You might also like
- Obstetrics History ExampleDocument3 pagesObstetrics History ExampleMohamed Elprince Adel100% (3)
- Strobel e Fey 2018Document18 pagesStrobel e Fey 2018Italo J B DuarteNo ratings yet
- SFATDocument9 pagesSFATKateNo ratings yet
- Insect Bites Stings 11 530kDocument2 pagesInsect Bites Stings 11 530kCM GonzalezNo ratings yet
- LSEBN Burns Blister ManagementDocument1 pageLSEBN Burns Blister ManagementErnesto GuebaraNo ratings yet
- NCM 106 BurnsDocument9 pagesNCM 106 BurnsJudeLaxNo ratings yet
- ToddlerDocument15 pagesToddlerCARL JOHN MANALONo ratings yet
- Burns Assessment - TeachMeSurgeryDocument5 pagesBurns Assessment - TeachMeSurgeryLaroui HoNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
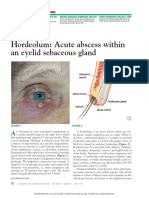
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Evaluation and Management of Sunburn: Roshni PR, Remya Reghu, Meenu Vijayan and Parvati KrishnanDocument4 pagesEvaluation and Management of Sunburn: Roshni PR, Remya Reghu, Meenu Vijayan and Parvati KrishnanMasri RaisNo ratings yet
- Burns 2Document40 pagesBurns 27vjkgkw29xNo ratings yet
- Bioactive Glass Material For Wound Healing BrochureDocument6 pagesBioactive Glass Material For Wound Healing BrochureWahyu Hidayat Bin SidijantoNo ratings yet
- Picu Protocols-Dr - Mohan Shenoy - 2.8.2010Document117 pagesPicu Protocols-Dr - Mohan Shenoy - 2.8.2010Aimhigh_PPMNo ratings yet
- 1 s2.0 S2468912221000316 MainDocument3 pages1 s2.0 S2468912221000316 MainsiskaNo ratings yet
- Maria Angeline Mendoza BSN 3a2 - Communicable Disease StudyDocument17 pagesMaria Angeline Mendoza BSN 3a2 - Communicable Disease StudyAiram Enilegna AzodnemNo ratings yet
- (Edn) Lippincot - BurnsDocument9 pages(Edn) Lippincot - BurnsKimmy NgNo ratings yet
- Burns GuidelineDocument1 pageBurns GuidelineRoi LevinzonNo ratings yet
- Bruise: Wounds and Injuries of The Soft Tissues of The Facial AreaDocument12 pagesBruise: Wounds and Injuries of The Soft Tissues of The Facial AreaCharlene LunaNo ratings yet
- De Bride MentDocument1 pageDe Bride Mentazhar naufaldiNo ratings yet
- FirstAid Poster FinalDocument1 pageFirstAid Poster FinalRECAİ TAŞNo ratings yet
- Mod 7 & 8 Study GuidesDocument11 pagesMod 7 & 8 Study GuidesFerd RuizNo ratings yet
- Burns: ABC of Wound HealingDocument4 pagesBurns: ABC of Wound HealingRuxandra BadiuNo ratings yet
- BURNSDocument4 pagesBURNSAllyssa Leila Estrebillo OrbeNo ratings yet
- Otitis Externa:: BacterialDocument9 pagesOtitis Externa:: BacterialNashat SaadiNo ratings yet
- Bandaging: Saint Paul University ofDocument7 pagesBandaging: Saint Paul University ofjohannah reine buenaflorNo ratings yet
- Principles of Wound Care-Back To The BasicsDocument3 pagesPrinciples of Wound Care-Back To The BasicsKatya LeyNo ratings yet
- Diagnosis and Management of Acute BurnsDocument3 pagesDiagnosis and Management of Acute BurnsDawnNo ratings yet
- Equine Medicine DISEASESDocument14 pagesEquine Medicine DISEASESlowi shooNo ratings yet
- Burn Ulcer Management: Salafudin YusraDocument44 pagesBurn Ulcer Management: Salafudin Yusraarief AnwarNo ratings yet
- Burn Wound CareDocument53 pagesBurn Wound Carenikinikko100% (1)
- Gochi Notes: Immuno-Allergy Part Vi Lecturer: Dra. Eva DizonDocument2 pagesGochi Notes: Immuno-Allergy Part Vi Lecturer: Dra. Eva DizonJustin TayabanNo ratings yet
- 2 4 1-BurnsDocument11 pages2 4 1-BurnsMicaNo ratings yet
