You might also like
- Compound Forming Extractants, Solvating Solvents and Inert Solvents: Iupac Chemical Data SeriesFrom EverandCompound Forming Extractants, Solvating Solvents and Inert Solvents: Iupac Chemical Data SeriesNo ratings yet
- Parameter 20/8 (PKM) 20/8 (RSUP) Nilai Rujukan UnitDocument9 pagesParameter 20/8 (PKM) 20/8 (RSUP) Nilai Rujukan UnitArya PrimanandaNo ratings yet
- Amprahan PICU Sabtu, 20 Feb 2021Document6 pagesAmprahan PICU Sabtu, 20 Feb 2021muhammadrikiNo ratings yet
- Dr. Nicoleta Lefter's bulletin of blood analysisDocument37 pagesDr. Nicoleta Lefter's bulletin of blood analysisMarilena TarcaNo ratings yet
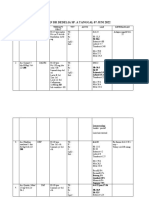
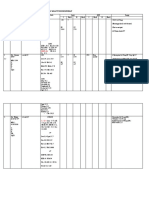
- LAPORAN DR DEDELIADocument3 pagesLAPORAN DR DEDELIAPerawat HolisticNo ratings yet
- Patient Profile Form Department of Pharmacy Practice, Mcops, ManipalDocument4 pagesPatient Profile Form Department of Pharmacy Practice, Mcops, ManipalvarishNo ratings yet
- Follow Up Ruangan Minggu, 28 November 2021 PUKUL 19.30 WIB: No Nama TGL MSK Ruan GAN Diagnosa Hasil LAB Keadaan UmumDocument8 pagesFollow Up Ruangan Minggu, 28 November 2021 PUKUL 19.30 WIB: No Nama TGL MSK Ruan GAN Diagnosa Hasil LAB Keadaan UmumSusyNo ratings yet
- FOLLOW UP RUANGAN: KONDISI PASIENDocument8 pagesFOLLOW UP RUANGAN: KONDISI PASIENSusyNo ratings yet
- Morning:: Dr. Ira Nurasyidah, SP.PDocument13 pagesMorning:: Dr. Ira Nurasyidah, SP.PNur FatimatuzzahraNo ratings yet
- HANDOVER ICU HCU 23 Agustus 2021 PagiDocument4 pagesHANDOVER ICU HCU 23 Agustus 2021 PagiNur Izdihar HadiNo ratings yet
- Pemeriksaan Lab/ Penunjang (09/03) : LapageiDocument6 pagesPemeriksaan Lab/ Penunjang (09/03) : Lapageiipd limabersaudaraNo ratings yet
- Biosynthesis of Steroid Hormones: Dr. Sumreena Mansoor Assistant Prof of BiochemistryDocument49 pagesBiosynthesis of Steroid Hormones: Dr. Sumreena Mansoor Assistant Prof of BiochemistryYumnah BabarNo ratings yet
- Biosystem 1561Document2 pagesBiosystem 1561ShahinNo ratings yet
- Coass: Ilham, Tari, NurhabibahDocument3 pagesCoass: Ilham, Tari, NurhabibahharzalinaNo ratings yet
- Tn. GAOS RekapanDocument35 pagesTn. GAOS RekapanmichaelarshantyNo ratings yet
- GLUCOCORTICOIDS AND METABOLISMDocument34 pagesGLUCOCORTICOIDS AND METABOLISMCrystine SinatraNo ratings yet
- List Pasien Isolasi 08072020 SALAM SEHAT SEMUADocument26 pagesList Pasien Isolasi 08072020 SALAM SEHAT SEMUAsylvesterbenyNo ratings yet
- Pemeriksaan Lab/ Penunjang (05/03)Document4 pagesPemeriksaan Lab/ Penunjang (05/03)ipd limabersaudaraNo ratings yet
- Mindray control sheet with Ranox control valuesDocument2 pagesMindray control sheet with Ranox control valuesShahinNo ratings yet
- No Nama TGL Masuk Ruangan Diagnosa Hasil Lab Keadaan UmumDocument22 pagesNo Nama TGL Masuk Ruangan Diagnosa Hasil Lab Keadaan UmumSusyNo ratings yet
- DUTY SDH + CKDDocument6 pagesDUTY SDH + CKDadelia putri wirandaniNo ratings yet
- List of Plastic Surgery Patients on Thursday March 17th 2016Document2 pagesList of Plastic Surgery Patients on Thursday March 17th 2016asddfggNo ratings yet
