You might also like
- Disorders of The Integumentary System: Internet ResourcesDocument4 pagesDisorders of The Integumentary System: Internet ResourcesDylan Dela CruzNo ratings yet
- Postherpetic Neuralgia ReferatDocument24 pagesPostherpetic Neuralgia Referatnerissa rahadianthiNo ratings yet
- Herpes ZosterDocument2 pagesHerpes ZosterNeweeJoonYowNo ratings yet
- Communicable Diseases of Childhoo1Document3 pagesCommunicable Diseases of Childhoo1esmirikNo ratings yet
- Herpes Z Oster Clinical PresentationDocument50 pagesHerpes Z Oster Clinical PresentationS KkNo ratings yet
- Notes On Herpes ZosterDocument13 pagesNotes On Herpes ZosterSaleh Mohammad ShoaibNo ratings yet
- Dermatology Lectures JRRMMCDocument10 pagesDermatology Lectures JRRMMCGi Em100% (1)
- World University of Bangladesh: "Herpes Zoster''Document3 pagesWorld University of Bangladesh: "Herpes Zoster''MD REFATNo ratings yet
- Classification Criteria For SLEDocument2 pagesClassification Criteria For SLEA. DuqueNo ratings yet
- Top Up Training Center and Research Consultancy Communicable Disease NursingDocument3 pagesTop Up Training Center and Research Consultancy Communicable Disease NursingSTEFFI GABRIELLE GOLEZNo ratings yet
- Burns AmbossDocument9 pagesBurns AmbossPati MuresanNo ratings yet
- Burns AmbossDocument9 pagesBurns AmbossPati MuresanNo ratings yet
- PsoriasisDocument27 pagesPsoriasisNikkaDablioNo ratings yet
- ShinglesDocument1 pageShinglesAlan Z. GianNo ratings yet
- Herpes Zoster Treatment GuidelinesDocument19 pagesHerpes Zoster Treatment GuidelinesMaha KhalidNo ratings yet
- Classification Criteria For SLEDocument4 pagesClassification Criteria For SLEofva26No ratings yet
- CPAT3201 2020 Inflammation Lecture 1 NOTESDocument50 pagesCPAT3201 2020 Inflammation Lecture 1 NOTESJoshua KaoNo ratings yet
- Varicella Vaccine EffectivenessDocument21 pagesVaricella Vaccine EffectivenessSul FadlyNo ratings yet
- Case Analysis Herpes ZosterDocument16 pagesCase Analysis Herpes ZosterRobbyNo ratings yet
- Guide ZonaOphtalmique Web EN VFDocument6 pagesGuide ZonaOphtalmique Web EN VFsiti rumaisaNo ratings yet
- BENIGN & MALIGNANT LESIONS OF THE SKIN by AlbraaDocument7 pagesBENIGN & MALIGNANT LESIONS OF THE SKIN by AlbraaZoi PapadatouNo ratings yet
- Herpes Zoster: Bing-Rong ZHOUDocument43 pagesHerpes Zoster: Bing-Rong ZHOUMichael Jansen Sulaiman100% (1)
- Herpes Zoster (Shingles/Acute Posterior Ganglionitis)Document13 pagesHerpes Zoster (Shingles/Acute Posterior Ganglionitis)Shawn Michael SwayzeNo ratings yet
- Colorful PPT Herpes ZosterDocument16 pagesColorful PPT Herpes Zosterekasepriani_chanNo ratings yet
- Classification Criteria For SLE PDFDocument4 pagesClassification Criteria For SLE PDFCocea MihaiNo ratings yet
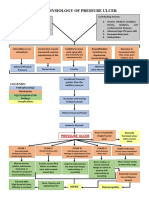
- Pathophysiology of Pressure UlcersDocument1 pagePathophysiology of Pressure UlcersSTORAGE FILENo ratings yet
- Lower Genital Infections GuideDocument2 pagesLower Genital Infections Guidecbac1990No ratings yet
- How to look 「皮疹」Document50 pagesHow to look 「皮疹」Satoshi KobayashiNo ratings yet
- ImportantDocument21 pagesImportantGaurav pareekNo ratings yet
- BURNSDocument26 pagesBURNSGaurav pareekNo ratings yet
