You might also like
- Hematocrit of ChickensDocument5 pagesHematocrit of ChickensRowzFerlTanutanNo ratings yet
- Problems On Cell KineticsDocument2 pagesProblems On Cell KineticsRazzilGan100% (1)
- Algas en SalamandrasDocument1 pageAlgas en Salamandrasdavidfer122367No ratings yet
- Protein ElectrophoresisDocument5 pagesProtein ElectrophoresisElissiaNo ratings yet
- Thursday Jan 31Document2 pagesThursday Jan 31api-447201619No ratings yet
- 10- Chapter 6Document24 pages10- Chapter 6Ziad Lutfi AlTahaynehNo ratings yet
- Foodlog Date Thursday February 9thDocument4 pagesFoodlog Date Thursday February 9thapi-654020081No ratings yet
- Foodlog Date Sunday February 5thDocument4 pagesFoodlog Date Sunday February 5thapi-654020081No ratings yet
- Pakan AbiDocument4 pagesPakan AbiZuhriya SholichahNo ratings yet
- LCR20070416B6Document2 pagesLCR20070416B6api-26938624No ratings yet
- Looriegelman and Comp. Application in BiopharmaceuticsDocument22 pagesLooriegelman and Comp. Application in BiopharmaceuticsTushar Bambharoliya100% (1)
- Metabolism 2020Document11 pagesMetabolism 2020aidsNo ratings yet
- Foodlog Date Monday February 6thDocument4 pagesFoodlog Date Monday February 6thapi-654020081No ratings yet
- Foodlog Date Wednesday February 8thDocument4 pagesFoodlog Date Wednesday February 8thapi-654020081No ratings yet
- Nutrient profiles of 17 peanut meal samplesDocument5 pagesNutrient profiles of 17 peanut meal samplesAhmed IsmailNo ratings yet
- 589 FullDocument10 pages589 Fullkaiyeung0818No ratings yet
- (Bivalvia: Mactracea) - PHD Thesis: Glasgow Theses Service Theses@Gla - Ac.UkDocument275 pages(Bivalvia: Mactracea) - PHD Thesis: Glasgow Theses Service Theses@Gla - Ac.UkKamsiah 2204124481No ratings yet
- Spring ExperimentDocument12 pagesSpring ExperimentHoussam HijaziNo ratings yet
- Thursday 1Document3 pagesThursday 1api-541251641No ratings yet
- Etextbook PDF For Prokaryotic Metabolism and Physiology 2nd EditionDocument61 pagesEtextbook PDF For Prokaryotic Metabolism and Physiology 2nd Editionvirginia.boles45998% (41)
- Foodlog Date Feb 5 2024 - Daily IntakeDocument1 pageFoodlog Date Feb 5 2024 - Daily Intakeapi-732519743No ratings yet
- Chapter 5: Factor Analysis: 5.1 KMO & Bartlett's TestDocument7 pagesChapter 5: Factor Analysis: 5.1 KMO & Bartlett's TestRayhan TanvirNo ratings yet
- February 9 - Sheet1Document1 pageFebruary 9 - Sheet1api-447547104No ratings yet
- Donoghue1999 PDFDocument23 pagesDonoghue1999 PDFAngélica SánchezNo ratings yet
- Foodlog - 02 07 2024Document1 pageFoodlog - 02 07 2024api-731983167No ratings yet
- 2021 - Starvation Ketosis and The KidneyDocument12 pages2021 - Starvation Ketosis and The KidneyambiebieNo ratings yet
- Lab 12 Energy Metabolism Jan 2010 - Phee Choon Ning ShamaneDocument12 pagesLab 12 Energy Metabolism Jan 2010 - Phee Choon Ning Shamanethe bungalowvideotapesNo ratings yet
- Tugas Rancob Sesudah RakDocument2 pagesTugas Rancob Sesudah RakHuda AnugrahNo ratings yet
- Foodlog Date 2 01 - Daily IntakeDocument1 pageFoodlog Date 2 01 - Daily Intakeapi-655785393No ratings yet
- Solubility of Propylene in WaterDocument2 pagesSolubility of Propylene in WaterMauricioNo ratings yet
- Febuary 1 - Sheet1Document1 pageFebuary 1 - Sheet1api-447547104No ratings yet
- Enrichment Exam in StatisticsDocument9 pagesEnrichment Exam in StatisticsMary Rose LinihanNo ratings yet
- Proteinsparing Effect of Carbohydrate PDFDocument8 pagesProteinsparing Effect of Carbohydrate PDFNurmaNo ratings yet
- Foodlog Date 02Document1 pageFoodlog Date 02api-732026573No ratings yet