- List Onko 6 MaretDocument9 pagesList Onko 6 MaretyongkyNo ratings yet
- IMG 20170617 1 Rep OB PDFDocument5 pagesIMG 20170617 1 Rep OB PDFCris RivasNo ratings yet
- Case Presentation 26 NOVEMBER 2020Document57 pagesCase Presentation 26 NOVEMBER 2020Yosua Butar ButarNo ratings yet
- List Pasien Thovask Jumat 30 Des 2016-1Document5 pagesList Pasien Thovask Jumat 30 Des 2016-1Deviwanti BataraNo ratings yet
- Senin 19 Desember 2016 Irina A Bawah: List Pasien UrologiDocument6 pagesSenin 19 Desember 2016 Irina A Bawah: List Pasien UrologiDeviwanti BataraNo ratings yet
- Handover Icu Hcu 02 September 2021 PagiDocument8 pagesHandover Icu Hcu 02 September 2021 PagizarazobellNo ratings yet
- DK Endokrin Mola OgieDocument51 pagesDK Endokrin Mola OgiehariogieNo ratings yet
- HANDOVER ICU HCU 03 09 2021 SiangDocument9 pagesHANDOVER ICU HCU 03 09 2021 SiangzarazobellNo ratings yet
- Di Indo Cuma DuaDocument2 pagesDi Indo Cuma Duafatimah putriNo ratings yet
- Senin, 29 Januari 2018 Bedah Onkologi: Swr/MowDocument2 pagesSenin, 29 Januari 2018 Bedah Onkologi: Swr/Mowsyaiful_snNo ratings yet
- AnalizeDocument2 pagesAnalizeClaudiaElenaNo ratings yet
- Begapara Premsagar Chowk House No 149 Ward No 6 DURG, 490023: Page: 1 of 17Document17 pagesBegapara Premsagar Chowk House No 149 Ward No 6 DURG, 490023: Page: 1 of 17Dani Shashwat100% (1)
- Clinical Pharmacy Case on CAD ManagementDocument41 pagesClinical Pharmacy Case on CAD ManagementLouie Fernand LegaspiNo ratings yet
- List Pasien Divisi Thovask-1Document5 pagesList Pasien Divisi Thovask-1Anonymous cdJttmLtNo ratings yet
- Sensus Saraf (Rabu, 06 September 2018) : NO Identitas DPJP Diagnosis Tindakan LAB KUDocument4 pagesSensus Saraf (Rabu, 06 September 2018) : NO Identitas DPJP Diagnosis Tindakan LAB KUAbigailGraceNo ratings yet
- FIXx Prof SY 03 Desember 2022Document6 pagesFIXx Prof SY 03 Desember 2022Fitri DicyNo ratings yet
- Pemeriksaan Lab/ Penunjang (10/03) : LapageiDocument8 pagesPemeriksaan Lab/ Penunjang (10/03) : Lapageiipd limabersaudaraNo ratings yet
- Coass: Aprita, Yana, Ejil, LentiDocument2 pagesCoass: Aprita, Yana, Ejil, LentiEjil HastiaNo ratings yet
- TN KoesrinDocument5 pagesTN KoesrinCristian RajagukgukNo ratings yet
- Cor Prominent Susp. Pneumonia, Mohon Korelasi Klinis Old Fracture Os Clavicula Kiri 1/3 TengahDocument3 pagesCor Prominent Susp. Pneumonia, Mohon Korelasi Klinis Old Fracture Os Clavicula Kiri 1/3 TengahMade SetiadjiNo ratings yet
- HPLC Isolation and Gc-Ms Characterization of A Compound Strongly Cross Reacting With Tetrahydroaldosterone AntiserumDocument12 pagesHPLC Isolation and Gc-Ms Characterization of A Compound Strongly Cross Reacting With Tetrahydroaldosterone AntiserumAnonymous m35iKgHNo ratings yet
- List Pasien Orthopedi 1 Oktober 2017Document19 pagesList Pasien Orthopedi 1 Oktober 2017Meidy RengkuanNo ratings yet
- 241221041419PMC21-9758Document2 pages241221041419PMC21-9758Ayesha SafeerNo ratings yet
- LIST OF PATIENTS IN THE CARDIOLOGY WARDDocument2 pagesLIST OF PATIENTS IN THE CARDIOLOGY WARDVini MalekeNo ratings yet
- HANDOVER ICU HCU 03 09 2021 PagiDocument8 pagesHANDOVER ICU HCU 03 09 2021 PagizarazobellNo ratings yet