- Community nursing: Wound care and tissue viabilityDocument59 pagesCommunity nursing: Wound care and tissue viabilityIlyes RaniNo ratings yet
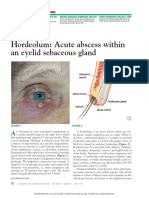
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Vascular Reactions and Sunburn EffectsDocument11 pagesVascular Reactions and Sunburn EffectsJolaine ValloNo ratings yet
- PHN (Dr. Ken) - DikonversiDocument32 pagesPHN (Dr. Ken) - DikonversiwkwkwkhhhhNo ratings yet
- Pain Syndromes Pain: Chronic Regional Pain SyndromeDocument3 pagesPain Syndromes Pain: Chronic Regional Pain SyndromeAlyssa BatasNo ratings yet
- Chickenpox: VaricellaDocument3 pagesChickenpox: VaricellaPauline Mae RobertoNo ratings yet
- Herpes Zoster: Nurul Iska Ulmarika Idrisc111 10 831 Ruth Faustine J. Rayo C 1 1 1 1 0 1 8 0Document26 pagesHerpes Zoster: Nurul Iska Ulmarika Idrisc111 10 831 Ruth Faustine J. Rayo C 1 1 1 1 0 1 8 0fatqur280% (1)
- Tinywow Communicable-Diseases 48897647 12Document1 pageTinywow Communicable-Diseases 48897647 12JULIUS CEZAR QUINAYNo ratings yet
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- Herpez Zoster Dan PHNDocument16 pagesHerpez Zoster Dan PHNRizky FatimahNo ratings yet
- 24 - Fever and RashDocument16 pages24 - Fever and RashPREEDIPAT PHINTHIPNo ratings yet
- Etiology and Pathogenesis of Urticaria and AngioedemaDocument34 pagesEtiology and Pathogenesis of Urticaria and AngioedemaNUR NATHANIANo ratings yet
- HHV3 Infections: Chickenpox and ShinglesDocument6 pagesHHV3 Infections: Chickenpox and ShinglesShuvashishSunuwarNo ratings yet
- Manajemen NyeriDocument30 pagesManajemen NyericlvpratamaNo ratings yet
- Vulvar Pruritus and Lichen Simplex ChronicusDocument10 pagesVulvar Pruritus and Lichen Simplex Chronicustiok widodoNo ratings yet
- Integumentary SystemDocument4 pagesIntegumentary SystemArnie Jean SalazarNo ratings yet
- Genital HerpesDocument29 pagesGenital HerpesGliza Jane100% (1)
- ProActive Training CaseStudy 5Document8 pagesProActive Training CaseStudy 5danthemanyvrNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- Physiology of Pain Pathways and Its Modulation: DR HassanDocument79 pagesPhysiology of Pain Pathways and Its Modulation: DR HassanvaishnaviNo ratings yet
- Bacterial Skin InfectionDocument4 pagesBacterial Skin InfectionAngeline TaghapNo ratings yet
- MANAGING PAIN: NON-PHARMACOLOGICAL AND PHARMACOLOGICAL STRATEGIESDocument30 pagesMANAGING PAIN: NON-PHARMACOLOGICAL AND PHARMACOLOGICAL STRATEGIESCitra AnggrainiNo ratings yet
- Rashes: Paediatric Dermatology: Ellis HonDocument95 pagesRashes: Paediatric Dermatology: Ellis HonB AuNo ratings yet
- Viral Disease 2021Document76 pagesViral Disease 2021Ageng betaNo ratings yet
- Epidemiology of Snake BitesDocument19 pagesEpidemiology of Snake BitesJonathan JumalonNo ratings yet
- Bacterial Skin Infections: Cellulitis Case and OverviewDocument75 pagesBacterial Skin Infections: Cellulitis Case and OverviewmasithaNo ratings yet
- Cims Case 1 - SGD A4Document16 pagesCims Case 1 - SGD A4SGD A4No ratings yet
- Guideline for Managing Herpes Zoster and PHN in Older AdultsDocument54 pagesGuideline for Managing Herpes Zoster and PHN in Older AdultsFitria Intan BeladinaNo ratings yet