- Foodlogtemplate 6Document2 pagesFoodlogtemplate 6api-447432225No ratings yet
- Anti-inflammatory compounds from marine spongeDocument21 pagesAnti-inflammatory compounds from marine spongeFransisca PutriNo ratings yet
- Inter SHDocument6 pagesInter SHAkmal FadilandaNo ratings yet
- Foodlog Date 2 11 - Daily IntakeDocument1 pageFoodlog Date 2 11 - Daily Intakeapi-733085568No ratings yet
- Experiment 1: University of BalamandDocument11 pagesExperiment 1: University of Balamandlaura sageNo ratings yet
- Enrichment Exam in StatisticsDocument8 pagesEnrichment Exam in StatisticsMary Rose LinihanNo ratings yet
- Marcet Boiler ReportDocument20 pagesMarcet Boiler Reportalwaysbethere100% (1)
- Nutrient Requirements of Beef Cattle: WWW - Aces.eduDocument8 pagesNutrient Requirements of Beef Cattle: WWW - Aces.eduFajar Sang RevolusionerNo ratings yet
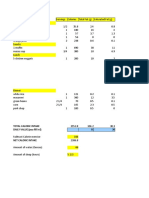
- Total Caloric Intake DAILY VALUE (You Fill In!)Document1 pageTotal Caloric Intake DAILY VALUE (You Fill In!)api-656419377No ratings yet
- WJEC 2014 Online Exam Review: GCSE Biology 4461-02Document29 pagesWJEC 2014 Online Exam Review: GCSE Biology 4461-02XPhysixZNo ratings yet
- Fermentation Lab ReportDocument8 pagesFermentation Lab ReportSarah Sulon77% (13)
- Growth of Escherichia Coli in A 5 Litre Batch Fermentation VesselDocument15 pagesGrowth of Escherichia Coli in A 5 Litre Batch Fermentation VesselAs'ad Mughal100% (2)
- Macronutrients Metabolism in ObesityDocument20 pagesMacronutrients Metabolism in ObesityMuhammad IqbalNo ratings yet
- Poultry Production Feasibility StudyDocument3 pagesPoultry Production Feasibility StudyJessica Jane PueblasNo ratings yet
- 4 5852862929099032890Document23 pages4 5852862929099032890Elteyb Nor eldaimNo ratings yet
- PK SolverDocument23 pagesPK SolverRusydinaNo ratings yet
- Food 1 27Document1 pageFood 1 27api-595139710No ratings yet
- Isolation Purification and Mass Production of ProtDocument7 pagesIsolation Purification and Mass Production of ProtYen DuongNo ratings yet
- Macronutrient Calculator 1Document2 pagesMacronutrient Calculator 1Andrey CaroNo ratings yet
- Daya Cerna Protein Bagian 1Document16 pagesDaya Cerna Protein Bagian 1Septa IndrizaNo ratings yet
- Kinetics of selective glucose fermentation using yeastDocument12 pagesKinetics of selective glucose fermentation using yeastIva Maicol Saavedra BecerraNo ratings yet
- Advanced Dairy Science and TechnologyFrom EverandAdvanced Dairy Science and TechnologyTrevor BritzNo ratings yet
- Physiological Ecology: How Animals Process Energy, Nutrients, and ToxinsFrom EverandPhysiological Ecology: How Animals Process Energy, Nutrients, and ToxinsNo ratings yet
- Advanced Catalysts and Nanostructured Materials: Modern Synthetic MethodsFrom EverandAdvanced Catalysts and Nanostructured Materials: Modern Synthetic MethodsNo ratings yet
- By Michael Somogyi. Laboratory: (From The of Biological Chemistry, Washington University Medical School, St. L, Ouis.)Document15 pagesBy Michael Somogyi. Laboratory: (From The of Biological Chemistry, Washington University Medical School, St. L, Ouis.)gibrambo5770No ratings yet
- Parallel Programming PresentationDocument66 pagesParallel Programming Presentationgibrambo5770No ratings yet
- Raw Milk Quality - Milk Flavor: Kansas Agricultural Experiment Station Research ReportsDocument6 pagesRaw Milk Quality - Milk Flavor: Kansas Agricultural Experiment Station Research Reportsgibrambo5770No ratings yet
