularis
d. Parafollicular cells
abdominal cavity
7. Which of the following glands is both an endocrine gland and an exocrine
b. bile salts in the blood irritate the peritoneal membranes, causing gland, except?
edema and pocketing of fluid. a. Pancreas
c. portal hypertension and hypoalbuminemia cause fluid shift into the b. Kidney
c. Gonads
peritoneal space. d. Pituitary gland
d. decreased peristalsis in the Gl tract contributes to gas formation and 8. Which of the following is not true with melatonin
distention of the bowel a. The secretion of melatonin is inhibited by darkness and triggered
by light.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 44
b. The pineal gland produces and secretes the hormone. 9. A patient suspected of having acromegaly has an elevated plasma growth
c. It helps regulate biological rhythms such as sleep and wake cycles. hormone level. In acromegaly, the nurse would also expect the patient's
d. Melatonin induces heat loss, reduces arousal and related brain diagnostic results to include:
activity and delays production of cortisol. a. Hyperinsulinemia
9. Part of the effect of growth hormone is influenced by a group of protein b. A plasma glucose of less than 70
chemical signals called: c. Decreased growth hormone levels with an oral glucose challenge
a. Somatomedin-C test
b. Prostaglandin d. A serum somatomedin C (insulin-like growth-factor) of more than
c. Prolactin 300
d. Gonadotropins 10. Which of the following is true regarding growth hormone (GH)
10. A client arrived at the emergency department with a possible diagnosis deficiencies?
of hyperparathyroidism. The nurse anticipates which serum electrolytes a. It can occur in adults as well as children.
finding would be abnormal? Select all that apply b. It occurs only in children.
a. Potassium c. It always results in dwarfism.
b. Sodium d. It is treated only in children because GH is usually produced only
c. Chloride until puberty.
d. Calcium 11. The 6-year-old son of Mr. and Mrs. Peters is admitted to the healthcare
e. Phosphorus facility with the diagnosis of idiopathic hypopituitarism. His height is
measured below the third percentile and weight at the 40th percentile.
Which of the following would be the first action of his attending nurse G?
WEEK 4: A/P OF ENDOCRINE SYSTEM & PITUITARY GLAND a. Provide for a tutor for his precocious intellectual ability.
(18/20) b. Recommend orthodontic referral for underdeveloped jaw.
1. A female client whose physical findings suggest a hyperpituitary condition c. Place him in a room with a 2-year-old boy.
undergoes an extensive diagnostic workup. Test results reveal a pituitary d. Collaborate with a dietician to access his caloric needs.
tumor, which necessitates a transsphenoidal hypophysectomy. The 12. While Andres is being assessed at the clinic, Nurse Shiela observed that
evening before the surgery, nurse Jacob reviews preoperative and the child appears to be small, with an immature face and chubby body
postoperative instructions given to the client earlier. Which build. Her parents stated that their child's rate of growth of all body parts
postoperative instruction should the nurse emphasize? is somewhat slow, but her proportions and intelligence remain normal.
a. "You must restrict your fluid intake." As a knowledgeable nurse, you know that the child has a deficiency of
b. "You must avoid coughing, sneezing, and blowing your nose." which of the following?
c. "You must lie flat for 24 hours after surgery." a. Melanocyte-stimulating hormone (MSH)
d. "You must report ringing in your ears immediately." b. Growth hormone (GH)
c. Antidiuretic hormone (ADH)
2. A patient suspected of having acromegaly has an elevated plasma growth
d. Parathyroid hormone (PTH)
hormone level. In acromegaly, the nurse would also expect the patient's
13. Nurse Aries entered the room of a child with hypopituitarism and was
diagnostic results to include:
asked by the couple about the condition of their child. Which of the
a. decreased growth hormone levels with an oral glucose challenge
following phrases if stated by the nurse best describes the condition?