- Name of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesDocument2 pagesName of Drug Mechanism of Action Contraindication Side Effects Adverse Effects Nursing ResponsibilitiesMichelle Dona MirallesNo ratings yet
- BurnsDocument5 pagesBurnsdhainey67% (3)
- Burns AssessmentDocument5 pagesBurns AssessmentAnurag BhuyanNo ratings yet
- Case Study BurnDocument3 pagesCase Study BurnInday BebeNo ratings yet
- NCP OrthoDocument7 pagesNCP OrthoShewit AbrahamNo ratings yet
- Msds Addnox FR 910 PTDocument4 pagesMsds Addnox FR 910 PTRajiv DubeyNo ratings yet
- Heridas 20 Cutaneas 20 NEJMDocument11 pagesHeridas 20 Cutaneas 20 NEJMKIM LORIE YAP PASCUALNo ratings yet
- Dengue Leaflet InfoDocument1 pageDengue Leaflet InfoMIJIN BAENo ratings yet
- COMPLICATIONSDocument41 pagesCOMPLICATIONSChethana NagaNo ratings yet
- Primary Care of Ocular Emergencies: Postgraduate MedicineDocument6 pagesPrimary Care of Ocular Emergencies: Postgraduate MedicineAmelia Sotelo RoldanNo ratings yet
- Wa0007.Document6 pagesWa0007.marllyaleja08No ratings yet
- Impaired Skin Integrity Related To Trauma or Infection: ObjectivesDocument5 pagesImpaired Skin Integrity Related To Trauma or Infection: Objectivesmhean azneitaNo ratings yet
- Aubrey Rose A. Vidon BSN 3Y1 - 2Document2 pagesAubrey Rose A. Vidon BSN 3Y1 - 2Aria100% (1)
- Wounds and BleedingDocument3 pagesWounds and BleedingJames Peter FernandezNo ratings yet
- Classification of Wounds: Definition: It Is A Bruise, Usually Produced by AnDocument3 pagesClassification of Wounds: Definition: It Is A Bruise, Usually Produced by AnIvyLove CatalanNo ratings yet
- Tatalaksana Luka Bakar Pada Layanan Primer - FBBDocument31 pagesTatalaksana Luka Bakar Pada Layanan Primer - FBBfebiola sihiteNo ratings yet
- NCP OrthoDocument6 pagesNCP OrthoRuth Anne Arriesgado NañozNo ratings yet
- Disorders of The Integumentary System: Internet ResourcesDocument4 pagesDisorders of The Integumentary System: Internet ResourcesDylan Dela CruzNo ratings yet
- System Disorder ADDocument1 pageSystem Disorder ADSariahNo ratings yet
- Pedia Case 3Document10 pagesPedia Case 3Jona Joyce JunsayNo ratings yet
- Animal Bite Flowchart: Patient Comes in at ER With Animal BiteDocument1 pageAnimal Bite Flowchart: Patient Comes in at ER With Animal BiteJonathan JumalonNo ratings yet
- Elise Tamayo - Infectious Disease PamphletDocument2 pagesElise Tamayo - Infectious Disease Pamphletapi-550823265No ratings yet
- ImportantDocument21 pagesImportantGaurav pareekNo ratings yet
- BURNSDocument26 pagesBURNSGaurav pareekNo ratings yet
- Reviewer in Physical Agents and Electrotherapy: Pagod Na Di Alam Kung BaketDocument8 pagesReviewer in Physical Agents and Electrotherapy: Pagod Na Di Alam Kung Baketrr4fgws945No ratings yet
- A. Diagram: Ii. Pathophysiology and ManagementDocument1 pageA. Diagram: Ii. Pathophysiology and ManagementgiaNo ratings yet
- 12b. Burns Injury (Russells Hall Hospital, UPDATED Mar 2012)Document11 pages12b. Burns Injury (Russells Hall Hospital, UPDATED Mar 2012)akshayNo ratings yet
- Guidelines For Measles SIA 2011 CambodiaDocument24 pagesGuidelines For Measles SIA 2011 CambodiaPrabir Kumar ChatterjeeNo ratings yet
- RC Workholism JCDocument4 pagesRC Workholism JCJean Carlos CastilloNo ratings yet
- Case Study For MCNDocument2 pagesCase Study For MCNchloeNo ratings yet
- Muscle Mass in 5 Weeks - Gain Le - John KempfDocument130 pagesMuscle Mass in 5 Weeks - Gain Le - John KempfVy TrieuNo ratings yet
- Amito Tiny Houses: 2 Mid Assignment Entrepreneurship (Bum-Cc-322)Document10 pagesAmito Tiny Houses: 2 Mid Assignment Entrepreneurship (Bum-Cc-322)Amit YadavNo ratings yet