- Deep Learning: Early Work Why Deep Learning Stacked Auto Encoders Deep Belief NetworksDocument33 pagesDeep Learning: Early Work Why Deep Learning Stacked Auto Encoders Deep Belief Networksgibrambo5770No ratings yet
- BiPAC 8800AXL FM 2.32c.7 4.UM 1 04 PDFDocument230 pagesBiPAC 8800AXL FM 2.32c.7 4.UM 1 04 PDFgibrambo5770No ratings yet
- J. Biol. Chem.-1951-Somogyi-859-71Document14 pagesJ. Biol. Chem.-1951-Somogyi-859-71gibrambo5770No ratings yet
- Improved Copper Reagents for Sugar DeterminationDocument6 pagesImproved Copper Reagents for Sugar Determinationgibrambo5770No ratings yet
- Food Cravings and Habit Chart PDFDocument2 pagesFood Cravings and Habit Chart PDFgibrambo5770No ratings yet
- J. Biol. Chem. 1940 Somogyi 315 8Document5 pagesJ. Biol. Chem. 1940 Somogyi 315 8gibrambo5770No ratings yet
- J. Biol. Chem.-1943-Stark-319-25Document8 pagesJ. Biol. Chem.-1943-Stark-319-25gibrambo5770No ratings yet
- Effects of intravenous insulin on peripheral glucose assimilation during hyperglycemiaDocument10 pagesEffects of intravenous insulin on peripheral glucose assimilation during hyperglycemiagibrambo5770No ratings yet
- J. Biol. Chem.-1948-Somogyi-597-603Document8 pagesJ. Biol. Chem.-1948-Somogyi-597-603gibrambo5770No ratings yet
- J. Biol. Chem.-1949-Somogyi-217-33Document18 pagesJ. Biol. Chem.-1949-Somogyi-217-33gibrambo5770No ratings yet
- J. Biol. Chem.-1948-Somogyi-597-603Document8 pagesJ. Biol. Chem.-1948-Somogyi-597-603gibrambo5770No ratings yet
- J. Biol. Chem.-1943-Stark-721-30Document11 pagesJ. Biol. Chem.-1943-Stark-721-30gibrambo5770No ratings yet
- J. Biol. Chem.-1951-Somogyi-859-71Document13 pagesJ. Biol. Chem.-1951-Somogyi-859-71gibrambo5770No ratings yet
- J. Biol. Chem.-1943-Stark-731-6Document7 pagesJ. Biol. Chem.-1943-Stark-731-6gibrambo5770No ratings yet
- J. Biol. Chem.-1937-Somogyi-741-7Document8 pagesJ. Biol. Chem.-1937-Somogyi-741-7gibrambo5770No ratings yet
- J. Biol. Chem. 1942 Somogyi 575 9Document6 pagesJ. Biol. Chem. 1942 Somogyi 575 9gibrambo5770No ratings yet
- J. Biol. Chem.-1941-Weichselbaum-5-20Document17 pagesJ. Biol. Chem.-1941-Weichselbaum-5-20gibrambo5770No ratings yet
- J. Biol. Chem.-1941-Somogyi-219-27Document10 pagesJ. Biol. Chem.-1941-Somogyi-219-27gibrambo5770No ratings yet
- Fermentation Rates of Maltose and Glucose in Alkaline SolutionsDocument7 pagesFermentation Rates of Maltose and Glucose in Alkaline Solutionsgibrambo5770No ratings yet
- J. Biol. Chem.-1938-Somogyi-179-87Document10 pagesJ. Biol. Chem.-1938-Somogyi-179-87gibrambo5770No ratings yet
- J. Biol. Chem. 1940 Weichselbaum 343 56Document15 pagesJ. Biol. Chem. 1940 Weichselbaum 343 56gibrambo5770No ratings yet
- J. Biol. Chem.-1933-Somogyi-665-70Document7 pagesJ. Biol. Chem.-1933-Somogyi-665-70gibrambo5770No ratings yet
- J. Biol. Chem.-1938-Somogyi-399-414Document17 pagesJ. Biol. Chem.-1938-Somogyi-399-414gibrambo5770No ratings yet
- J. Biol. Chem.-1933-Somogyi-665-70Document7 pagesJ. Biol. Chem.-1933-Somogyi-665-70gibrambo5770No ratings yet
- J. Biol. Chem.-1931-Somogyi-157-64Document6 pagesJ. Biol. Chem.-1931-Somogyi-157-64gibrambo5770No ratings yet
- By Michael Somogyi. (From The Laboratory The Jewish Hospital of St. Louis, St. Louis.) (Received For Publication, May 16, 1929.)Document9 pagesBy Michael Somogyi. (From The Laboratory The Jewish Hospital of St. Louis, St. Louis.) (Received For Publication, May 16, 1929.)gibrambo5770No ratings yet
- Ulator REV2 USA EXAMPLEDocument35 pagesUlator REV2 USA EXAMPLEMilton UrrozNo ratings yet
- Psyc 331 Exam 2 Study GuideDocument2 pagesPsyc 331 Exam 2 Study GuidedivssssssNo ratings yet