test
a. A complete normal growth pattern, but with the onset of
b. a serum somatomedin C (insulin-like growth-factor) of more than
precocious puberty
300
b. Normal growth for first five years, followed by progressive linear
c. hyperinsulinemia
growth retardation
d. a plasma glucose of less than 70
c. Growth retardation in which height and weight are equally affected
3. During assessment of the patient with acromegaly, the nurse would
d. Linear growth retardation with skeletal proportions normal for
expect the patient to report:
chronologic age
a. infertility
14. The following are the functions of the endocrine system, except?
b. dry, irritated skin
a. Regulate heart rate and blood pressure
c. an increase in height of 2 to 3 inches per year
b. Water balance
d. undesirable changes in appearance
c. Direct blood flow
4. A patient with acromegaly is treated with a transsphenoidal
d. Regulates immune system
hypophysectomy. Postoperatively, the nurse:
e. Controls reproductive function
a. Ensures that any clear nasal drainage is tested for glucose
15. The primary function of T3 and T4 is to:
b. Encourages deep breathing and coughing to prevent respiratory
a. Regulate bone growth
complications
b. Release calcitonin
c. Maintains the patient flat in bed to prevent cerebrospinal fluid leak
c. Reduce blood glucose levels
d. Assists the patient with toothbrushing Q4H to keep the surgical area
d. Increase metabolic rate
clean
16. Antidiuretic hormone and oxytocin are stored and released by the:
5. A patient suspected of having acromegaly has an elevated plasma growth
a. Adrenal cortex
hormone (GH) level. In acromegaly, what would the nurse also expect the
b. Thyroid gland
patient's diagnostic results to indicate?
c. Pineal gland
a. Elevated levels of plasma insulin-like growth factor-1 (IGF-1)
d. Posterior pituitary gland
b. Hyperinsulinemia
17. A client with a history of hypertension & is admitted due to primary
c. Decreased GH levels with an oral glucose challenge test
hyperaldosteronism. This diagnosis indicates that the client's
d. Plasma glucose of <70 mg/dL (3.9 mmol/L)
hypertension E is caused by excessive hormone secretion from which
6. Dwarfism (hypopituitarism) - complication?
gland?
a. growth hormone measured in blood plasma
a. Adrenal medulla
b. body image disturbance, nutrition-altered, chronic pain, risk for
b. Thymus gland
sexual dysfunction
c. Pancreas
c. unclear
d. Adrenal cortex
d. diabetes
18. The following glands are both an endocrine gland and an exocrine gland,
7. The nurse is caring for a client with acromegaly. Following a
except?
transsphenoidal hypophysectomy, the nurse should:
a. Kidney
a. Suction the mouth and pharynx every hour
b. Pancreas
b. Encourage the client to cough
c. Gonads
c. Place the client in low Trendelenburg position
d. Pituitary gland
d. Monitor the client's blood sugar
19. Part of the effect of growth hormone is influenced by a group of protein
8. A patient with acromegaly is treated with a transsphenoidal
chemical signals called:
hypophysectomy. Postoperatively, the nurse:
a. Somatomedin-C
a. Encourages deep breathing and coughing to prevent respiratory
b. Prostaglandin
complications
c. Prolactin
b. Ensures that any clear nasal drainage is tested for glucose
d. Gonadotropins
c. Maintains the patient flat in bed to prevent cerebrospinal fluid leak
20. Which of the following is not true with melatonin?
d. Assists the patient with toothbrushing Q4H to keep the surgical area
a. The secretion of melatonin is inhibited by darkness and triggered
clean
by light.
b. The pineal gland produces and secretes the hormone.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 45
c. It helps regulate biological rhythms such as sleep and wake cycles
d. Melatonin induces heat loss, reduces arousal and related brain
activity and delays production of cortisol.