- A Simple Guide to Pruritis (Itch), Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pruritis (Itch), Diagnosis, Treatment and Related ConditionsNo ratings yet
- Herpes Zoster, (Shingles) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHerpes Zoster, (Shingles) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (17)
- Enhancing Rigor in Quantitative ResearchDocument21 pagesEnhancing Rigor in Quantitative ResearchIzhra MargateNo ratings yet
- Bemonc: Basic Emergency Obstetric and Newborn CareDocument32 pagesBemonc: Basic Emergency Obstetric and Newborn CareIzhra MargateNo ratings yet
- Reviewing of Related LiteratureDocument15 pagesReviewing of Related LiteratureIzhra MargateNo ratings yet
- Drug Mechanism, Indications, Side Effects & Nursing CareDocument16 pagesDrug Mechanism, Indications, Side Effects & Nursing Careclydell joyce masiarNo ratings yet
- Understanding Mixed Methods Research DesignsDocument19 pagesUnderstanding Mixed Methods Research DesignsIzhra MargateNo ratings yet
- ETHICAL RESEARCH GUIDELINESDocument12 pagesETHICAL RESEARCH GUIDELINESIzhra MargateNo ratings yet
- SDG'SDocument24 pagesSDG'SIzhra MargateNo ratings yet
- Philippine Reproductive HealthDocument14 pagesPhilippine Reproductive HealthIzhra MargateNo ratings yet
- Formulating Theoretical/Concep Tual FrameworksDocument33 pagesFormulating Theoretical/Concep Tual FrameworksIzhra MargateNo ratings yet
- Ano It DengueDocument1 pageAno It DengueIzhra MargateNo ratings yet
- REDCOPDocument4 pagesREDCOPIzhra MargateNo ratings yet
- Well Baby FNCPDocument7 pagesWell Baby FNCPIzhra MargateNo ratings yet
- Bemonc: Basic Emergency Obstetric and Newborn CareDocument32 pagesBemonc: Basic Emergency Obstetric and Newborn CareIzhra MargateNo ratings yet
- Health and Wellnes ProgramsDocument12 pagesHealth and Wellnes ProgramsIzhra Margate100% (1)
- Women's and Children's Rights GuideDocument10 pagesWomen's and Children's Rights GuideIzhra MargateNo ratings yet
- FilariasisDocument23 pagesFilariasisIzhra MargateNo ratings yet
- FASCIOLOPSIASISDocument12 pagesFASCIOLOPSIASISIzhra MargateNo ratings yet
- Bemonc: Basic Emergency Obstetric and Newborn CareDocument32 pagesBemonc: Basic Emergency Obstetric and Newborn CareIzhra MargateNo ratings yet
- FilariasisDocument23 pagesFilariasisIzhra MargateNo ratings yet
- Air PollutionDocument14 pagesAir PollutionIzhra MargateNo ratings yet
- National Voluntary Blood Services Program OverviewDocument9 pagesNational Voluntary Blood Services Program OverviewIzhra MargateNo ratings yet
- SHINGLESDocument27 pagesSHINGLESIzhra MargateNo ratings yet
- NUTRIDocument19 pagesNUTRIIzhra MargateNo ratings yet
- SHINGLESDocument27 pagesSHINGLESIzhra MargateNo ratings yet
- LeprosyDocument18 pagesLeprosyIzhra MargateNo ratings yet
- Drug StudyDocument2 pagesDrug StudyIzhra MargateNo ratings yet
- Domestic ViolenceDocument15 pagesDomestic ViolenceIzhra MargateNo ratings yet
- GIARDIASISDocument16 pagesGIARDIASISIzhra MargateNo ratings yet
- LeprosyDocument18 pagesLeprosyIzhra MargateNo ratings yet
- PERTUSSISDocument29 pagesPERTUSSISIzhra MargateNo ratings yet