You might also like
- Map Arataki Waitakere Ranges Regional ParkDocument1 pageMap Arataki Waitakere Ranges Regional ParkFlorence NightingleNo ratings yet
- Map Arataki Waitakere Ranges Regional ParkDocument1 pageMap Arataki Waitakere Ranges Regional ParkFlorence NightingleNo ratings yet
- Auckland Council Bookable Site Map Locality GuideDocument1 pageAuckland Council Bookable Site Map Locality GuideFlorence NightingleNo ratings yet
- Reading and Numeracy Assessment ResultsDocument4 pagesReading and Numeracy Assessment ResultsGillian Bollozos-CabuguasNo ratings yet
- NEO System DiagnosisDocument30 pagesNEO System DiagnosisbljNo ratings yet
- How To ReadDocument32 pagesHow To ReadjorgeluiztadeurodriguesfilhoNo ratings yet
- En8Rc-Iia-2.22:: Table of Specification English 8Document1 pageEn8Rc-Iia-2.22:: Table of Specification English 8Kristina De los ReyesNo ratings yet
- Qdoc - Tips Transformer Foundation DesignDocument13 pagesQdoc - Tips Transformer Foundation DesignabguyNo ratings yet
- Flood MapsDocument3 pagesFlood MapsBayAreaNewsGroup100% (2)
- 1 - MDR Submission 2015 - 2nd Half-ProjectDocument2 pages1 - MDR Submission 2015 - 2nd Half-ProjectfizanlaminNo ratings yet
- DHR Brochure PDFDocument23 pagesDHR Brochure PDFDoloritasNo ratings yet
- Discovery Hybrid RheometerDocument23 pagesDiscovery Hybrid RheometernilavanmuthuNo ratings yet
- Eighty Eight Project BrochureDocument21 pagesEighty Eight Project Brochure92km7jw9k5No ratings yet
- Resistance Projection Welding Process GuideDocument9 pagesResistance Projection Welding Process GuideAlexandre GoulartNo ratings yet
- 5666658521d36 HSSECompetencymatrixDocument1 page5666658521d36 HSSECompetencymatrixSaran rasayaNo ratings yet
- 2017 Generic Drill Yearly Check ListDocument2 pages2017 Generic Drill Yearly Check ListCogbillConstructionNo ratings yet
- Set The Roads On FireDocument5 pagesSet The Roads On FirePraveen SakrappanavarNo ratings yet
- Complete Green Item FileDocument196 pagesComplete Green Item FileExecutive Computer ProductsNo ratings yet
- Clear Mutual Expectations RefresherDocument10 pagesClear Mutual Expectations RefresherInstalasi RehabilitasiNo ratings yet
- Oracle BI Publisher 11g R1 Fundamentals (Student Guide - Volume I) (101-200) PDFDocument100 pagesOracle BI Publisher 11g R1 Fundamentals (Student Guide - Volume I) (101-200) PDFangel_ceruz20No ratings yet
- SampleDocument13 pagesSampleLuiz FabricioNo ratings yet
- Bunn VPR Parts ManualDocument26 pagesBunn VPR Parts Manualsatx840No ratings yet
- M U4 PioneerTrailsDocument1 pageM U4 PioneerTrailsmrtalmadgeNo ratings yet
- FMO ESG Toolkit (AutoRecovered)Document149 pagesFMO ESG Toolkit (AutoRecovered)me.abhishekpNo ratings yet
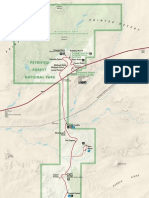
- Petrified Forest NPDocument1 pagePetrified Forest NPapi-19487128No ratings yet
- The Church of the Unveiled SpringDocument1 pageThe Church of the Unveiled SpringMarkus WallNo ratings yet
- Wire Rope 2019 PDFDocument22 pagesWire Rope 2019 PDFkarthikNo ratings yet
- Bhavarthabodhini TikaDocument1,018 pagesBhavarthabodhini Tikajainendra08No ratings yet
- 4 4packetDocument4 pages4 4packetapi-327561261No ratings yet
- Jaz TT Cup Knotted BrushDocument9 pagesJaz TT Cup Knotted BrushGianfranco CopelloNo ratings yet
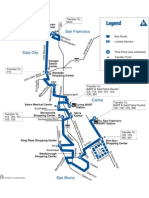
- Route 122 8 22 04 MAPDocument1 pageRoute 122 8 22 04 MAPJason BentleyNo ratings yet
- MMPI2 RFOverview Mini MNL HQDocument11 pagesMMPI2 RFOverview Mini MNL HQMaham Fatima0% (1)
- Wire Rope and SlingsDocument22 pagesWire Rope and Slingsmou mouNo ratings yet