🍎🍓🍑🍒🌶️ (Shane, Mae, Rocette, Mary, Khlaryzel) pg. 46
You might also like
- ArrhythmiaDocument2 pagesArrhythmiaChris Pritchard93% (30)
- Digestive SystemDocument114 pagesDigestive SystemAj MirandaNo ratings yet
- MSE Psychiatric InterviewingDocument26 pagesMSE Psychiatric InterviewingZonny PatelNo ratings yet
- DR Thomas Brown PH D Attention Deficit Disorder The Unfocused Mind in Children and AdultsDocument191 pagesDR Thomas Brown PH D Attention Deficit Disorder The Unfocused Mind in Children and AdultsjenNo ratings yet
- Digestive System Anatomy and Physiology - NurseslabsDocument33 pagesDigestive System Anatomy and Physiology - NurseslabsMari FeNo ratings yet
- Lesson 4 Digestive SystemDocument10 pagesLesson 4 Digestive SystemJulio De GuzmanNo ratings yet
- 9 GitDocument81 pages9 GitAbdurahman Tainy100% (1)
- Compilation Medsurg PrelimsDocument29 pagesCompilation Medsurg PrelimsEunice CuñadaNo ratings yet
- Aetcom 3.5Document4 pagesAetcom 3.5Kondayoor SharadaNo ratings yet
- III - Digestive SystemDocument3 pagesIII - Digestive SystemGael QuingNo ratings yet
- Covid Studies and ArticlesDocument10 pagesCovid Studies and ArticlesKelly McNeiceNo ratings yet
- Digestive and Body MetabolismDocument25 pagesDigestive and Body MetabolismGuenNo ratings yet
- NCMB 316 M1 Cu1Document23 pagesNCMB 316 M1 Cu1Maica Lectana100% (1)
- Ivan PavlovDocument6 pagesIvan PavlovJerah Revicente RosalNo ratings yet
- GROUP 1 - Digestive SystemDocument76 pagesGROUP 1 - Digestive SystemMa. Therese CampoNo ratings yet
- Pathophysiology of Acquired Immunodeficiency Syndrome: Predisposing Factors Predisposing FactorsDocument1 pagePathophysiology of Acquired Immunodeficiency Syndrome: Predisposing Factors Predisposing FactorsJason A. Adoyogan0% (1)
- Nutrition&DietTherapy (LAB) - Functions of The Digestive SystemDocument14 pagesNutrition&DietTherapy (LAB) - Functions of The Digestive SystemkappaNo ratings yet
- RT 204 Prefinal TransesDocument22 pagesRT 204 Prefinal TransesLouise0% (1)
- Ncmb316 Prelim (Bai)Document41 pagesNcmb316 Prelim (Bai)kpbalay5921pamNo ratings yet
- Gastrointestinal TractDocument5 pagesGastrointestinal TractMalayao, Philip Jude M.No ratings yet
- Digestive SystemDocument5 pagesDigestive Systemlim.angelyne0126No ratings yet
- THE Disgestive System: by Second GroupDocument17 pagesTHE Disgestive System: by Second GroupAuliya AlfaNo ratings yet
- Pemicu 1 GIT Aldi FDocument86 pagesPemicu 1 GIT Aldi Faldi firdausNo ratings yet
- Digestive System 16 18Document11 pagesDigestive System 16 18riguel222No ratings yet
- Digestion and Absorption-AKDocument63 pagesDigestion and Absorption-AKSaiNagaVignesh BandhamNo ratings yet
- MetabolismDocument3 pagesMetabolismElsie CarbonNo ratings yet
- Outline: Relative Measurements of Alimentary TractsDocument9 pagesOutline: Relative Measurements of Alimentary TractsProfessor GhoulNo ratings yet
- Anaphy FinalsDocument20 pagesAnaphy FinalsHazel Anne Dela CruzNo ratings yet
- Chapter XI DigestiveDocument19 pagesChapter XI DigestiveTitoMacoyTVNo ratings yet
- Digestion and Absorption NotesDocument60 pagesDigestion and Absorption NotesAstha AgrawalNo ratings yet
- Digestive SystemDocument2 pagesDigestive SystemRashid DayaoNo ratings yet
- UNIT 11 CompressedDocument24 pagesUNIT 11 Compressedemerald CasinilloNo ratings yet