- CSYah Tambo 2018 JIPHDocument12 pagesCSYah Tambo 2018 JIPHadhiniNo ratings yet
- Chapter 2 Emergency Help: Form 4 ScienceDocument1 pageChapter 2 Emergency Help: Form 4 ScienceWani MesraNo ratings yet
- Solis Surgical Wound Classification PDFDocument35 pagesSolis Surgical Wound Classification PDFDon RicaforteNo ratings yet
- Factors That Contribute Depression Among Grade 10 of Iligan City National High SchoolDocument52 pagesFactors That Contribute Depression Among Grade 10 of Iligan City National High SchoolPiyang BeaumNo ratings yet
- Dried Ivy Leaf ExtractDocument3 pagesDried Ivy Leaf Extractfauzan26No ratings yet
- Positive Health': A New, Dynamic Concept of HealthDocument47 pagesPositive Health': A New, Dynamic Concept of Healthmert05No ratings yet
- Age-Related Hyperkyphosis Its Causes, Consequences, and ManagementDocument19 pagesAge-Related Hyperkyphosis Its Causes, Consequences, and ManagementshivnairNo ratings yet
- Lucban ES, Report On Children Month CelebrationDocument13 pagesLucban ES, Report On Children Month CelebrationRitchelle PerochoNo ratings yet
- GAIN Report ThailandDocument45 pagesGAIN Report ThailandWarrenNo ratings yet
- CV - Chandra Mohan GuptaDocument4 pagesCV - Chandra Mohan GuptavarunNo ratings yet
- The Holmes Life: Rahe InventoryDocument1 pageThe Holmes Life: Rahe InventoryAkhwand SaulatNo ratings yet
- Medical Billing Questions 1Document7 pagesMedical Billing Questions 1framar572112100% (1)
- Test Bank HemaDocument72 pagesTest Bank HemaDesiree ArquisolaNo ratings yet
- WHW News Edition 1, 2014Document20 pagesWHW News Edition 1, 2014Women's Health WestNo ratings yet
- Unlocking The Prediction of Preeclampsia, A Widespread, Life-Threatening Pregnancy ComplicationDocument5 pagesUnlocking The Prediction of Preeclampsia, A Widespread, Life-Threatening Pregnancy ComplicationImam SantosoNo ratings yet
- Medication Guide Mefloquine Hydrochloride Tablets USP Medication Guide Mefloquine Hydrochloride Tablets USPDocument4 pagesMedication Guide Mefloquine Hydrochloride Tablets USP Medication Guide Mefloquine Hydrochloride Tablets USPConio CarrasNo ratings yet
- Piriformis SyndromeDocument6 pagesPiriformis SyndromeChân Mệnh Thiên TửNo ratings yet
- Keperawatan Bencana Jurnal 3Document14 pagesKeperawatan Bencana Jurnal 3Fitriani HanifahNo ratings yet
- Advanced Fitness Assessment and Exercise Prescription 8Th Edition Version Full Chapter PDFDocument53 pagesAdvanced Fitness Assessment and Exercise Prescription 8Th Edition Version Full Chapter PDFsapitonuk100% (6)
- Bob Stahl PHD, Elisha Goldstein PHD, Saki Santorelli EdD MA, Jon Kabat-Zinn PHD - A Mindfulness-Based Stress Reduction Workbook-New Harbinger Publications (2010)Document332 pagesBob Stahl PHD, Elisha Goldstein PHD, Saki Santorelli EdD MA, Jon Kabat-Zinn PHD - A Mindfulness-Based Stress Reduction Workbook-New Harbinger Publications (2010)cristina100% (2)
- Five Clinical Studies Demonstrate The Effectiveness of Flower Essence Therapy in The Treatment of Depression AutorDocument18 pagesFive Clinical Studies Demonstrate The Effectiveness of Flower Essence Therapy in The Treatment of Depression AutorSIVAKRISHNAN.RNo ratings yet
- Tongue DisordersDocument31 pagesTongue DisordersMaphoto Xola0% (1)
- Adriani Pemicu 4 KGDDocument196 pagesAdriani Pemicu 4 KGDSelly HerliaNo ratings yet
- Lung CancerDocument12 pagesLung CancerАнастасия ОстапенкоNo ratings yet