- Buffalo Mt. Drive Detour MapDocument1 pageBuffalo Mt. Drive Detour MapsummitdailyNo ratings yet
- Centennial Review: The Battle: Free Enterprise vs. Big GovernmentDocument4 pagesCentennial Review: The Battle: Free Enterprise vs. Big GovernmentColorado Christian UniversityNo ratings yet
- Healing Lyme: Buhner Core Protocol (Unofficial) PDFDocument4 pagesHealing Lyme: Buhner Core Protocol (Unofficial) PDFSteluța DrâmbuNo ratings yet
- DHR BrochureDocument23 pagesDHR BrochureDung ChuNo ratings yet
- Ewd 43Document4 pagesEwd 43Antonio GomezNo ratings yet
- The Trojan Reach Sector MapDocument1 pageThe Trojan Reach Sector MapLorenzo AngellaNo ratings yet
- Mahindra Mahindra Brochure1046Document5 pagesMahindra Mahindra Brochure1046Ankur MestryNo ratings yet
- ParentnecinfographicDocument1 pageParentnecinfographicapi-510754135No ratings yet
- Proyecto 2Document9 pagesProyecto 2DIANA PAOLA CHAVEZ RISCONo ratings yet
- Gurgaon MasterplanDocument1 pageGurgaon MasterplanRishabh InvestorclinicNo ratings yet
- Secondary Compartmental-cum-Special Result 2023Document1 pageSecondary Compartmental-cum-Special Result 2023gaurav9709602147No ratings yet
- Sample Application: Bug Status CountDocument21 pagesSample Application: Bug Status CountMukul TanejaNo ratings yet
- D80149GC11 sg1 PDFDocument340 pagesD80149GC11 sg1 PDFNestor Torres PachecoNo ratings yet
- YogSandesh May Eng2011Document66 pagesYogSandesh May Eng2011Manmohan GuptaNo ratings yet
- Construction SiteDocument1 pageConstruction SiteAndrei CristianNo ratings yet
- Ewd 16Document20 pagesEwd 16Antonio GomezNo ratings yet
- Ryde City Hub design philosophyDocument6 pagesRyde City Hub design philosophyarch232No ratings yet
- 6 Steps of HealingDocument1 page6 Steps of HealingjunekarlaleeNo ratings yet
- Student FlyerDocument1 pageStudent FlyerKrishna HaraleNo ratings yet
- Winter 2021 Program Application: DeadlineDocument3 pagesWinter 2021 Program Application: DeadlineDobler LilianaNo ratings yet
- Toronto FUN Guide Spring / Summer 2009 (Swimming, North York District)Document24 pagesToronto FUN Guide Spring / Summer 2009 (Swimming, North York District)KidsEnergyBurner100% (2)
- Advanced Photoshop Issue 060Document88 pagesAdvanced Photoshop Issue 060Dipesh Bardolia0% (1)
- VW 6 Speed Automatic Transmission 09G Repair Manual Edition 07.2015 D3E8001EAACDocument167 pagesVW 6 Speed Automatic Transmission 09G Repair Manual Edition 07.2015 D3E8001EAACAlexandre Loreto100% (1)
- VW 6 Speed Automatic Transmission 09g Repair Manual Edition 072015 D3e8001eaac PDFDocument167 pagesVW 6 Speed Automatic Transmission 09g Repair Manual Edition 072015 D3e8001eaac PDFSebastian Gomez Gomez100% (1)
- Lesson 7-Session Border Controller ConceptsDocument76 pagesLesson 7-Session Border Controller ConceptsBikash DashNo ratings yet
- OPUS Clinician Survey (2014)Document2 pagesOPUS Clinician Survey (2014)hasselNo ratings yet
- Laboratory Information SystemDocument3 pagesLaboratory Information SystemhasselNo ratings yet
- OPUS UP Scoring Guide 6 June 2016Document4 pagesOPUS UP Scoring Guide 6 June 2016hasselNo ratings yet
- Opus Hqol Status (2014)Document2 pagesOpus Hqol Status (2014)hasselNo ratings yet
- Opus Le Functional Status (2014)Document1 pageOpus Le Functional Status (2014)hasselNo ratings yet
- OPUS Upper Extremity Functional StatusDocument2 pagesOPUS Upper Extremity Functional StatushasselNo ratings yet
- Lecture 3.2.3: Erection III: Steel Construction: Fabrication and ErectionDocument4 pagesLecture 3.2.3: Erection III: Steel Construction: Fabrication and ErectionMihajloDjurdjevicNo ratings yet