- Digestive System Summary of The Main PointsDocument6 pagesDigestive System Summary of The Main PointsElaf NaifNo ratings yet
- Chapter - 16 Digestion and Absorption: Unit - 5 Human PhysiologyDocument4 pagesChapter - 16 Digestion and Absorption: Unit - 5 Human Physiologysonu kumarNo ratings yet
- Digestive SystemDocument12 pagesDigestive SystemJen SmithNo ratings yet
- Characterized: Heterotrophs or Organisms That Cannot Make Their OwnDocument5 pagesCharacterized: Heterotrophs or Organisms That Cannot Make Their OwnKyungsoo DoNo ratings yet
- Digestive SystemDocument15 pagesDigestive SystemHenry BuñagNo ratings yet
- Physiology 2 Doc - 055059Document44 pagesPhysiology 2 Doc - 055059Bhagyashri DarjiNo ratings yet
- Digestive System FinalsDocument6 pagesDigestive System FinalsAlliana Pauline AbanNo ratings yet
- (Compana) Digestive SystemDocument10 pages(Compana) Digestive SystemTherese Claire Marie JarciaNo ratings yet
- Lab Act DigestiveDocument8 pagesLab Act DigestiveJhia TorreonNo ratings yet
- Digestive SystemDocument3 pagesDigestive SystemkhakimagdalenaNo ratings yet
- Lec - Activity16 and 17 - Digestive - SystemDocument9 pagesLec - Activity16 and 17 - Digestive - SystemPrancheska Abigayle Peneyra SantiagoNo ratings yet
- Digestive System NotesDocument40 pagesDigestive System NotesSANDIE SORELLENo ratings yet
- The Digestive System 1Document28 pagesThe Digestive System 1AnnNo ratings yet
- CHAPTER 9 Gastrointestinal SystemDocument7 pagesCHAPTER 9 Gastrointestinal SystemGilianne Balatbat ManuelNo ratings yet
- GI - Anatomy To DiagnosticsDocument39 pagesGI - Anatomy To DiagnosticsIvan FernandezNo ratings yet
- Final: Gluconeogenesis - When The Liver and KidneysDocument43 pagesFinal: Gluconeogenesis - When The Liver and KidneysRashid DayaoNo ratings yet
- Digestive SystemDocument9 pagesDigestive System79ctq9xpf7No ratings yet
- 3.4. Seminar-The Digestive SystemDocument54 pages3.4. Seminar-The Digestive System6f5d6b5r6tNo ratings yet
- The Digestive System and Body MetabolismnotesDocument31 pagesThe Digestive System and Body MetabolismnotesJared Bien TagolimotNo ratings yet
- Anatomy and Physiology of The GIT NotesDocument20 pagesAnatomy and Physiology of The GIT NotesAndreNo ratings yet
- Digestive SystemDocument5 pagesDigestive SystemKate BambalanNo ratings yet
- Gastrointestinal Tract (GIT) - A Continuous Tube That Begins atDocument5 pagesGastrointestinal Tract (GIT) - A Continuous Tube That Begins atBestoon SaifaddinNo ratings yet
- VisibleBody Digestive SystemDocument13 pagesVisibleBody Digestive SystemcascaveletteNo ratings yet
- Functions of The Digestive System: Canines, Premolars, and Molars. Each Tooth Consists of ADocument3 pagesFunctions of The Digestive System: Canines, Premolars, and Molars. Each Tooth Consists of AEmmanuel CuevasNo ratings yet
- Digestive System NewDocument34 pagesDigestive System NewSANDIE SORELLENo ratings yet
- HEALTH ASSESSMENT!!!Digestive SystemDocument24 pagesHEALTH ASSESSMENT!!!Digestive Systemapi-19885395100% (1)
- Digestive System - SummaryDocument15 pagesDigestive System - Summarys.tinaja.marieantonetteNo ratings yet
- Human Anatomy The Gastrointestinal TractDocument53 pagesHuman Anatomy The Gastrointestinal TractGadzikaNo ratings yet
- Pemicu 1 GI GraceDocument146 pagesPemicu 1 GI Gracegrace liwantoNo ratings yet