- IRNA MEDIK - Pandan Wangi - Fini FirdiniDocument9 pagesIRNA MEDIK - Pandan Wangi - Fini Firdiniriska santri utamiNo ratings yet
- List Pasien Thovask Kamis 29 Des 2016Document5 pagesList Pasien Thovask Kamis 29 Des 2016Deviwanti BataraNo ratings yet
- Follow Up Ruangan Senin, 6 Desember 2021 PUKUL 19.30 WIB: No Nama TGL MSK Ruan GAN Diagnosa Hasil LAB Keadaan UmumDocument11 pagesFollow Up Ruangan Senin, 6 Desember 2021 PUKUL 19.30 WIB: No Nama TGL MSK Ruan GAN Diagnosa Hasil LAB Keadaan UmumSusyNo ratings yet
- Pathology Test Results Show Liver Abscess and Pleural EffusionDocument3 pagesPathology Test Results Show Liver Abscess and Pleural EffusionAngilie de AlbaNo ratings yet
- Amprahan HCU Kamis Pagi, 15 Februari 2024Document6 pagesAmprahan HCU Kamis Pagi, 15 Februari 2024alfaz zamzamiNo ratings yet
- Er Morning Report Saturday Night, March 9 2019Document8 pagesEr Morning Report Saturday Night, March 9 2019Evan AninditoNo ratings yet
- Resident Admission NoteDocument3 pagesResident Admission NoteAli El SafadiNo ratings yet
- Ovoran NICU III Minggu Pagi 16 Juli 2023Document7 pagesOvoran NICU III Minggu Pagi 16 Juli 2023juliNo ratings yet
- STT Mä CK Giá Nhóm Ghi Chu 26-Aug: 1 (CK, HTY, CNTT, DP) 2 (ĐTC, XD, VLXD) 3 (PB, HC, CS, NĐ) 4 (K)Document2 pagesSTT Mä CK Giá Nhóm Ghi Chu 26-Aug: 1 (CK, HTY, CNTT, DP) 2 (ĐTC, XD, VLXD) 3 (PB, HC, CS, NĐ) 4 (K)Nam HoaiNo ratings yet
- Pasien IhcDocument27 pagesPasien IhcM. Eka PutraNo ratings yet
- FFP Tranfusion in A 31-Year-Old Patient With Eclampsia: Hariogie Putradi Moderator: Dr. Siti Fatonah, Sp. PKDocument193 pagesFFP Tranfusion in A 31-Year-Old Patient With Eclampsia: Hariogie Putradi Moderator: Dr. Siti Fatonah, Sp. PKhariogieNo ratings yet
- Hepatitis C Case AZOTEMIA Positive AntiHCVDocument31 pagesHepatitis C Case AZOTEMIA Positive AntiHCVtorajasaNo ratings yet
- COVID-19 Test Results and Cardiac Echo FindingsDocument3 pagesCOVID-19 Test Results and Cardiac Echo FindingsJames Raynel NonanNo ratings yet
- 2020 Review PIC - Uniform PolicyDocument2 pages2020 Review PIC - Uniform Policymonday125No ratings yet
- Annals 1368 001Document9 pagesAnnals 1368 001monday125No ratings yet
- ADMA 2010 BlackboardDocument41 pagesADMA 2010 Blackboardmonday125No ratings yet
- Acupuncture PDFDocument14 pagesAcupuncture PDFmonday125No ratings yet
- Caffeine BronchodilatorDocument30 pagesCaffeine Bronchodilatormonday125No ratings yet
- 2010 - Zhang - EAP For AR Review PDFDocument8 pages2010 - Zhang - EAP For AR Review PDFmonday125No ratings yet
- Business Case For A New Consultant Chemical Pathology Final VersionDocument11 pagesBusiness Case For A New Consultant Chemical Pathology Final Versionmonday125No ratings yet
- Become Healthy or Extinct Darryl DsouzaDocument180 pagesBecome Healthy or Extinct Darryl Dsouzacontactsm100% (1)
- Les Perry How Do We Define An Adequate Response To SynacthenDocument66 pagesLes Perry How Do We Define An Adequate Response To Synacthenmonday125No ratings yet
- Clinical Guideline For Anticoagulant Use in AdultsDocument108 pagesClinical Guideline For Anticoagulant Use in Adultsmonday125No ratings yet