- Smt. B. K. Shah Medical Institute & Research Centre 1st Year Post Graduate Students Record - 2015-2016Document4 pagesSmt. B. K. Shah Medical Institute & Research Centre 1st Year Post Graduate Students Record - 2015-2016TRH RECRUITMENTNo ratings yet
- Goldman-Cecil Medicine 25th 2015Document39 pagesGoldman-Cecil Medicine 25th 2015Dumitru HarsenieNo ratings yet
- Neurology Mnemonics Memory AidsDocument27 pagesNeurology Mnemonics Memory AidsMuhammad Luqman Nul Hakim100% (1)
- A Color Handbook of Skin Diseases of The Dog and Cat, 2nd EditionDocument337 pagesA Color Handbook of Skin Diseases of The Dog and Cat, 2nd EditionHo Duc Tham100% (2)
- Microanatomy of GIT 1Document64 pagesMicroanatomy of GIT 1MEHJABINHAQNo ratings yet
- Hypertension in Pregnancy: Pathophysiology and Treatment: Stephanie Braunthal and Andrei BrateanuDocument15 pagesHypertension in Pregnancy: Pathophysiology and Treatment: Stephanie Braunthal and Andrei BrateanuAini EvellynNo ratings yet
- Reprocessing (Emdr) Terhadap Penurunan Skor Post Traumatic Stress Disorder (PTSD) Akut Pada Pasien PascaDocument13 pagesReprocessing (Emdr) Terhadap Penurunan Skor Post Traumatic Stress Disorder (PTSD) Akut Pada Pasien PascaRismilah MazidaNo ratings yet
- Sindrom AlagileDocument8 pagesSindrom AlagilewenyinriantoNo ratings yet
- CV DR Ari Sami Hussain NadhimDocument5 pagesCV DR Ari Sami Hussain NadhimAri SamiNo ratings yet
- M. Preterm and Postterm - NewDocument92 pagesM. Preterm and Postterm - NewTry Ariditya UtomoNo ratings yet
- Oppenheim J.J., Feldmann M. - Introduction To The Role of Cytokines in Innate Host Defense and Adaptive Immunity (2000) PDFDocument18 pagesOppenheim J.J., Feldmann M. - Introduction To The Role of Cytokines in Innate Host Defense and Adaptive Immunity (2000) PDFHesbon MomanyiNo ratings yet
- Local AnestheticsDocument93 pagesLocal Anestheticsgeetika100% (1)
- TMDDocument170 pagesTMDVinaya Srinivasan100% (2)
- Care of The Older Adult Handouts PrelimsDocument7 pagesCare of The Older Adult Handouts PrelimsAmanda Joy TuizaNo ratings yet
- Pathology REP FinalDocument15 pagesPathology REP Finalswerelloxsthe3rdNo ratings yet
- Werner & Ingbar’s The Thyroid 8th EditionDocument10 pagesWerner & Ingbar’s The Thyroid 8th Editionbyrock66No ratings yet
- Pilonidal SinusDocument3 pagesPilonidal SinusHaddani FozaNo ratings yet
- CAP Diagnosis and TreatmentDocument9 pagesCAP Diagnosis and TreatmentRozecarl JhoyNo ratings yet
- Wound NoteDocument16 pagesWound NoteofasusiNo ratings yet
- DRUG PRESENTATION On Emergency and CPR DrugsDocument39 pagesDRUG PRESENTATION On Emergency and CPR DrugsShibi BennyNo ratings yet
- Impression Techniques For Dental ImplantDocument48 pagesImpression Techniques For Dental ImplantAli AlmakramiNo ratings yet
- Test - Report 24 - 01 - 2022Document3 pagesTest - Report 24 - 01 - 2022Habib Ur RahmanNo ratings yet
- Lung Abscess Bronchoectasis PleurisynDocument19 pagesLung Abscess Bronchoectasis Pleurisynmarco luenaNo ratings yet
- Orthodontic Treatment: Patient Information LeafletDocument2 pagesOrthodontic Treatment: Patient Information LeafletRakan KhtoomNo ratings yet
- Calcanectomy For OsteomyelitisDocument7 pagesCalcanectomy For OsteomyelitisCleff FlowersNo ratings yet
- Everything You Need To Know About AllergiesDocument26 pagesEverything You Need To Know About AllergiesGiuliana FloresNo ratings yet
- Big Pharma's Worst NightmareDocument51 pagesBig Pharma's Worst NightmaredjoleNo ratings yet
- Home remedies for common ailmentsDocument34 pagesHome remedies for common ailmentsBrigitte Nolan100% (3)