- ORGB 5th Edition Nelson Solutions Manual 1Document44 pagesORGB 5th Edition Nelson Solutions Manual 1shirley100% (52)
- Professional Teachers (Secondary) 10-2022 FilipinoDocument26 pagesProfessional Teachers (Secondary) 10-2022 FilipinoPRC Baguio100% (1)
- ELMO-T3 Operation - E - 55Document34 pagesELMO-T3 Operation - E - 55nguyen minhNo ratings yet
- Operacion y Mantenimiento Stacker PDFDocument1,146 pagesOperacion y Mantenimiento Stacker PDFjhon omarNo ratings yet
- CHN DrugstudyDocument2 pagesCHN DrugstudyNathalie OmalNo ratings yet
- Defences in Therapy Steele MosqueraDocument16 pagesDefences in Therapy Steele MosqueraOyrania AndreopoulouNo ratings yet
- Townsend 1979Document28 pagesTownsend 1979api-534238122No ratings yet
- Hemodynamic Effects of Dexmedetomidine vs ClonidineDocument12 pagesHemodynamic Effects of Dexmedetomidine vs ClonidinezzzzNo ratings yet
- Nurses' disaster response competencies at health centers in Bireuen District, AcehDocument15 pagesNurses' disaster response competencies at health centers in Bireuen District, AcehWahyu HidayatiNo ratings yet
- Aromasin 25 MG Coated Tablets SMPCDocument9 pagesAromasin 25 MG Coated Tablets SMPCpedjaljubaNo ratings yet
- Process Recording - SampleDocument3 pagesProcess Recording - SampleMara Magsanoc70% (10)
- Trainee's Record Book SWBLDocument12 pagesTrainee's Record Book SWBLaaronjules100% (2)
- 02 Id Ego and Super EgoDocument11 pages02 Id Ego and Super EgoEmraan MalikNo ratings yet
- 18.20.04 - BSSL Seafarers Health Self Declaration With COVID 19 Test And... (1) - 3Document3 pages18.20.04 - BSSL Seafarers Health Self Declaration With COVID 19 Test And... (1) - 3Dean IL RE JamesNo ratings yet
- Fatigue Management Report Template-CompletedDocument4 pagesFatigue Management Report Template-CompletedAbdullah100% (1)
- Pestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementDocument15 pagesPestle Analysis On Reliance Industries: MBA Student - DBS Module International ManagementshubhamNo ratings yet
- Medical Checkup PackagesDocument2 pagesMedical Checkup PackagesLia AnggitaNo ratings yet
- Safety Data Sheet: Butyrylcholinesterase Inhibitor Screening Kit (Colorimetric)Document6 pagesSafety Data Sheet: Butyrylcholinesterase Inhibitor Screening Kit (Colorimetric)Verliyanti BastariNo ratings yet
- Flow Penanganan DeviasiDocument4 pagesFlow Penanganan DeviasiGaluhNo ratings yet
- LP Trauma Kapitis PDFDocument29 pagesLP Trauma Kapitis PDFPajoNo ratings yet
- H2S Monitor Manual - Tango TX1Document50 pagesH2S Monitor Manual - Tango TX1MattNo ratings yet
- Clinical Handbook of Psychotropic Drugs, 25e (May 8, 2023)_(0889376328)_(Hogrefe Publishing) ( Etc.) (Z-Library)Document555 pagesClinical Handbook of Psychotropic Drugs, 25e (May 8, 2023)_(0889376328)_(Hogrefe Publishing) ( Etc.) (Z-Library)Dragutin PetrićNo ratings yet
- CONCRETING TITLEDocument5 pagesCONCRETING TITLEChristian Bulaong100% (1)
- Charity Marathon Risk AssessmentDocument9 pagesCharity Marathon Risk Assessmentamarnadh100% (1)
- Role Play Script BHS INGGRISDocument6 pagesRole Play Script BHS INGGRISardiyantiNo ratings yet
- Course Outline PBH 101 MW 18Document7 pagesCourse Outline PBH 101 MW 18FAYAZ AHMEDNo ratings yet
- Uts ReadingDocument7 pagesUts ReadingLaisah IdrNo ratings yet
- JIDMR SCOPUS Ke 4 Anwar MallongiDocument4 pagesJIDMR SCOPUS Ke 4 Anwar Mallongiadhe yuniarNo ratings yet
- Treatment Plan PortfolioDocument2 pagesTreatment Plan Portfolioapi-518560779No ratings yet