- Acupuncture in Modern MedicineDocument400 pagesAcupuncture in Modern Medicinepranav100% (2)
- ST Agnes Catholic Primary SchoolDocument12 pagesST Agnes Catholic Primary Schoolmonday125No ratings yet
- Karen Smith Duty Biochemist ScenariosDocument43 pagesKaren Smith Duty Biochemist Scenariosmonday125100% (2)
- Pleasing Her Husband's Boss (Hot Wife and Her Cuckold 2) by Michaels DeanaDocument29 pagesPleasing Her Husband's Boss (Hot Wife and Her Cuckold 2) by Michaels Deanamonday12560% (10)
- Uric AcidDocument6 pagesUric Acidmonday125100% (1)
- JonathanLandsman VitaminToKillVirusesDocument18 pagesJonathanLandsman VitaminToKillVirusesPortugal ForenseNo ratings yet
- Les Perry How Do We Define An Adequate Response To SynacthenDocument66 pagesLes Perry How Do We Define An Adequate Response To Synacthenmonday125No ratings yet
- ICP-MS Talk ACBDocument31 pagesICP-MS Talk ACBmonday125No ratings yet
- Bible 2018Document183 pagesBible 2018monday125No ratings yet
- Oil Pulling A Traditional Method On The Edge of EvDocument4 pagesOil Pulling A Traditional Method On The Edge of Evmonday125No ratings yet
- DRDocument17 pagesDRmonday125No ratings yet
- OspeDocument29 pagesOspemonday125No ratings yet
- Trisomy ScreeningDocument55 pagesTrisomy Screeningmonday125No ratings yet
- 1 s2.0 S0753332218345657 MainDocument11 pages1 s2.0 S0753332218345657 Mainmonday125No ratings yet
- FRCPath OSPE Questions and AnswersDocument11 pagesFRCPath OSPE Questions and Answersmonday125No ratings yet
- FOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'sDocument19 pagesFOCUS SAS Training Day Leeds Dr. Joanna Sheldon Protein Reference Unit, St. George'smonday125No ratings yet
- Writing An Abstract: Sally - Benton@bartshealth - Nhs.ukDocument7 pagesWriting An Abstract: Sally - Benton@bartshealth - Nhs.ukmonday125No ratings yet
- DRDocument17 pagesDRmonday125No ratings yet
- SasDocument8 pagesSasmonday125No ratings yet
- Critical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)Document10 pagesCritical Appraisal: DR A C J Hutchesson Chair of Examiners' Panel, Frcpath (Clinical Biochemistry)monday125No ratings yet
- 2.1.1.1. Aguilar and Stiles' Experiment.: Visual Adaptation and Retinal G A I N Controls 2 7 7Document1 page2.1.1.1. Aguilar and Stiles' Experiment.: Visual Adaptation and Retinal G A I N Controls 2 7 7AkicaNo ratings yet
- 131 Malignant HyperthermiaDocument6 pages131 Malignant Hyperthermiasulai701280No ratings yet
- Why Is Important To Drinking A Lot of Water?: Veny Khairani Annadiyah Xi Mipa 7 / 34Document2 pagesWhy Is Important To Drinking A Lot of Water?: Veny Khairani Annadiyah Xi Mipa 7 / 34Veni Khairani AnnadiaNo ratings yet
- Soul of Remedies - Introduction - TamilDocument3 pagesSoul of Remedies - Introduction - Tamilfly2suganyaNo ratings yet
- Swimming Pool SanitationDocument3 pagesSwimming Pool SanitationselennelaimitoNo ratings yet
- Efficacy of Garlic Based Treatments Against Monogenean Parasites Infecting The Guppy Poecilia Reticulata PetersDocument8 pagesEfficacy of Garlic Based Treatments Against Monogenean Parasites Infecting The Guppy Poecilia Reticulata PetersGabri ElaNo ratings yet