- Chapter22notes DIGESTIONDocument42 pagesChapter22notes DIGESTIONpancit cantonNo ratings yet
- Bahan Pemicu 1 Gastrointestinal Ivan BuntaraDocument151 pagesBahan Pemicu 1 Gastrointestinal Ivan BuntaraMarco GunawanNo ratings yet
- Digestive SystemDocument10 pagesDigestive SystemJOANNA MARIE INVENTORNo ratings yet
- Digestive System.: Nur112: Anatomy and Physiology ISU Echague - College of NursingDocument9 pagesDigestive System.: Nur112: Anatomy and Physiology ISU Echague - College of NursingWai KikiNo ratings yet
- Pemicu 1 Blok GIT SintaDocument85 pagesPemicu 1 Blok GIT SintasimranNo ratings yet
- Molecular Biology - WikipediaDocument9 pagesMolecular Biology - WikipediaLizbethNo ratings yet
- On Dreams - AristotleDocument10 pagesOn Dreams - AristotleLefeneNo ratings yet
- Archery Parental ConsentDocument1 pageArchery Parental ConsentleightertonprimaryNo ratings yet
- Surgical Drainage of Deep Neck AbscessesDocument27 pagesSurgical Drainage of Deep Neck AbscessesIrma DamayantiNo ratings yet
- 4.daftar PustakaDocument5 pages4.daftar PustakaanggaNo ratings yet
- HFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationDocument16 pagesHFOV - Dragonfly - The Next Primary Mode of Neonatal VentilationflowlineNo ratings yet
- Microbiology Chapter 4 Laboratory Methods Staining Body FluidsDocument19 pagesMicrobiology Chapter 4 Laboratory Methods Staining Body FluidsAkhilesh TiwariNo ratings yet
- Assignment2 PDFDocument4 pagesAssignment2 PDFJavier GonzalezNo ratings yet
- Preparation of Soyabean Milk and ItDocument22 pagesPreparation of Soyabean Milk and Itniki dadhichNo ratings yet
- San Joaquin Resources 2013-2014Document466 pagesSan Joaquin Resources 2013-2014api-22559015No ratings yet
- D M A T: General BuildingsDocument17 pagesD M A T: General BuildingsDeva RajNo ratings yet
- Michael Fraser BookletDocument5 pagesMichael Fraser BookletRushika PurohitNo ratings yet
- Diagnostic Pacing Maneuvers For Supraventricular Tachycardia - Part 2Document13 pagesDiagnostic Pacing Maneuvers For Supraventricular Tachycardia - Part 2aafagihNo ratings yet
- GENERAL BIOLOGY 2 Baby LabDocument10 pagesGENERAL BIOLOGY 2 Baby LabRK MendozaNo ratings yet
- Characterization of Ube Coconut Pulp Muffin Fortified With JuteDocument95 pagesCharacterization of Ube Coconut Pulp Muffin Fortified With JuteroselynmaenavarroNo ratings yet
- Cology of Pediatrics N GeriatricsDocument41 pagesCology of Pediatrics N GeriatricsGANESH KUMAR JELLA100% (1)
- Signature Assignment: Final Draft !1Document17 pagesSignature Assignment: Final Draft !1Allison Van KirkNo ratings yet
- Statistics Related To Child Health.Document34 pagesStatistics Related To Child Health.charan pooniaNo ratings yet
- 29737930Document26 pages29737930MAULIDYA NURUL AINI -No ratings yet
- HISTOPATH FIXATIONdocx PDFDocument8 pagesHISTOPATH FIXATIONdocx PDFmaricel duque100% (1)
- Perihal: Penawaran Harga Set Untuk Laboratorium Pemeriksaan Covid-19 Di Provinsi Banten TA 2021Document2 pagesPerihal: Penawaran Harga Set Untuk Laboratorium Pemeriksaan Covid-19 Di Provinsi Banten TA 2021M A J I D R I M B A N INo ratings yet
- Albumin FS : Order Information Calibrators and ControlsDocument3 pagesAlbumin FS : Order Information Calibrators and ControlsrabiatulNo ratings yet
- GermanyDocument4 pagesGermanyKelz YouknowmynameNo ratings yet