- Reversible Dementia and DeliriumDocument65 pagesReversible Dementia and Deliriummpm8471No ratings yet
- Neurotics Anonymous Test of Mental and Emotional HealthDocument2 pagesNeurotics Anonymous Test of Mental and Emotional Healthcraigt90% (10)
- Skor Tokolitik PDFDocument5 pagesSkor Tokolitik PDFrahayu muhsiNo ratings yet
- Trabeculectomy Dictation GuideDocument2 pagesTrabeculectomy Dictation GuideErik Anderson MDNo ratings yet
- How To Get Appointed Ocn370397207Document46 pagesHow To Get Appointed Ocn370397207api-241896162No ratings yet
- The Herbaceous Notes of FragranceDocument0 pagesThe Herbaceous Notes of FragranceosamamusaNo ratings yet
- Study of Prevelance of Rhesus (RH) Blood Group Antigens Profiling Among Blood DonorsDocument7 pagesStudy of Prevelance of Rhesus (RH) Blood Group Antigens Profiling Among Blood Donorsindu mathiNo ratings yet
- Mispa Count Plus Service ManualDocument331 pagesMispa Count Plus Service Manuallemanhcuong1503No ratings yet
- 2012 Pittsburgh Black Business Directory PDFDocument104 pages2012 Pittsburgh Black Business Directory PDFMhacblink ManNo ratings yet
- Anti-Dopamine D2 Receptor Antibody Ab30743 Anti-Dopamine D2 Receptor Antibody Ab30743Document3 pagesAnti-Dopamine D2 Receptor Antibody Ab30743 Anti-Dopamine D2 Receptor Antibody Ab30743Michael DaleyNo ratings yet
- CFO Controller Healthcare Financial Reporting in Dallas TX Resume Michael ExlineDocument2 pagesCFO Controller Healthcare Financial Reporting in Dallas TX Resume Michael ExlineMichaelExlineNo ratings yet
- An Introduction To Anatomy and Physiology MidwiferyDocument108 pagesAn Introduction To Anatomy and Physiology MidwiferyGayuh Kartika100% (3)
- Anemia PPT 2Document1 pageAnemia PPT 2Uzma TahseenNo ratings yet
- B.SC in Operation Theatre and Anesthesia Technology PDFDocument24 pagesB.SC in Operation Theatre and Anesthesia Technology PDFIqbal HarzikyNo ratings yet
- 3Document5 pages3Reg ArbotanteNo ratings yet
- Management of Osteoporosis and Bone Pain Calcitonin Nasal Spray-CalcisprayDocument30 pagesManagement of Osteoporosis and Bone Pain Calcitonin Nasal Spray-CalcisprayLeo FluxNo ratings yet
- Benefits of Alkaline Water EbookDocument58 pagesBenefits of Alkaline Water Ebookanitabillion100% (3)
- Celiac Disease: An Autoimmune Condition Triggered by GlutenDocument2 pagesCeliac Disease: An Autoimmune Condition Triggered by GlutenGiabellNo ratings yet
- Study of Dosage Laws in HomeopathyDocument27 pagesStudy of Dosage Laws in HomeopathydrdivishNo ratings yet
- Prevalence of Dysmenorrhea Among Medical StudentsDocument3 pagesPrevalence of Dysmenorrhea Among Medical StudentsNovia ambarwatiNo ratings yet
- Cyst of Jaws-RadiologyDocument60 pagesCyst of Jaws-RadiologyshabeelpnNo ratings yet
- StyleitalianoDocument11 pagesStyleitalianoDemmy WijayaNo ratings yet
- Safe antibiotics for rabbits skin issuesDocument7 pagesSafe antibiotics for rabbits skin issuesSk LoonaNo ratings yet
- 2nd Announcement JakNews 2024Document19 pages2nd Announcement JakNews 2024Nando EllaNo ratings yet